In a nutshell
GiveWell believes that distributing insecticide-treated nets (ITNs) is one of the most cost-effective programs that donors can support. We estimate that it costs approximately $3,000 to $8,000 to avert a death in locations where GiveWell supports campaigns. We think mass distribution of ITNs is cost-effective because:
- Malaria is a major cause of child mortality in locations where GiveWell funds campaigns
- ITNs provide substantial protection from malaria (we estimate using an ITN reduces malaria mortality by approximately 40 to 55%, varying by location).
- ITNs are relatively cheap.
- Averting malaria probably provides substantial additional benefits like increased income later in life.
GiveWell’s current top recommended organization for ITN distributions is Against Malaria Foundation. Our page on the Against Malaria Foundation is available here and our cost-effectiveness analysis is here.
Published: December 2023; Last updated: April 2024 (Previous versions of this page: 2021 report, 2018 report, 2015 report, 2014 report, 2012 report, 2011 report, 2009 report)
Summary
Basics
Insecticide-treated nets (ITNs) are nets that have been treated with insecticide to deter and kill the mosquitoes that transmit malaria. They are typically hung over beds to provide protection during sleep. GiveWell has mainly funded ITN distributions through the Against Malaria Foundation (AMF). AMF uses GiveWell funding to buy nets and other partners fund the cost of distributing them. AMF’s nets are distributed in mass campaigns run by countries’ national malaria programs. (More)
How cost-effective is it?
As of December 2023, we estimate that it costs approximately $3,000 to $8,000 (varying by location) to avert a death in areas where GiveWell supports campaigns. This equates to being 9x to 23x as cost-effective as spending on unconditional cash transfers (GiveWell’s benchmark for comparing different programs).
We think that mass distribution of nets is cost-effective because:
- Malaria is a major cause of child deaths in areas where GiveWell funds campaigns. Our estimate of the mortality rate attributable to malaria is around 0.3% to 0.9% per child per year (varying by location). We rely primarily on malaria-specific mortality estimates from the Global Burden of Disease (GBD) Model (more). We also assume that for each malaria death, an additional 0.75 deaths attributed to another cause by the GBD are indirectly caused by malaria. This is based on evidence that malaria control programs often have larger impacts on mortality than would be expected from their impact on malaria alone (more). These estimates are broadly in line with our impression that malaria is widely seen as one of the main causes of child mortality in sub-Saharan Africa.
- ITNs provide significant protection against malaria. Our impression is that there is widespread agreement in the global health community that ITNs are an important malaria prevention tool. We estimate that sleeping under nets reduces malaria mortality by around 40% to 55% in locations where GiveWell fund campaigns. This is based on a meta-analysis of randomized controlled trials (RCTs), which estimates that distributing ITNs reduces malaria cases by 45% (more). We then apply various adjustments including an adjustment for insecticide resistance. Although insecticide resistance has become significantly more widespread since these studies were conducted, new types of nets to counteract resistance have been developed too. We currently estimate that resistance reduces the effectiveness of nets by roughly 5% to 30%, depending on the location and the mix of nets used (more).
- We think that each ITN provides effective protection for around two years in most countries. This is based on studies that tracked retention and physical durability of ITNs in real-life conditions. (More)
- ITNs probably provide significant benefits beyond averting child mortality. In particular, we think that ITNs, by averting malaria during a sensitive period of childhood development, could improve long-run outcomes. This is based on two studies that find historical malaria eradication campaigns led to long-term increases in income. We use a combined estimate from these studies and cross reference it against other child health programs that we think lead to income effects (e.g., deworming, iron fortification). We discount the combined estimate from the malaria eradication studies by 70% to reflect our uncertainty about the quality of this evidence. Even with this discount, we estimate that ~25% to ~40% of the total modeled benefits of the program come from increased income rather than averted deaths. (More)
- It is relatively cheap to reach people with ITNs. Intuitively, this is because nets are inexpensive to purchase and each net provides protection for at least a year. We estimate that it costs ~$4 to ~$6 to deliver each net to a household, based on forward-looking projections from AMF on their costs to purchase each net, the costs to distribute nets, and estimates of the proportion of nets purchased but not distributed from previous campaigns (although we have very little information on these) (more). To estimate the cost per additional child under five reached, we estimate 63% of delivered nets are used (more), each net protects around two people on average (more), and roughly 15% to 20% of people sleeping under nets are children under 5 (more). This results in an estimate that it costs approximately $20 to $25 for one additional child under age five to sleep under a net. (More)
- Without GiveWell funding, fewer children would have access to ITNs:
- Without campaigns, people would be unlikely to access ITNs. Our understanding is that these campaigns are the main way people access ITNs in malaria-endemic countries. We think that relatively few people would access nets through other sources, such as “continuous distribution” of nets (which only targets certain groups and we think is underfunded in most countries), or purchasing nets on their own. We currently assume that people are equally likely to obtain nets from other sources as they were in the original studies measuring the impacts of ITNs on mortality (i.e., roughly 5% to 10% of people would get nets in the absence of campaigns). (More)
- Without our funding, campaigns would be unlikely to occur. AMF works in countries that don't have enough money from the other big funders of net campaigns (the Global Fund and President’s Malaria Initiative) to pay for high-quality mass campaigns (i.e., those that occur at least every three years, achieve a high degree of coverage, and distribute nets that are effective given local resistance profiles). We currently estimate that there is a 20% to 60% chance that other funders would replace GiveWell’s ITN funding in our absence (depending on the specific country and campaign). Our adjustment for “diverting other actors spending away from net campaigns” lowers cost-effectiveness by approximately 15% to 40% depending on the location. This is high relative to some other programs we fund, but we think ITNs are still a good investment even after accounting for this. (More)
We quantify these arguments using a cost-effectiveness analysis, which allows us to compare across different programs. Here is a sketch, using estimates for one country, Uganda, as an example.
| What we are estimating | Best guess (rounded) | Confidence intervals
(25th - 75th percentile) (more) |
Implied cost-effectiveness
(in multiples of direct cash transfers) |
|---|---|---|---|
| Grant amount (arbitrary value) | $1,000,000 | ||
| Child mortality benefits | |||
| Cost per additional child under 5 sleeping under a net (more) | $22.15 | $19 - $30 | 18x - 11x |
| Number of additional children under 5 receiving nets as a result of this grant (more) | ~45,000 | ||
| Years of effective protection provided by each net (more) | 2 | 1.5 - 2.3 | 12x - 18x |
| Annual mortality rate from malaria and associated causes among children without access to nets (more) | 0.64% | 0.3% - 0.9% | 8x - 21x |
| Reduction in malaria mortality per year of protection from nets (more) | 51% | 45% - 58% | 14x - 17x |
| Initial cost-effectiveness estimate | |||
| Initial cost per death averted | ~$3,400 | ||
| Moral weight for each under-5 death averted (more) | 116 | ||
|
Initial cost-effectiveness estimate
|
10x | ||
| Summary of primary benefits (% of modeled benefits) | |||
| Reduced mortality among children under 5 (more) | 59% | ||
| Reduced mortality among older children and adults (more) | 9% | 6% - 14% | 15x - 17x |
|
Income increases in later life (more)
|
32% | 19% - 42% | 13x - 18x |
|
Additional adjustments
|
|||
| Adjustment for additional program benefits and downsides (more) | 38% | 26% - 51% | 14x - 17x |
| Supplemental grantee-level adjustments (more) | -4% | -20% - -2% | 13x - 16x |
| Adjustment for diverting other actors’ spending into net campaigns (more) | -0.19% | ||
| Adjustment for diverting other actors’ spending away from net campaigns (more) | -32% | -58% - -14% | 10x - 20x |
| Final cost-effectiveness
(multiples of cash transfers) |
15.5x | ||
| Final cost per death averted (see here) | ~$5,000 | ||
We’ve also considered other perspectives that we think might not be captured explicitly in these cost-effectiveness estimates (e.g., whether experts see ITNs as a good investment). Overall, we don’t think any of these alternative perspectives undermine the case for ITNs. But we have spent considerably less time and effort engaging with these questions than we have on our main cost-effectiveness model. We hope to spend more time on these questions in the future. (More)
How could we be wrong?
- How many nets purchased with GiveWell funding are distributed and used? Our estimates of the number of people reached with nets are based on a number of uncertain factors. These include:
- The share of purchased nets distributed: As part of our cost per net analysis, we rely on data shared by AMF on the proportion of ITNs that it purchased but were not distributed in each campaign (from around 2% to 10% across countries). We haven't yet reviewed the methodology used to collect this data in detail. One thing that would increase our confidence in this data is cross-checking it against independent sources to understand how far GiveWell-funded campaigns increased the proportion of people with access to ITNs. As of the time of writing, we have started but not yet finalized or published this work. (More)
- The share of distributed nets that are used: We estimate that 63% of distributed nets are used. This is a rough estimate, and we haven’t cross-checked this against recent, independent survey data. We also use the simplifying assumption that net usage is the same across countries, which we think is unlikely to be correct. (More)
- Would other ways of funding nets be effective? To date, GiveWell has only funded ITNs through mass campaigns. The large majority of our funding for nets has also gone to one organization (AMF). It might be that we’re missing other effective ways of funding nets. This could include continuous distribution of nets (e.g., in schools and routine healthcare appointments), “market shaping” interventions to increase net supply/reduce net price, or by funding other organizations. (More)
- How long do nets provide protection? We have not recently updated our analysis of net durability, and some aspects may be out of date. In particular, we currently assume that next-generation ITNs (containing additives designed to mitigate insecticide resistance) provide protection for the same length of time as standard ITNs. We haven’t yet investigated this question in depth and we’ve seen some evidence suggesting it is wrong. Our 25th to 75th percentile confidence interval for how long nets provide effective protection is 1.5 to 2.3 years in Uganda, implying a cost-effectiveness that net distributions are 12 to 18 times as cost-effective as direct cash transfers (“12x to 18x”). (More)
- How big a concern is insecticide resistance? We currently account for increasing resistance to pyrethroids, the main chemical used in ITNs, with a -4% to -33% adjustment to net effectiveness, depending on the location and mix of nets used. We are uncertain about a number of aspects of our analysis including the level of increase in pyrethroid resistance over time. We’ve also not completed or published our analysis of chlorfenapyr nets, the type of next-generation ITN that we expect to be most promising, but we hope to update this in the future. (More)
- Would people access nets from other sources without GiveWell funding for ITN campaigns? This could happen if:
- People would access nets from other sources in the absence of campaigns. Our cost-effectiveness analysis currently assumes approximately 5% to 10% of households would access ITNs if campaigns didn’t occur. It’s possible this is inaccurate, and we have not tried to estimate this empirically. We plan to look at this question in more detail in the future. (More)
- Other funders would replace GiveWell funding for ITN campaigns in our absence. The funding landscape for malaria programs is fairly crowded. We think there’s a chance that other funders would replace GiveWell’s campaign funding in our absence. We are also uncertain about whether our funding will create an expectation of continued funding and reduce other funders’ future spending on ITNs. Our current adjustment for other actors’ spending, which attempts to account for this factor, decreases impact by ~32% in Uganda, and our 25th to 75th percentile confidence interval for this adjustment is -58% to -14%, which implies a cost-effectiveness of 10x to 20x. We hope to improve our estimates on this question in the future by investigating whether funding gaps that we didn’t fill were covered by other funders, but we haven’t conducted this analysis systematically yet. (More)
- Will nets remain impactful in the future? We’re unsure if changes in the malaria landscape will make nets less cost-effective in the future. Trends that we think could have an impact are the malaria vaccine rollout (which is likely to mean falling overall malaria burden) and the possible development of resistance to next-generation nets (which could make nets less effective at averting malaria). (More)
-
How much do nets increase income in later life? The effect of ITNs on income in later life accounts for ~25% to ~40% of the benefits in our model (depending on the location). We are nervous about these effects constituting such a high share of the benefit, given the evidence for them is speculative and uncertain. Our 25th to 75th percentile confidence interval is that income effects account for 19% to 42% of our total modeled benefits in Uganda, implying a cost-effectiveness of 13x to 18x. We’re aware of further research on long-run income effects of other health interventions, such as vaccines, that we could use to check our estimates, but we haven’t done this work yet. (More)
- How many deaths are caused by malaria? Record keeping on the causes of mortality in malaria-endemic countries is not reliable. Our analysis relies on malaria mortality estimates from the Global Burden of Disease Project, and we’re unsure how accurate they are (more). We also adjust these estimates by assuming that malaria contributes to 0.75 deaths from other causes for each death attributed directly to malaria. This is a highly uncertain best guess (more). Our 25th to 75th percentile confidence interval for mortality caused by malaria in Uganda is 0.3% to 0.9%, which implies a cost-effectiveness of 8x to 21x.
- How accurate was our analysis of nets in hindsight? GiveWell’s cost-effectiveness analyses are “forward-looking” and aim to predict the impact a program will have at the time we make a grant decision. We have paid less attention to backwards checks to understand how accurate the predictions in our ITN grants were. This is a weakness in our approach and something we aim to improve in the future. (More)
Note: The figures in this report are from our December 2023 cost-effectiveness analysis. Our estimates change over time as we gather new information and update our analysis, and so the numbers in this report may not exactly match those in our most recent cost-effectiveness analysis (available here).
GiveWell’s current top recommended organization for ITN distributions is Against Malaria Foundation. Our page on the Against Malaria Foundation is available here.
1. The basics of the program
1.1 What is malaria and what are its impacts?
Malaria is a disease caused by Plasmodium parasites which are transmitted to people through the bites of infected mosquitoes.1 Symptomatic cases involve flu-like symptoms including fever, which can progress to severe illness or death.2 Some groups are at particularly high risk of severe symptoms including infants, children under five years of age, pregnant women, travelers, and people with HIV or AIDS.3
The World Health Organization (WHO) estimates that malaria deaths fell from 897,000 in 2000 to 619,000 in 2021.4 Globally, there were an estimated 249 million malaria cases in 2022.5 The WHO African Region carries a disproportionately high share of the malaria burden. In 2021, the region accounted for 94% of all malaria cases and 95% of deaths.6
1.2 What are ITNs?
An insecticide-treated net (ITN) is a net (usually a bed net) which has been treated with insecticide to kill and repel the mosquitoes that carry malaria.7 Long-lasting insecticidal nets (LLINs) are factory-treated ITNs made of material into which insecticide is incorporated or bound around the fibers. To be categorized as long-lasting by WHO, ITNs must remain effective after 20 washes in lab conditions and for three years in real-world conditions.8
ITN distribution is one of two main WHO-recommended strategies for malaria vector control.9 WHO recommends that ITNs be distributed for free for those at risk for malaria (one for every 1.8 people in the target population).10
- Nets containing a pyrethroid and an additive called piperonyl butoxide (PBO) designed to enhance the effect of the pyrethroid (recommended since 2017).11
- Nets containing a pyrethroid and an additional insecticide, chlorfenapyr (recommended since 2023).12
- Nets containing a pyrethroid and an insecticide growth regulator, pyriproxyfen, designed to disrupt mosquito growth and reproduction (recommended since 2023).13
1.3 How do ITN distributions work?
ITNs are typically distributed through mass campaigns and "continuous distribution" channels.16
- Mass campaigns involve large-scale distribution to households, either door-to-door or through central distribution sites in a community. In most cases, WHO recommends an interval of three years between campaigns.17
- Continuous distribution involves ongoing distribution during other touchpoints that people may have with the state or healthcare system. Settings where people can access nets via continuous distribution include antenatal clinics, immunization clinics, and schools.18
2. How GiveWell estimates cost-effectiveness
GiveWell recommends programs that we believe save or improve lives as much as possible for as little money as possible. To estimate this, we produce a cost-effectiveness analysis (“CEA”) which aims to produce a best guess of the overall impact of a program per dollar donated.
We use "moral weights" to quantify the benefits of different impacts a program may have (e.g., increased income vs reduced deaths). We benchmark to a value of 1, which we define as the value of doubling someone’s consumption for one year. The main moral weights we use for our analysis of malaria nets are in the table below.
| Benefit | Moral weight (units of value per outcome) |
|---|---|
| Doubling consumption for one person for one year | 1 |
| Value of increased income through averting a case of malaria in a person under age 15 with ITNs | 0.23 |
| Averting the death of a child under five from malaria | 116 |
| Averting the death of someone aged over five from malaria | 73 |
For more about how GiveWell thinks about cost-effectiveness, see our discussion on this page.
3. How many people do net campaigns reach?
3.1 Summary
The starting point for our analysis is the number of people who will be protected with nets per $1 million in AMF spending.25 We estimate that each $1 million spent leads to ~38,000 to ~56,000 children under 5 sleeping under nets (varying by country).26 We also estimate that each net provides protection for 1.2 to 2 years.27 A summary is below, using one country (Uganda) as an example:
| What we are estimating | Value |
|---|---|
| Donation to Against Malaria Foundation (AMF) (arbitrary value) | $1,000,000 |
| Cost per net distributed, excluding in-kind government costs (more) | $4.25 |
| Proportion of nets used (more) | 63% |
| People sleeping under each net (more) | 1.8 |
| % of population under age five (more) | 17% |
| Subtotal: Cost per child under five sleeping under a net | $22.15 |
| Subtotal: Number of children under five sleeping under a net per year per $1m spent | ~45,000 |
| Years of effective coverage provided by each net (more) | 2 |
| Total (overall number of children under five protected for one year) | ~89,000 |
- We’re unsure how many nets funded by GiveWell are purchased but not distributed. We have begun the process of cross checking our analysis against independent surveys, but have not completed or published this work yet (more).
- We are unsure how long each net provides effective protection. Our analysis relies on a number of uncertain assumptions including how durability varies between net types and across locations (more).
- We use the simplifying assumption that net usage is the same across locations. This is unlikely to be accurate, since net usage may vary depending on climate, cultural norms, and other factors (more).
- We have not deeply investigated how many people can acquire nets from non-campaign sources, and we think we could be underestimating this (implying we’re overestimating cost-effectiveness) (more).
3.2 How much does each net cost?
Summary
As of December 2023, we estimate that it costs approximately $4 to $6 (varying by location) to distribute one net in an AMF-supported program.28 In Uganda, our estimate is $4.45.
Unlike most of our analysis, our estimates of cost per net are unpublished and we do not break down our calculations in detail in this report. This is because we have not received permission to publish country-specific cost estimates we received from the Global Fund or AMF’s projections for the costs it expects to pay to procure each net by country and net type, which our calculations rely on. AMF notes that, while they would like to allow the publishing of net costs, in keeping with their approach to transparency, doing so has the risk of compromising sensitive net price negotiations with manufacturers.29
Our approach
We calculate the cost per net distributed in each country based on the following estimates:
- Estimates of the costs that AMF expects to pay to purchase each net in the future (at the time we made our most recent grant). We adjust these to account for the proportion of nets that are purchased but not delivered, based on estimates from previous campaigns. Averaging across countries and net types, this accounts for 52% of total costs.30 (More)
- Estimates of the "non-net" costs (e.g., distribution costs) per net. These are based on estimates of costs that AMF and other funders incurred in previous campaigns. Across countries, these account for 44% of total costs on average.31 (More)
- A rough estimate of the value of in-kind government contributions (e.g., staff time) to the campaigns that AMF supports. These account for 5% of total costs on average.32 (More)
We use the cost per net excluding in-kind government contributions (e.g., $4.25 in Uganda) when estimating the number of nets distributed per $1 million spent by AMF.33 This is because we account for these in-kind contributions separately in our adjustment for other actors’ spending. Because we think AMF's spending causes these government costs to be incurred, we adjust the impact of the program downward to account for benefits that are lost as a result of these funds not being spent elsewhere (more below). We also present AMF as covering all costs other than the government’s contributions in our summary of the proportion of costs covered by different actors, even though we think the Global Fund actually covers some costs. This is because we do not have permission to publish the proportion of costs covered by the Global Fund and because these proportions do not make a difference to our bottom line (details in footnote).34
Cost to purchase each net
We estimate the cost per net distributed in an AMF-supported campaign. This varies by country and net type and is based on:
- The average cost AMF told us it expects to pay to purchase each type of net. We assess this at the point of investigating a given grant (e.g., our most recent grant in Uganda was in 2021). We do not have permission from AMF to publish these estimates.
- Our best guess about the proportion of different types of net that AMF will purchase for future campaigns in each location. This is based on discussions with AMF. In Uganda, at the time we made our most recent grant, we thought that AMF planned to purchase 100% PBO nets for its next campaign. This affects our cost estimates because PBO nets are more expensive than pyrethroid-only LLINs.
-
An estimate of the proportion of nets that will be purchased but not delivered (e.g., because they are lost, stolen, damaged, or otherwise not accounted for) based on data from previous distributions. This estimate varies by country, from 2% in Uganda to 10% in Guinea.35 We use this to adjust our estimate of the cost per net purchased to estimate the purchase price of each net that will be distributed. We’re unsure about this data, which we haven’t investigated in detail (more below).
Distribution and other "non-net" costs
Next, we estimate all the other costs associated with net campaigns other than the purchase price. We refer to these collectively as "non-net costs." Unlike our estimates of the costs to purchase nets (which are "forward-looking"), we estimate these costs based on spending on previous campaigns, as we think these will be a better guide to future costs than projections.
Overall, we estimate that the non-net costs per net are approximately $1.50 to $3, varying by location. These costs include:
- The costs of shipping and delivering nets from the factory to people’s homes.
- The costs of conducting surveys after the distributions to monitor how the nets are used.36
- AMF’s organizational costs (e.g., staff salaries) per net distributed. We estimate this based on data on AMF’s historical organizational costs in a given period, divided by the number of nets it distributed in that period.
Unlike the purchase costs of each net, these costs are split between different organizations. In most cases, the Global Fund or another partner pays for most of the distribution costs and AMF pays for the monitoring surveys. To estimate the Global Fund’s distribution costs, we use country-specific information on costs incurred by the Global Fund for some previous campaigns. Because we do not have permission from the Global Fund to publish this information (more below), we do not break down our estimate of non-net costs by component.
In-kind government contributions
The campaigns that AMF supports are ultimately managed by national governments’ ministries of health. We would expect AMF’s funding to divert some ministry of health resources (e.g., staff time, office space, etc.) towards campaigns that might otherwise have gone towards other activities.
We estimate that these resources amount to approximately $0.15 to $0.35 per net distributed, varying by location. This estimate is based on an analysis of a single distribution in Malawi in 2012, which found that the value of these resources accounted for $0.13 per ITN.37 We then adjust this figure to account for changes in the proportion of costs attributable to "non-net costs" between different countries (details in footnote).38
Shortcomings and uncertainties
- Uncertainty about distribution data. Our estimates are based on data shared by AMF on the number of nets distributed in each campaign (we use this to estimate the proportion of nets that are purchased but not delivered). However, we have not reviewed the methodology used to collect this data, and we are unsure how reliable it is (details in footnote).39
One method we could use to corroborate this data is to cross reference it with independent survey data (from the Demographic and Health Surveys and Malaria Indicator Surveys) on the proportion of the population in countries with AMF-supported campaigns with access to nets. Our reasoning is that, if AMF-supported campaigns are reaching a high proportion of targeted households, this should show up in surveys conducted afterwards as a high proportion of households having access to a net. As of December 2023, we have begun this work but not yet finalized or published our analysis. We hope to investigate this question in more detail in the future.
- Lack of information on non-net costs from other funders. Our calculations rely on estimates of non-net costs incurred by other funders, but we have very limited information on these costs. In particular, we use country-specific information on costs incurred by the Global Fund for some previous campaigns, but the information we have only covers a small number of previous campaigns (including some but not all the countries in our analysis).40
We are particularly uncertain about our estimates of non-net costs in DRC, both because we do not have any information from previous campaigns in DRC and because our understanding is that DRC is an unusually expensive location to operate in.
- Another concern about our estimates of the Global Fund’s non-net costs is that we do not have permission from the Global Fund to publish them. We see this as a concern both because we rely on comprehensive data to produce accurate costing analysis, and because GiveWell aims to be transparent about the data underlying our analysis wherever possible.
-
Lack of cross checks from costing studies. We have not systematically cross referenced our estimates against independent data sources (e.g., costing studies, published lists of net purchase prices). In 2023, we conducted a rough internal analysis, indicating our estimates were in roughly the same range as other published data. However, we have not investigated this in detail or published our analysis. We may do more work on this in the future.
3.3 What proportion of nets are used?
We estimate that 63% of nets distributed in GiveWell-funded campaigns are used.41 This is based on net usage in studies underlying the meta-analysis we use to estimate the impact of ITNs on malaria. We estimate that usage was approximately 70% in these studies (more). We then adjust this figure downwards by 10% because we expect that usage in contemporary distributions is lower than was observed in these studies (more). A summary of our calculations is below:
| What we are estimating | Value |
|---|---|
| Net usage in study contexts | 70% |
| Net usage in contemporary distributions, relative to study contexts | 90% |
| Total (proportion of nets used in contemporary distributions) | 63% |
Net usage in study contexts
Our analysis of how nets reduce child mortality is based on a published meta-analysis of 23 studies of ITN distributions (Pryce et al. 2018). The meta-analysis is discussed in detail below. The study’s main finding was that ITNs significantly reduce (a) malaria cases and (b) child mortality from all causes, compared both to no nets and to untreated nets.42
We estimate that net usage in the studies underlying the meta-analysis was around 70%.
- This is based on an analysis of the five studies in the meta-analysis that measured the impact of ITN distributions (compared to no nets) on the incidence of malaria cases.43
- Of these five, we use estimates from three studies (accounting for around 60% of the statistical weight in the meta-analysis for this outcome)44 that provided data on net usage.
- Our best guess is that net usage in these studies was 72% on average.45 We then round this figure to 70% for simplicity and to reflect our uncertainty. See this spreadsheet for details of our calculations.
Our main uncertainty about this estimate is that the figures reported in these studies refer to the proportion of people sleeping under nets the previous night,46 whereas our cost-effectiveness analysis models the proportion of nets that are used. We are uncertain about how comparable these two measures are and can envisage scenarios where there are significant discrepancies between the two.47
Net usage in contemporary distributions
We roughly guess that usage is 10% lower in contemporary GiveWell-supported net distributions than in the studies underlying the Pryce et al. meta-analysis. This implies that net usage in contemporary distributions is around 63%.48
The -10% adjustment is not based on a specific calculation. Instead, we think of this as a reasonable best guess from cross-referencing several sources:
- Intuitively, we would expect usage to be lower in contemporary large-scale ITN distributions than in the context of small-scale studies. Some of these studies involved visits to households after the distribution to encourage net usage and upkeep (discussed in more detail in our summary of Pryce et al.). We would expect these activities to push usage rates upwards relative to contemporary distributions.
- A previous version of the Pryce et al. review, Lengeler 2004a, notes one example where net usage fell as a controlled study of an ITN distribution was scaled up into a national program.49 We interpret this as supporting evidence that larger-scale distributions are likely to see lower usage than controlled small-scale studies, on average.
- AMF conducts surveys after its campaigns to estimate the proportion of nets that are used over time (discussed in more detail in our review of AMF). These surveys have generally found usage rates in the 60 to 80% range, varying by length of time since the initial distribution and the specific definition of usage.50
- In a previous version of this report, we analyzed data from national surveys collected in WHO’s World Malaria Reports to understand more about net usage in sub-Saharan Africa. Our analysis of usage, roughly correcting for possible over-reporting, suggested that net usage was in the 57% to 73% range for most countries in the 2010 World Malaria Report and would have an interquartile range of 68% to 84% for countries in the 2012 World Malaria Report.51 We see this data as providing evidence of usage in roughly the same range as the studies in Pryce et al. Note that we have not revisited this data since 2014.
Our main uncertainties about our estimates are:
- We use a simplifying assumption that usage rates are the same across countries. We would guess that this assumption is unlikely to be correct, and we know of evidence from one paper that finds that usage rates vary across countries with different climate patterns and by season.52 We have not investigated the question of how usage varies by country in depth.53
- Net usage is a challenging outcome to measure accurately. Asking people to self-report whether they slept under a net the previous night is likely to lead to inflated estimates of usage because of social desirability bias (survey respondents being more likely to overreport “good” behaviors).54 We believe that measuring usage with a high degree of accuracy would require unannounced visits to homes at night, which we have not seen outside the context of some studies in the Pryce et al. meta-analysis (because of the high disturbance caused).
3.4 How many people sleep under each net?
We estimate that approximately two people sleep under each net used (varying somewhat by country).55 A summary of our calculations is below, using one country (Uganda) as an example:
| What we are estimating | Value |
|---|---|
| Average number of people sleeping under an in-use net, from AMF data | 1.88 |
| Adjustment for social desirability bias | -6% |
| Total (Average number of people per net) | ~1.8 |
Our analysis is based on data from surveys conducted by Against Malaria Foundation which aim to track how the nets it distributes are used over time.56 Survey data collectors count the number of nets found hanging in surveyed households and ask households to self-report how many people slept under each hanging net the previous night. From these two figures, we can infer the average number of people sleeping under each hanging net.57
Our analysis includes a downward adjustment of -6% to the estimated number of people sleeping under each net to account for social desirability bias (details in footnote).58 See this spreadsheet for our full calculations.
Our main uncertainties about this analysis are:
-
We have some reservations in general about AMF’s monitoring data, discussed here in our separate page on AMF. We could cross check these assumptions against independent sources of data like the Demographic and Health Surveys (DHS) and Malaria Indicators Survey (MIS). We haven’t yet conducted this analysis, but may do so in the future.
- Our estimate of the impact of social desirability bias is based on our “priors” (our subjective best guesses about what a plausible adjustment for social desirability bias would be). We do not have any data to validate these assumptions.
3.5 Usage by age
We assume that children under five sleep under nets in equal proportion to their share of the population in each country (e.g., if children under five are 20% of the population, 20% of the people sleeping under nets are children under five). In the countries included in our cost-effectiveness analysis, the percentage of children under five ranges from 14% to 17% of the population.59 This breakdown is important because young children are at highest risk from malaria, and our analysis is sensitive to the level of protection they receive.60
This method is rough and further investigation could lead us to update our estimates of children’s net usage either up or down. As with overall net usage (more above) and the number of people using each net, one approach we could use to update our analysis is checking the proportion of people using nets in different age groups in independent surveys such as the Demographic and Health Surveys or Malaria Indicator Surveys. We have conducted an initial analysis of this data, but have not yet completed or published this work.
3.6 How long does each net provide protection?
Overview
We estimate that one AMF-purchased net confers 1.2 to 2 years of effective protection over the course of each three-year distribution cycle.61 We define "effective protection" as protection at the same level provided by the nets in the studies we rely on to measure the impact of nets on malaria (discussed below).
WHO recommends that net distributions should take place at three-year intervals in most places,62 whereas our estimate of the impact of nets on malaria is based on studies with an average follow-up period of around one year (we refer to these as “study contexts,” more below). We think that nets decay over time, and so we would be overstating the benefits of net distribution by extrapolating that impact over the full three years. To do this, we need to account for two things:
- The level of decay in study contexts nets (due to, e.g., insecticide decay, wear and tear).
- The level of decay in nets distributed today, relative to study contexts.
Our estimate is based on studies that tracked, in real-life conditions, the retention and physical integrity of two common net brands. We then compare these results with data and best guesses about net durability in the meta-analysis that measured nets' impact on mortality.63
A summary of our calculations for Uganda is below:
| What we are estimating | Value (rounded) |
|---|---|
| Years of protection provided by one type of contemporary LLIN (Vestergaard PermaNet 2.0) per year, relative to study contexts (more) |
|
| Subtotal: Total years of protection provided by each Vestergaard PermaNet 2.0 purchased today, relative to study contexts | 2.27 |
| Adjustment for durability of "next-generation" nets (more) | 0% |
| Adjustment for % lower durability for "generic" LLINs (more) | -15% |
| % of nets purchased by AMF, 2018 - 2020 | |
|
|
| Adjustment for pre-existing nets (more) | -7% |
| Total (total years of effective protection provided by each net, relative to study contexts) | 2.0 |
We also estimate that:
- Net durability in DRC is 17% lower than in other locations (more).
- The effective level of protection each net provides is 29% to 37% lower in South Sudan, DRC, and some states in Nigeria. For DRC, this represents a separate, negative adjustment in addition to the 17% net durability adjustment. This reflects our guess that the impact of extra funding in these locations is to reduce the amount of time between distributions (e.g., a given region moving from a four-year interval to a three-year interval), rather than increasing the number of people reached in a particular campaign. (More)
The calculations for our durability analysis are available here.64
A note on net definitions
Throughout this section, we use the following terms:
- Contemporary nets / ITNs: ITNs that AMF has purchased for recent campaigns or may purchase in the future.
- Conventional nets / ITNs: The more rudimentary form of ITN used in the studies we rely on to estimate the impact of nets on mortality. These required retreatment with insecticide to top up their insecticide levels (more below).
Contemporary nets can be further subdivided as follows:
- ITNs vs LLINs: To be categorized as “long-lasting” by WHO, ITNs must remain effective after 20 washes in lab conditions and for three years in real-world conditions.65 Our understanding is that the only nets categorized as LLINs to date are pyrethroid-only LLINs. PBO, chlorfenapyr and pyriproxyfen nets are not yet categorized as LLINs because they have not met WHO durability standards (more above).
- WHO qualification status: ITNs can be either “generic” (e.g., the Yorkool LN) or “reference class” (e.g., the PermaNet 2.0) depending on whether or not they have passed Phase III WHO testing (more below).
We expect that each factor has an influence on a net’s durability. We discuss how we account for these in the sections below.
Our approach
Overview
We expect that ITNs do not provide protection for their full recommended lifecycle (three years).66 This may be for a number of reasons, including being given away, lost, stolen or appropriated for other uses, holes or tears developing in the fabric, and the insecticide in the net fibers losing efficacy over time.
Our analysis of how long each net provides protection considers three main outcomes67 , in line with WHO and the U.S. President’s Malaria Initiative (PMI) guidelines for ITN field durability monitoring:68
- Attrition: The proportion of distributed nets that are no longer present or being used as intended (e.g., because they’ve been thrown away due to damage or used for something else).69
- Physical integrity: A measure of the physical integrity of the net's textile. Each net is classified as “Good,” “Serviceable,” or “Too torn” based on the proportion of its surface covered in holes.70
- Residual insecticide content: The concentration of the insecticide chemical in the net.71
Data on LLIN durability
Our starting point is an analysis of durability data for one specific type of pyrethroid-only LLIN, the Vestergaard PermaNet 2.0.72 We conducted a literature search and compiled a dataset of studies containing field monitoring data on the PermaNet 2.0. In total, we identified 11 monitoring studies (covering distributions between 2005 and 2017 in 10 countries).73
We aggregate the data from these studies by taking a simple average of the proportion of surviving nets and the proportion of surviving nets classified as "too torn" across all studies at each follow-up interval after distribution.74 The aggregated data is available in this sheet.75
We extrapolate durability data from the PermaNet 2.0 to other types of net using a number of assumptions, discussed below. The focus on the PermaNet 2.0 is a limitation of our analysis, because we increasingly expect that GiveWell funding will be used to buy next-generation nets (particularly pyrethroid-PBO nets and pyrethroid-chlorfenapyr nets),76 and we have less information on their durability. This means our current analysis is likely to become less accurate over time (more below).
How durable are LLINs, compared to the nets used in the original net studies?
Next, we compare the PermaNet 2.0’s durability to the nets in the meta-analysis that measured nets' impact on child mortality (discussed below). While the durability information provided in these original studies is limited, we think that the type of net used and the conditions in which they were studied are likely to have resulted in higher durability compared to nets distributed today.
One weakness in our approach is that this comparison is based on data from five studies in the meta-analysis that measured all-cause mortality. This is different from the main input we use to model the impact of ITNs on mortality, which relies on different studies in the meta-analysis that measured malaria cases (details in footnote).77
We make the following assumptions for each durability metric:
- Attrition. We assume that there was no net attrition in the studies estimating the impact of ITNs on child mortality.78
As a result, we assume all attrition measured in monitoring studies of the PermaNet 2.0 counts as lost protection, relative to the studies in the meta-analysis.79
- This assumption is based largely on data from Phillips-Howard et al. 2003, which reported low attrition rates.80
- Researchers also distributed additional nets during the course of the Phillips-Howard et al. 2003 study (meaning there may have been more nets available for use at the end than at the beginning).81
- Physical integrity. We assume that the nets used in the mortality meta-analysis suffered one-third less damage compared to PermaNet 2.0 nets at each relevant monitoring point up to 24 months post-distribution (when the studies ended).82 This is a rough best guess, because none of the studies estimating mortality reported data on nets’ physical integrity. Our reasoning is:
-
Insecticide decay. We assume that the PermaNet 2.0 sees no more or less insecticide decay over a 36-month distribution cycle than the ITNs in Pryce et al. saw over the 24 month period that they were studied.86 The pyrethroid insecticide in contemporary nets decays more slowly than in conventional ITNs, but regular retreatment of conventional ITNs tops up insecticide levels. If we assume the ITNs assessed in Pryce were retreated with insecticide every six months (as per the trial protocols), our analysis suggests that the average level of insecticide in each type of net would likely be similar over time (details in footnote).87
Taking all these factors into account, we estimate that a PermaNet 2.0 provides 2.27 years of effective protection over a three-year distribution cycle.88 See this section of our analysis for our calculations.
Adjustment to account for other net types
Our analysis above is based on data for the PermaNet 2.0 only. In practice, we expect that AMF may purchase other types of net. These include "generic" LLINs (which have received product prequalification from WHO based on passing Phase I and sometimes Phase II tests, but haven't undergone Phase III field testing)89 and next-generation nets (e.g., those containing additives like PBO (piperonyl butoxide) or additional insecticides like chlorfenapyr).90 More on these different net types above.
- We assume that generic LLINs have 15% lower durability than the PermaNet 2.0 (a “reference class” net. This adjustment is based on an analysis of four durability studies of the Yorkool LN, a generic LLIN which did not have to undergo field durability testing for WHO approval.91
- We assume that PBO and other types of next-generation nets have equivalent durability as the PermaNet 2.0.92 This is a rough guess because we have not yet done a detailed review of next-generation net durability, and it is possible that the additional chemicals in next-generation nets decay at different rates to the pyrethroid insecticide used in contemporary ITNs (more below).
- We calculate a weighted average of durability based on the proportion of different net types purchased by AMF between 2018 and 2020.93
This method produces an adjusted figure of 2.11 years of effective protection provided by the average AMF-purchased net. See this section of our analysis for our calculations.
Adjustment for net durability in DRC
We assume that net durability in DRC is 17% lower than in other locations. This adjustment is based on data we have seen from Against Malaria Foundation’s post-distribution monitoring surveys, which track net usage and condition over time. We also incorporate data from a durability study conducted by PMI in DRC, which finds worse durability in DRC compared to our analysis of durability in other locations.94
This adjustment reduces our estimate of the length of effective protection provided by each net from 2.11 years in other locations to 1.75 years in DRC. See this spreadsheet for our calculations.
Adjustment for moving distributions closer together
Our cost-effectiveness analysis models the impact of net distributions taking place at three-year intervals (as recommended by WHO). This assumes that, without funding from AMF, distributions would still happen on three-year intervals but fewer nets would be distributed.
In fact, our understanding is that in DRC, some states in Nigeria, and South Sudan, at the time we made our most recent grants, additional funding was more likely to reduce the amount of time between distributions (e.g., a given region moving from a four-year interval to a three-year interval), rather than increase the number of nets distributed in a particular campaign (details in footnote).95 In these circumstances:
- Recipients receive some additional benefits, since they receive a new net (that provides high protection) in place of an old net (that provides little protection) earlier than they otherwise would.
- But there are also additional costs that come from having to buy more nets (since to replace nets more frequently, you need more nets).
We think that the cost per additional year of protection from moving distributions closer together is higher than the cost per additional year of protection from protecting people who would otherwise not receive a net at all.
To account for this, we use an adjustment to reduce the overall number of years of coverage96 provided by nets in DRC (-29%), some states in Nigeria (-35%), and South Sudan (-37%).97 A summary of our calculations for one country, DRC, is below.
| What we are estimating | Value |
|---|---|
| Cost per ITN distributed in DRC (discussed above) | $5.85 |
| Campaign intervals | |
| Standard interval between net campaigns, as recommended by WHO | 36 months |
| Estimated interval between net campaigns in DRC without GiveWell funding | 42 months |
| Estimated interval between net campaigns in DRC with GiveWell funding | 33 months |
| Years of effective coverage per year for different campaign intervals | |
| Average number of years of effective coverage provided per year over the course of a 36-month distribution period | 0.58 |
| Average number of years of effective coverage provided per year over the course of a 42-month distribution period | 0.52 |
| Average number of years of effective coverage provided per year over the course of a 33-month distribution period | 0.62 |
| Cost per year of effective coverage at different campaign intervals | |
| Cost per year of effective coverage in a standard 36-month distribution | $3.34 |
| Cost per year of effective coverage from reducing the interval between campaigns from 42 to 33 months | $4.73 |
| Total (reduced cost-effectiveness from reducing the interval between campaigns compared to expanding campaign coverage) | -29% |
Overall, we’re uncertain about this adjustment. Our biggest uncertainties are:
- The calculations we use for this adjustment are complex and unintuitive. We think that this raises the likelihood that we could be making a mistake.
- Our analysis estimates how much AMF’s funding will reduce the interval between campaigns in each location (e.g., 42 to 33 months in DRC). This involves making guesses about what would happen in the absence of AMF’s funding, which is necessarily speculative.
- Our analysis is sensitive to the rate at which nets deteriorate towards the end of their lifespan (e.g., from year 3 to year 4). The durability studies we rely on do not provide any data after year 3, so our assumptions about decay at this stage are based on rough guesses.98
-
We have received feedback from AMF that this adjustment mischaracterizes the impact of its funding (details in footnote).99 This implies we could be underestimating cost-effectiveness in these locations.
We calculate this adjustment using the following method:
- First, we estimate the average number of years of effective coverage provided by nets at different possible intervals (up to six years).
- Years 1-3: We use the figures discussed above.100
- Years 4-6: We have not reviewed data from field monitoring on net durability over this period, so we extrapolate based on the data we have reviewed in years 1-3 and some rough guesses (details in footnote).101
- We apply adjustments of -7% to account for reduced coverage from generic LLINs (details in footnote)102 and for lower durability in DRC (details in footnote).103
- Overall, we estimate that the number of years of effective coverage per net falls from 0.92 in year one to 0.01 in year six after a distribution in most countries, and 0.81 to 0.00 in DRC in the same period.104
- We also estimate the level of effective coverage remaining at each month post-distribution by extrapolating from our estimates above and assuming linear decay over each successive month (details in footnote).105 For example, this method suggests that nets distributed at 36-month intervals in DRC provide an average of 0.58 years of effective coverage per year over the course of their 3-year lifespan.106
- We roughly estimate what the impact of AMF’s funding will be on the interval between campaigns in each location.
- For example, we guess that the impact of AMF’s funding in DRC will be to shorten the average interval between campaigns from 42 months to 33 months in the provinces it supports.107
- These estimates are based on our understanding of the funding landscape for ITN campaigns in each country, AMF’s expectations about the impact of its funding, and the historical timing of the country's past campaigns (details in footnote).108
- We use the estimates above to calculate the cost per year of effective coverage provided for campaigns at 36-month intervals (which our main cost-effectiveness analysis is modeling) and compare it to the cost per year of effective coverage from shortening the interval between campaigns.109 This calculation implies that the cost per year of effective coverage from shortening the interval between campaigns is 29% lower in DRC, 35% lower in some states in Nigeria, and 37% lower in South Sudan.110
- Intuitively, the reason this is a significant downward adjustment is that we think nets still provide some protection on average after three years. This means that shortening the interval between campaigns (and causing people to receive a new net earlier than they would have otherwise) is not as cost-effective as increasing the proportion of people who receive a net in a given campaign.
See this section of our cost-effectiveness analysis for our calculations.
Adjustment for pre-existing nets
Some households who receive nets in mass campaigns might already have non-worn-out nets available from previous campaigns. In these cases, we would expect some of these households to throw away their old nets. We think that this effectively results in some coverage that could have been provided by the old nets being lost, and therefore reduces our estimate of the level of coverage net distributions provide.
To account for this, we estimate a downward adjustment of 3% to 7% (varying by location).111 Our approach is:
- We take the number of years of effective coverage that we think residual nets have left at the point that a new campaign is most likely to happen. For most countries, this is 0.29 years (at the end of a three-year distribution cycle).112 In Nigeria, South Sudan, and DRC, we use different estimates based on our best guesses about the likely impact of AMF’s funding reducing the interval between campaigns (details in footnote).113
- We assume that households discard 50% of residual nets at the point of a new distribution.114 We have not seen any empirical data to support this estimate, so this is a very rough guess.
- We multiply the number of years of coverage at the point of a new distribution (0.29 in most countries) by 50% to estimate the overall loss in effective coverage, and divide it by our overall estimate of the number of years of effective coverage (2.11 in all countries except DRC) to estimate our final adjustment (3% to 7%).
See this section of our cost-effectiveness analysis for our calculations.
Shortcomings and uncertainties
Net durability is a research area with a fairly extensive evidence base, and our analysis is based on a detailed review of that evidence. Nonetheless, our durability estimate relies on a number of best guesses and uncertain assumptions. We’ve also not significantly updated our analysis since 2020, meaning it risks becoming increasingly inaccurate as other types of next-generation net become more widespread. Our key uncertainties are:
-
We have not yet conducted a separate durability analysis for next-generation nets. Instead, we assume that these nets have equivalent durability to the PermaNet 2.0, which we have reviewed in detail.
- At the time we first conducted our analysis, we thought this was a reasonable simplifying assumption. Our understanding was that these nets are very similar to pyrethroid-only LLINs, with the same physical properties (with the exception of the added chemical component).
- But it's possible that the extra chemical components in these nets decay at a different rate than pyrethroids. In 2023, we conducted an internal unpublished analysis on this question. We found some evidence that the PBO additive in PBO nets decays at faster rates than the pyrethroid insecticide, implying our model is overestimating durability in locations where PBOs are distributed. But we have not yet prioritized investigating this question in detail. We’ve also not deeply investigated the durability of chlorfenapyr or pyriproxyfen nets.
-
Our estimate of ITN durability is based on weighting different net types’ durability by the volume of those nets purchased by AMF between 2018 and 2020.115 We have not updated this analysis since 2020 and the proportion of each type of net may have significantly shifted since then. In particular, we would expect contemporary campaigns to involve a higher proportion of PBO and other next-generation nets. Our weighted average approach is also not fine-grained enough to take into account differences in the types of net purchased for specific campaigns.
- Our analysis of insecticide content is based on just one study, which may not be generalizable.116 More broadly, the relationship between insecticide content and insecticidal efficacy is unclear and there is evidence that efficacy can be high even at low insecticide concentrations, meaning the results of our comparison are challenging to interpret.117
- There is relatively little information on net durability in the studies in the Pryce et al. meta-analysis, meaning that we base our comparison between net durability in study contexts and contemporary distributions on some rough guesses. For example, we use a guess that the nets in the RCTs suffered a third less physical damage than nets in contemporary distributions because some of the RCTs included training and materials on net use and repair. We use a guess here because none of the Pryce et al. studies measuring reductions in child mortality report data on nets’ physical integrity.
-
Our analysis of durability in Pryce et al. is based on the studies that measured all-cause child mortality, not the studies measuring malaria incidence that we primarily rely on in our cost-effectiveness model.118 We have not yet updated our durability model to account for any differences between the studies measuring all-cause child mortality and the studies measuring malaria incidence.119
3.7 How many people would access nets from other sources?
The question of how many people access nets from other sources is important because it relates to counterfactual impact. We’re interested in the impact of us funding a mass distribution campaign relative to us not funding a mass distribution campaign. The difference between these outcomes is affected by how likely people are to access nets from other sources. For example, consider the following scenarios:
- We fund a mass distribution campaign; some people that receive nets already have nets.
- We fund a mass distribution campaign; some people that receive nets get more nets in future (e.g., from a health clinic visit), so prematurely throw away the nets we distribute.
- We don’t fund a mass distribution campaign; people get nets anyway because another funder (e.g., the Global Fund) steps in and funds a mass distribution campaign.
- We don’t fund a mass distribution campaign and neither does another funder. However, people get nets anyway because they buy them from shops, or access them through routine distribution channels (e.g., via health clinic visits).
Each of these stories shrinks the impact of funding a mass distribution campaign relative to not funding it (i.e., our counterfactual impact). Concern 1 is captured by our adjustment for pre-existing nets. Concern 2 is captured by our durability calculations,120 and concern 3 is captured by our adjustment for other actors’ spending.
We currently have no adjustments in the model to account for concern 4. Effectively, this amounts to assuming that people today are no more or less likely to obtain nets from other sources than they were during original studies testing the impact of ITNs on malaria (more below), which were predominantly conducted in the 1980s and 1990s. In these trials, around 5% to 10% of people had access to nets in the control group.121 By using these control groups as a stand-in for the counterfactual today, we effectively assume that 5% to 10% of people would get nets in the absence of any mass distribution campaign.
We haven’t vetted this assumption thoroughly and plan to do so in future. We think there are a few reasons to believe this assumption may not be a bad approximation:
- Mass distribution campaigns are still the dominant channel through which people in malaria-endemic countries acquire nets. The latest Demographic and Health Survey (DHS) data suggests that 91% of households that own nets got them from mass campaigns in Uganda, 83% in Guinea, 76% in Nigeria and 68% in Togo.122 While there are reasons to be cautious in interpreting this data (more below), the fact that mass campaigns account for the lionshare of coverage at least suggests that coverage would be significantly lower in their absence.
- There’s evidence that uptake of nets falls dramatically when people have to pay. For example, we have seen a one paper123 showing that the uptake of insecticide-treated nets fell by 60 percentage points when the price increased from zero to $0.60 in Kenya.124 We think this allays the concern that people would just buy nets if they didn’t receive them from a mass distribution campaign, though leaves open the question of whether they would seek out free bed nets from continuous touchpoints (e.g., health clinics).
- The people that most benefit from mass distribution campaigns may be the least likely to acquire nets from other sources. People in poor/remote areas (where we’d expect mortality effects to be concentrated) may be the least likely to get nets from other sources, due to lower disposable income and/or them being less likely to visit health facilities.
On the other hand, there are also reasons to think this might not be a good assumption:
- It seems intuitive that nets are more accessible through other channels today. Our guess is that access to nets through continuous distribution channels has increased over time, as malaria funding has grown since the 1980s and 1990s. This implies that if people without access to mass distribution campaigns wanted to get nets, they would probably have more options today.
- DHS data can’t capture behavioral responses to a lack of mass distribution campaigns. We think we should be cautious about interpreting aggregate DHS data on net sources. For example, if mass distribution campaigns already cover the vast majority of people in Uganda, this data doesn’t tell us much about how people/health systems would respond to a lack of campaigns. A better way to investigate this would be to look at net access in regions that have not had a mass distribution campaign for many years, which would better probe this counterfactual. We haven’t done this yet, but plan to do so in future.
Our best-guess is that we are probably underestimating concern 4. Rather than 5 to 10%, we think it’s more likely that 20%125 of people would get nets in the absence of a mass campaign, either through purchasing one themselves or receiving one via a continuous touchpoint in the health system. This would result in a 10% reduction in cost-effectiveness.126 We plan to explore this more by examining: what net access is like in places that have not recently received mass campaigns, the extent to which this differs between countries, and whether it makes sense for GiveWell to support programs which seek to strengthen continuous distribution channels.127
4. What impact do net campaigns have?
4.1 Summary
Our cost-effectiveness analysis models three main benefits from ITN campaigns:
- Reduced mortality for children under age five (more).
- Reduced mortality for older children and adults (more).
- Increased long-term income, from averting malaria in a sensitive developmental window of childhood (more).
A summary of the contributions of each type of benefit to our estimate of the modeled value of the program is below, using Uganda as an example.128
| What we are estimating | % modeled benefits |
|---|---|
| Reduced mortality for young children | 59% |
| Reduced mortality for older children and adults | 9% |
| Long-term income increases | 32% |
We also include a number of supplemental adjustments to account for additional benefits and offsetting impacts. Rather than explicitly modeling these, we have applied percentage adjustments based on our best guesses.
- We divide these into intervention-level factors (e.g., costs averted from treatment of illness), which increase our cost-effectiveness estimate by 38% to 48% overall (38% in Uganda) (more), and grantee-level factors (relating to the implementation of the program), which reduce our estimate by 4% (more).
- We also include an adjustment to incorporate the impact of AMF’s funding on other actors’ spending. This reduces our cost-effectiveness estimate by approximately 15% to 40% depending on the location (32% in Uganda) (more).
- Overall, we estimate that it costs approximately $3,000 to $8,000 (varying by location) to avert a death through ITN campaigns. This equates to being approximately 9 to 23x as effective as spending on unconditional cash transfers.129
Some of the major uncertainties in these estimates are:
- Our estimates of the effects of malaria on later-life income are based on very uncertain historical evidence (more).
- We think that malaria increases the risk of mortality from other causes and estimate that this causes 0.75 indirect deaths from other causes for each direct malaria death. This is a highly uncertain best guess from triangulating several different sources (more).
- Our analysis relies on estimates of malaria mortality from the Institute for Health Metrics and Evaluation's (IHME) Global Burden of Disease (GBD) Project. These estimates are based on modeling assumptions that we have not fully investigated (more).
4.2 Reduced mortality for children under five
ITNs reduce child mortality by averting malaria cases. We estimate that each $1 million spent by AMF averts ~100 to ~450 deaths of children under age five (varying by location).130 A summary of our calculations is below, using one country (Uganda) as an example:
| What we are estimating | Value (rounded) |
|---|---|
| Number of children under five protected for one year (discussed above) | ~89,000 |
| Reduction in malaria deaths among children using nets (more) | 51% |
| Malaria-attributable mortality rate for children under five without access to nets (more) | 0.64% |
| Total (under-five deaths averted) | 294 |
The impact of ITNs on malaria mortality
Summary
Overall, we estimate that sleeping under a net reduces a child’s mortality risk by 39% to 56% (varying by country) per year of effective protection.131 This is based on an estimate from a meta-analysis, Pryce et al. 2018, that ITN distributions reduce the rate of malaria cases by 45% during a roughly one-year average period after distribution (more).132 We then apply the following adjustments:
- An adjustment to convert the estimate of the impact of net distributions (45%) into an estimate of the impact of sleeping under nets (64%), based on the estimated proportion of children who used nets in the meta-analysis (70%). (More)
- An adjustment for reduced effectiveness because of insecticide resistance (-4 to -33%, depending on the location).133 (More)
- Downward adjustments for internal validity (study quality) and external validity (generalizability) of -5% each. (More)
We also convert the impact on malaria cases into an estimate of the impact on malaria deaths. To do this we assume a 1:1 relationship between reduced malaria cases and reduced malaria deaths (more).
A summary of our calculations is below, using one country (Uganda) as an example:
| What we are estimating | Value |
|---|---|
| Reduction in malaria cases from being targeted for insecticide-treated net campaigns (more) | 45% |
| Proportion of children sleeping under nets in study contexts (more) | 70% |
| Subtotal: Reduction in malaria cases among children using nets | 64% |
| Reduced effectiveness because of insecticide resistance (more) | -11% |
| Adjustment for study quality and generalizability (more) | 95%, 95% |
| Ratio of malaria case reductions to reductions in malaria deaths (more) | 100% |
| Total (reduction in malaria mortality from using ITNs) | 51% |
How do net distributions affect malaria cases?
We estimate that net distributions reduce malaria cases by 45%.134 This estimate is based on results from a meta-analysis by Cochrane,135 Pryce et al. 2018, which summarizes 23 randomized controlled trials of ITN distributions.136
The studies in Pryce et al. 2018 were conducted between 1985 and 2002 (with most taking place in the 1990s),137 and the programs they evaluate differ from contemporary distributions in a number of ways. Key features of the programs and the study contexts that inform our analysis are:
- What happened in the control group. Of the 23 studies in Pryce, 12 studies evaluated ITNs compared to a control group that did not receive any nets, and 11 studies evaluated ITNs compared to untreated nets.138 We focus on the 12 studies evaluating ITNs vs no nets in our analysis. This is because we expect that in the absence of ITN distributions, people are more likely to not use nets at all rather than use untreated nets.
- The intervention being delivered. The specific approaches used in the 12 studies evaluating ITNs vs no nets varied. One study evaluated the impact of insecticide-treated curtains (for hanging over household doors or windows) rather than bednets,139 and another study compared bednets vs curtains vs a control group who received neither.140 The remaining 10 studies evaluated bednets.141 Some studies also included pre- and post-distribution activities to encourage households to use and maintain their nets (e.g., visits to check nets were being used properly).142 These activities are more intensive than anything we have seen in contemporary distributions, and our best guess is that they promoted better net upkeep and higher usage.143
- The type of nets used. The studies in Pryce et al. 2018 were conducted before ITNs were as widespread as they are today. The studies evaluated more rudimentary types of net, which are treated with insecticide using a less durable method and require regular retreatment (“conventionally-treated nets”).144 Most of the programs evaluating ITNs vs no nets in Pryce retreated nets every six months, although in a few studies the interval was longer or shorter than this (or the studies are unclear).145
- The type of randomization. 15 of the 23 studies randomized at the village or community level, 6 at the household level, and 2 at the individual level.146 The campaigns GiveWell funds today all deliver nets to whole communities.
- Study duration. Most of the 12 studies evaluating ITNs vs no nets lasted either one or two years (although some were shorter). No study measured outcomes beyond two years.147 The five studies measuring the impacts of ITNs vs no nets on malaria cases (that we primarily rely on in our analysis, more below) lasted approximately one year on average,148 and the separate five studies measuring the impacts of ITNs vs no nets on all-cause mortality (that we use in our analysis of net durability) lasted approximately two years on average.149 This is an important distinction from contemporary distributions, which are recommended at three-year intervals.150 We attempt to adjust for this difference in our analysis of net durability, discussed above.
- Net usage. Some studies report how many people slept under distributed nets, either by measuring this (via household visits to observe people sleeping under nets) or asking people to self-report net usage in surveys. Most studies measuring net usage found usage in the 60% to 80% range, while self-reported usage was generally higher.151 We would expect measured usage to be significantly more accurate. As discussed in the section of this report on net usage, our best guess is that usage in the studies we rely on most in our cost-effectiveness analysis152 was around 70% on average.
- Insecticide resistance. Our understanding is that insecticide resistance was less widespread when the studies were conducted than it is in most malaria endemic countries today,153 although some studies in Pryce et al. did find evidence of resistance. Our analysis finds that, out of 18 studies in the meta-analysis,154 mosquitoes were susceptible to insecticide in six studies and resistant (to varying degrees) to insecticide in four studies. In eight studies the level of resistance is unknown.155 Of the five studies that measured malaria incidence rates, which we rely on most in our cost-effectiveness analysis156 (discussed below), our analysis suggests that mosquito populations were resistant in one study (which comprises only a low proportion of the meta-analysis weight), susceptible in two studies, and the level of resistance is unknown in two studies.157
Overall, our assessment is that, while these studies provide strong evidence of the effectiveness of ITN distributions against malaria, the programs involved are not fully comparable to contemporary distributions. We account for these differences throughout our cost-effectiveness analysis with various adjustments. These include:
- Net usage, which we would guess is lower in contemporary distributions than in the meta-analysis studies (more).
- Nets losing their protective effect over time (on average, our analysis suggests that nets in contemporary distributions are less durable than the nets in these studies) (more).
- The growth in insecticide resistance since the trials in Pryce et al. were conducted (more).
- Internal and external study validity adjustments (more).
The main finding of Pryce et al. 2018 is that ITN distributions provide protection against malaria compared to no net distributions.158 The specific outcomes measured included:159
- All-cause child mortality: ITN distributions reduced overall under-five child mortality by an estimated 17% (95% Confidence Interval (“95% CI”) 11% to 23%) compared to no nets (data from five studies).160
- Malaria incidence: ITN distributions reduced the incidence161 of uncomplicated episodes of P. falciparum, the type of malaria responsible for the vast majority of malaria deaths,162 by an estimated 45% (95% CI 36% - 52%, data from five studies) compared to no nets. These results are based on a different set of studies from the estimates on all-cause mortality (with one overlapping), as most studies measured one or the other outcome but not both.163
- Severe malaria cases: ITN distributions reduced the incidence of severe malaria cases by an estimated 44% (95% CI 18% to 62%) compared to no nets (two studies).
- Malaria prevalence: ITN distributions reduced the prevalence164 of P. falciparum malaria by an estimated 17% (95% CI 2% to 29%, six studies) compared to no nets.
- Hemoglobin: ITN distributions increased average hemoglobin levels by an estimated 1.29 increase in percentage packed cell volume (95% CI 0.42 to 2.16) compared to no nets (five studies).
The review authors assessed the quality of studies included as generally high. They evaluated each study for risk of bias. The studies comparing ITNs against no nets were evaluated as low risk in most categories.165 We have not independently assessed each study for risk of bias.
Overall, we interpret Pryce et al. 2018 as providing strong evidence that ITN campaigns reduce both malaria cases and mortality compared to no nets. We use the estimated 45% reduction in uncomplicated episodes of P. falciparum malaria as our starting point for estimating the impact of contemporary distributions on under-five malaria mortality in our cost-effectiveness analysis.166 This approach allows us to adapt our analysis more easily to contexts where the proportion of deaths due to malaria differs substantially from that observed in the Pryce et al. studies.167 We separately account for non-malaria deaths indirectly averted elsewhere in our analysis (more below).
- Approximately one-third of the meta-analysis weight for this outcome comes from studies that measured malaria episodes for people of all ages, not just young children.168 Elsewhere in our cost-effectiveness analysis we estimate that ITNs provide less effective protection for older children and adults than young children.169 This implies that the 45% estimate we use could underestimate the protective impact of ITNs on young children. We have not investigated this in detail or included an adjustment to account for this.
- Converting this estimate into an estimate of the impact of ITNs on mortality requires an additional assumption about how far reductions in case rates translate into reductions in malaria mortality (see below).
The impact of using ITNs on malaria
The finding from Pryce et al. 2018 that ITNs reduce malaria incidence by 45% estimates the reduction in malaria cases among households who were targeted by ITN distributions compared to a control group (an "intention-to-treat" estimate). It does not measure the reduction in malaria cases among households who received and used these ITNs (a "treatment-on-the-treated" estimate).170
To estimate the impact of using nets on malaria cases, we include an additional adjustment for net usage rates in the Pryce et al. meta-analysis. We estimate that around 70% of ITN recipients in the Pryce et al. studies used ITNs (see this section for a discussion of our analysis). We divide the Pryce et al. estimate of reductions in malaria cases (45%) by 70% to estimate the reduction in malaria incidence among children sleeping under nets (64%).171
This could yield inaccurate estimates of the impact of nets if the proportion of children using nets differed significantly between trial contexts and contemporary ITN distributions (discussion in footnote). Our concern about this is mitigated because we believe that usage in contemporary ITN distributions is relatively similar to usage in the studies included in Pryce et al. (discussion in footnote).173
Insecticide resistance
We estimate that insecticide resistance reduces the protection provided by nets by 4% to 33% (varying by location, and based on the mix of nets used).174 A summary of our calculations is below, using one country, Uganda, as an example:175
| What we are estimating | Value |
|---|---|
| Mosquito mortality based on insecticide resistance tests, relative to trials in Cochrane meta-analysis (standard LLINs) | 38% |
| Share of net effectiveness provided by insecticide / physical barrier | 73% / 27% |
| Effectiveness of standard LLINs in Uganda today, relative to Cochrane meta-analysis | 55% |
| Subtotal: Reduction in effectiveness from insecticide resistance (standard LLINs) | 45% |
| Reduction in effectiveness from insecticide resistance, relative to trials in Cochrane meta-analysis (PBO nets) | 4% |
| Proportion of areas in Uganda where PBO nets are more effective than standard LLINs | 82% |
|
Proportion of PBO nets we thought AMF would purchase in Uganda at the time we made our most recent grant
|
100% |
| Total (reduction in effectiveness due to insecticide resistance in Uganda) | 11% |
Since the studies in Pryce et al. were conducted in the 1980s to 2000s,176 mosquitoes in malaria-endemic areas have developed increasing resistance to the most common type of insecticide used in LLINs.177 This is likely to make them less effective. However, in more recent years, new types of next-generation nets containing additives (e.g., PBO and chlorfenapyr) designed to combat insecticide resistance have been developed.178 We would expect these to restore some of the effectiveness that standard LLINs have lost.
Our insecticide resistance calculations are available here. Note that these calculations factor in both the level of insecticide resistance and the type of net we think our grantees were likely to purchase in a particular location at the time we investigated our most recent grant. This means our analysis is likely to evolve over time, since our grantees are likely to purchase different types of net for different distributions, and our analysis is sensitive to the type of net used.
Our analysis is based on the following steps:
- Estimating insecticide resistance for standard LLINs
- The most common test used to measure insecticide resistance is a WHO-standardized diagnostic dose assay. These tests expose wild-caught mosquitoes to insecticide and measure their mortality rates.179 We collate the results of tests conducted between 2013 and 2020 from 11 endemic countries and take the average test result from each country during that period.180 The average mosquito mortality rate in these tests varies from 23% to 95%, depending on the country.181
- We roughly adjust for increasing resistance since the studies were conducted by assuming an additional increase in insecticide resistance of 0.83 percentage points per year (details in footnote).182
- ITNs are likely to provide some protection by acting as a physical barrier to mosquitoes in addition to their insecticidal role.183 We estimate that 27% of the protection provided by nets in the Cochrane review underlying our analysis was attributable to the physical barrier and 73% was attributable to insecticide (details in footnote).184 We apply these percentages to the mosquito mortality results discussed above to estimate a reduction in effectiveness for standard LLINs of 22% to 62% (45% in Uganda), varying by country (calculations in footnote).185 This can be interpreted as reduced effectiveness relative to the studies in the Cochrane meta-analysis we rely on.186
- Estimating resistance for "next-generation" nets
- WHO recommends that several types of "next-generation" nets should be distributed instead of standard LLINs in areas of pyrethroid resistance (more above). Our analysis currently focuses on PBO nets, because other types of next-generation nets were only recently (in March 2023) recommended by WHO.187
We account for next-generation nets in our analysis by:188
- Collating data from combined pyrethroid and PBO (“synergist”) bioassays conducted between 2015 and 2019 that were conducted alongside standard pyrethroid-only bioassays.189 We then compare the average level of mosquito mortality between synergist and pyrethroid-only bioassays. Our analysis implies that, in areas where the tests were conducted, PBOs substantially lessen the reduction in net effectiveness from insecticide resistance compared to standard LLINs (from 22% to 62% to 4% to 50% across countries, and from 45% to 4% in Uganda).190
- PBO effectiveness varies depending on the type of insecticide resistance present. We would guess that synergist bioassay results are skewed toward areas where PBO is more likely to be effective.191 We add a downward adjustment to account for the difference between the areas where these assays were conducted within each country and the country as a whole. We estimate that PBOs are more effective than standard LLINs in 12 to 90% of areas across countries (82% in Uganda, details in footnote).192
-
Roughly estimating the proportion of PBOs that we expect our grantees to purchase for distributions in each country (19% to 100% across countries, 100% in Uganda).193 We update this figure during a grant investigation for a given opportunity, and so this estimate is likely to change over time. For Uganda, we most recently assessed this for an October 2021 grant (for distributions to take place in 2023),194 and so these proportions do not necessarily reflect the mix of nets that our grantees will purchase in the future.
- In DRC (although not in other countries, reasoning in footnote),195 we also account for chlorfenapyr nets. Our current guess is that chlorfenapyr nets completely eliminate the reduction in effectiveness from insecticide resistance. However, our analysis of chlorfenapyr nets is still ongoing, and this conclusion could change. We factor these nets into our analysis for DRC using a rough guess that AMF is likely to purchase 45% chlorfenapyr nets in its next DRC campaign. This results in an overall insecticide resistance adjustment of -4%.196
- WHO recommends that several types of "next-generation" nets should be distributed instead of standard LLINs in areas of pyrethroid resistance (more above). Our analysis currently focuses on PBO nets, because other types of next-generation nets were only recently (in March 2023) recommended by WHO.187
We account for next-generation nets in our analysis by:188
- As discussed above, WHO released new recommendations in March 2023 to deploy two types of next-generation, dual ingredient nets in areas of insecticide resistance.197 We expect our grantees will purchase at least some of these nets in future distributions. However, we have not yet fully incorporated the likely impact of next-generation nets in our analysis (only in DRC, and only using rough initial estimates of the impact of chlorfenapyr nets). We plan to update our analysis with more data in the future.
- The relationship between insecticide resistance and net effectiveness is unclear. There are reasons to think that pyrethroid-only LLINs could maintain some effectiveness even against resistant mosquitoes. For example, the insecticide may repel mosquitoes (and cause them to seek out other targets) even when it does not kill or fully disable them.198 Our current approach uses the simplifying assumption that effectiveness declines linearly with mosquito mortality (with the exception of the protection provided by the net’s physical barrier).
- We assume that PBO nets in upcoming distributions will be targeted to areas where the type of insecticide resistance that is susceptible to PBO is present.199 This assumption is based on our understanding that our grantees have been careful about selecting locations for PBO distributions, but in reality, targeting of PBOs is unlikely to be perfectly accurate.
- Our adjustment estimates ITN effectiveness relative to the studies in the Pryce et al. meta-analysis and is premised on the assumption that insecticide resistance was not present in the studies in the meta-analysis. However, our analysis suggests that one of the five main studies we rely on from the meta-analysis may have taken place in the context of insecticide resistance, and in two more studies the level of resistance is unknown.200 This implies that we could be overestimating the growth in insecticide resistance and therefore underestimating contemporary ITN efficacy. We account for this separately in our analysis with an upward adjustment of 5%,201 but this is a rough and uncertain guess.
Adjusting for study quality and generalizability
Our cost-effectiveness analysis includes two additional adjustments to account for the possibility that the effects estimated in Pryce et al. 2018 do not reflect the true impact of net distributions on malaria:
- Internal validity. We adjust our estimate of the impact of ITN distributions downward by 5% to account for internal validity. This accounts for there being some chance that the estimate from Pryce et al. might not have been the true effect ITNs had on the populations being studied. We think the studies included were high quality, and so our best guess is that the meta-analysis captures something close to the true effect in the study settings. Although we don't have specific, serious concerns about internal validity, we use a default value below 100% based on our expectation that, in general, published studies are more likely to overstate an intervention's efficacy than understate it.
- External validity. We include a further 5% downward adjustment to account for possible residual differences between the studies in Pryce et al. and contemporary distributions. This adjustment is relatively small because we separately account for the most significant ways in which the studies might not reflect contemporary distributions.202
The impact on malaria mortality
The starting point in our analysis is the impact of nets on malaria cases, not on deaths (more above). To account for this, we make the additional assumption that using nets reduces malaria mortality by the same proportion that it reduces malaria incidence (e.g., if ITNs reduce malaria cases by 50%, they also reduce malaria mortality by 50%). Our reasoning for this is:
- It seems plausible that a reduction in clinical malaria would result in a similar reduction in malaria mortality. We're not aware of evidence that ITNs disproportionately prevent non-severe cases of malaria.
-
The estimated reduction in uncomplicated malaria cases in Pryce et al. (45%) is very similar to the reduction in severe malaria episodes (44%, 95% CI 18% to 62%, although only two studies measured this outcome).203 This strengthens our confidence that ITNs don’t disproportionately prevent mild cases (which are unlikely to lead to death) relative to severe cases (which can lead to death).
What is the mortality rate among children who would benefit from nets?
We estimate that the risk of death from malaria and related causes for children who do not have access to nets is 0.31% to 0.88% per child per year (varying by location).205
A summary of our calculations for one country (Uganda) is below:
| What we are estimating | Value (rounded) |
|---|---|
| Baseline annual risk of death from malaria for children under age five | 0.24% |
| Number of deaths indirectly caused by malaria for every direct malaria death | 0.75 |
| Subtotal: Risk of death attributable to malaria (directly and indirectly) | 0.41% |
| Proportion of children using nets at the time of the GBD model in Uganda | 70% |
| Reduction in malaria mortality from using nets (discussed above) | 51% |
| Total (mortality rate attributable to malaria among children not sleeping under nets) | 0.64% |
This is based on:
- Estimates from the Institute for Health Metrics and Evaluation (IHME)'s 2019 Global Burden of Disease (GBD) model. This gives baseline estimates that a child’s risk of death from malaria in countries with the largest GiveWell-funded programs is 0.16% to 0.37% per year, varying by location (more).206
- Indirect malaria mortality: We estimate that malaria causes 0.75 deaths attributed to other causes for every death directly attributed to malaria. This suggests that ITNs could avert more mortality than might be expected from malaria deaths alone (more).
- An adjustment for higher mortality among children who don’t use nets. Our understanding is that the GBD estimates are for the overall mortality risk in a given location. We are interested in mortality rates among children who don’t use nets, which we would expect to be higher. We include a separate adjustment for this, based on reverse engineering mortality rates among children who don’t use nets from the effectiveness of nets against malaria and the proportion of children who we think used nets at the time of the GBD model (more).
- An adjustment to account for the impact of another malaria program, seasonal malaria chemoprevention (SMC), which is not currently incorporated into the GBD estimates. This reduces our estimate of baseline mortality in countries with SMC programs. (More)
Baseline malaria mortality for children under age five
Our estimates of annual malaria mortality for children under five are drawn from the Institute for Health Metrics and Evaluation (IHME) Global Burden of Disease (GBD) project.207 We use 2019 national-level estimates for malaria mortality among 1-59-month-olds with the exception of Nigeria, where we use state-level estimates.208 This provides estimates of annual malaria mortality of 0.16% to 0.37% (varying by location).209
These estimates are a source of significant uncertainty in our analysis:
- Our understanding is that the GBD estimates rely on a number of modeling assumptions,210 in part because raw data on malaria from health surveillance systems is relatively unreliable in many low-income countries.211 We have not investigated all the modeling assumptions underlying these estimates in detail and we’re not sure how accurately GBD can attribute deaths to specific causes.
-
GBD estimates of malaria incidence and mortality imply significant variation in the case fatality rate across countries. The implied case fatality rate for children under five varies from 0.22% (Togo) to 0.60% (Chad), with an average of 0.41%.212 We would expect some variation across contexts (e.g., because of transmission intensity and variation in health systems), but we’re unsure whether this level of variation is capturing real differences across contexts or statistical noise. We have not investigated this question in depth.
An additional uncertainty is how the GBD estimates compare to other sources. In 2023, GiveWell commissioned Rethink Priorities to conduct a research project comparing the GBD estimates to widely-used estimates of malaria mortality from WHO.213 Our understanding had been that the WHO estimates were generally lower than the IHME estimates. We were concerned that we could be systematically overestimating malaria mortality by using GBD estimates only.
Overall, the report reduced our concern about this issue. The main findings of the report were:
- WHO’s estimates were historically significantly lower than GBD estimates (17% lower in 2019), but went through a significant methodology change in 2021 that has narrowed the gap.214
- The gap between sources is largest in areas outside sub-Saharan Africa, where the malaria disease burden is lower (and where GiveWell does not fund ITNs).215
- GBD estimates tend to record lower deaths among children under five, and higher deaths among older children and adults.216 This might be the result of GBD using verbal autopsy reports to inform its estimates, whereas WHO (and some other researchers) believe that these can’t distinguish between malaria and other febrile illnesses.217
While we’re still uncertain about the reliability of each source, and the verbal autopsy question, we opted not to change data sources following this project. The benefits of ITNs are concentrated in children under five (where the gap between WHO and GBD is smaller), and so we think that switching would not not lead to major changes in our bottom line.
Indirect malaria mortality
Malaria control interventions often have a larger effect on all-cause mortality than would be expected exclusively from declines in malaria-specific mortality.218 Deaths may have several causes, while only being attributed to one cause. For example, malaria may increase the likelihood of death from malnutrition or other infectious diseases.219 We account for this with an estimate that for each death directly caused by malaria, an additional 0.75 deaths are indirectly caused by malaria.220
We are highly uncertain about what the exact value for this effect should be. Our estimate of 0.75 is based on triangulating three different sources of information:
- Our analysis of the relationship between all-cause mortality and malaria incidence in Pryce et al. implies a value of up to 1.5 indirect deaths for every direct malaria death.221
Our best guess is that this is an overestimate, because:
- The studies underlying the Pryce et al. meta-analysis took place in the 1980s, 1990s, and 2000s.222 It is plausible that the ratio of direct to indirect deaths has fallen since that time in malaria-endemic countries as overall health has improved and under-five mortality has decreased.223
- We use national-level estimates from the Global Burden of Disease project from the countries where the studies in Pryce et al. were conducted as inputs to our analysis (see here). Intuitively, we might expect the Pryce et al. RCTs to be conducted in areas where malaria mortality was higher than the national average. If that assumption is correct, our analysis would be likely to overestimate the share of indirect deaths and underestimate the share of direct malaria deaths.
-
We have also spoken with malaria experts who told us that it is widely accepted there are roughly 0.5 to 1 indirect malaria deaths for every direct malaria death.224
- Our analysis of water chlorination programs, another intervention that reduces child mortality by averting infectious diseases, suggests a ratio of 2.7 deaths indirectly averted for every death directly averted from enteric infection.225 This leads us to believe that a high ratio of indirect to direct deaths is plausible.
Taking all three sources of information into account, we use a value of 0.75 as our best guess for the ratio of indirect malaria deaths to direct malaria deaths for contemporary ITN distributions.226
Adjustment to account for higher mortality among children who don’t use nets
The GBD malaria mortality estimates that we use aim to capture the overall malaria mortality rate in each country. These estimates already incorporate the expected benefits of net distributions227 (taking into account that some people are already protected by ITNs and therefore have lower mortality). By contrast, we are interested in the impact of increasing access to nets among children who would not otherwise use them. We therefore need to estimate mortality among children who are not protected by nets (and who we would expect to have higher mortality rates than average).
We therefore include an adjustment to estimate the mortality risk for children who would not otherwise use nets.
Our adjustment uses (i) GBD estimates of the proportion of children under five who slept under a net the previous night in each country (ranging between 47% and 80% by location) and (ii) the estimated protective effect of using a net in each country.228 This allows us to "reverse engineer" mortality among children who do not use nets.229
Overall, this adjustment increases our mortality estimates in all locations, aligning with our expectation that mortality rates would be higher among children who don’t use nets. For example, in Uganda the mortality risk rises from 0.41% for all children to 0.64% for children who don't use nets.230
Our main reservations about this adjustment are:
- We have not carefully vetted the IHME usage estimates we use. We are uncertain about how representative the estimates are of net usage in each country, and we have not investigated the methodology used to estimate them.
- The calculation we use does not take into account the community-level protective effect of using ITNs and only considers the benefit to the individual user.231
- In effect, this adjustment is attempting to "undo" the incorporation of previous ITN distributions into the GBD 2019 estimates. It is possible that we have done so incorrectly.
The impact of seasonal malaria chemoprevention
Several countries included in our cost-effectiveness analysis also deliver another malaria intervention, seasonal malaria chemoprevention (SMC).232 Our understanding is that the GBD 2019 malaria mortality estimates do not include the expected impact of SMC campaigns (which have been rapidly scaled up in some countries, particularly Nigeria, in recent years),233 as they do for ITN distributions.234 Failing to account for this would mean our analysis would risk overestimating malaria mortality and (by extension) cost-effectiveness.
We account for this with an additional adjustment, representing the deaths we expect would be averted by SMC in countries where both ITNs and SMC are distributed.235
4.3 Impacts on mortality for older children and adults
Overall, we estimate that each $1 million spent by AMF averts ~50 to ~160 deaths of older children (over age five) and adults.236 A summary of our calculations is below, using one country (Uganda) as an example:
| What we are estimating | Value |
|---|---|
| Averted deaths among children under age five per $1m in Uganda (discussed above) | 294 |
| Number of malaria deaths among over-fives in Uganda per under-five malaria death in Uganda | 0.3 |
| ITN effectiveness at reducing mortality for over-fives, relative to under-fives | 80% |
| Total (over-five deaths averted) | 70 |
While children under the age of five are disproportionately at risk, malaria is also a mortality risk to older children and adults.237 We estimate the impact of ITNs on mortality for people age five and older using the following method:
- Benchmarking based on under-five mortality averted by ITNs. For each country in our analysis, we take the estimated ratio of over-five to under-five malaria deaths from Global Burden of Disease Project data.238 We multiply this value by our previous estimate of the number of under-five deaths averted by ITNs per cohort.
- Adjusting for lower efficacy for over-fives. We adjust our estimate downwards by 20% because we believe that ITNs may have lower efficacy for older children and adults. We are very uncertain about this adjustment, for which we have not seen any estimates from published research. Our understanding is that there is minimal empirical evidence on the level of protection provided by ITNs to adults.239
Our adjustment is based instead on three considerations that we think could plausibly affect efficacy by age:
- Later sleeping times: We expect that older children and adults are less likely than young children to be asleep during the hours when mosquitoes are most likely to bite.240
- Lower net usage: It is plausible that older children and adults sleep under ITNs less frequently than young children.241
- Community-level effects: One counteracting factor is that we expect some of the protection provided by ITNs to be a community-level effect (from the overall number of mosquitoes and level of malaria in the community being lower).242 This implies some protection against malaria regardless of an individual’s net usage.
See this section of our cost-effectiveness analysis for our full calculations.243
4.4 Long-term income increases
Summary
Our best guess is that averting childhood malaria cases leads to small income gains in adulthood. This contributes a substantial share of our estimated benefits for malaria programs. As of December 2023, we estimate that these benefits account for ~25% to ~40% of the total modeled benefits244 of distributing ITNs.245 In Uganda, our 25th - 75th percentile confidence interval is that this accounts for 19% - 42% of the total modeled benefits of distributing ITNs, with a best guess of 32%.246
To create our best guess on the effect of reductions in malaria on later-life income, we rely on evidence from two historical quasi-experiments, Bleakley 2010 and Cutler et al. 2010, that measure the effect of eradicating malaria on later-life income in the Americas and India. Based on this evidence, we estimate that each case of childhood malaria averted increases adult income by 0.6%, and that these benefits persist over 40 years of an individual’s working life. A summary of our calculations is below, using one country, Uganda, as an example:
| What we are estimating | Value (rounded) |
|---|---|
| Arbitrary donation to Against Malaria Foundation (AMF) | $1,000,000 |
| Total child years of protection by nets (Age <5) (discussed above) | ~89,000 |
| Total child years of protection by nets (Age 5-14) | ~150,000 |
| Increase in annual income per childhood malaria case averted (more) | 0.6% |
| Baseline counterfactual malaria incidence (Age <5) (more) | 103% |
| Baseline counterfactual malaria incidence (Age 5-14) (more) | 43% |
| Reduction in malaria incidence for people using nets (more) | 51% |
| Malaria cases averted by nets (Age <5) | ~47,000 |
| Malaria cases averted by nets (Age 5-14) | ~33,000 |
| Years until long-run income benefits start (more) | 10 |
| Years of long-term benefits (more) | 40 |
| Discount rate on future economic benefits (more) | 4% |
| Multiplier for resource sharing within households (more) | 2 |
| Totals | |
| Total children receiving a 0.6% long-term income increase | ~80,000 |
| Moral weight on a 0.6% increase in adult income | 0.23 |
| Total units of value from income increases per year | 18,551 |
| Total units of value from deaths averted (see here) | 39,269 |
| % of total modeled benefits from long-term income increases | 32% |
Intuitively, we think it is plausible that long-term income increases constitute an important share of the benefits of ITNs because:
- It seems plausible that averting malaria during a sensitive period of childhood development could improve long-run outcomes. Though we haven't deeply investigated potential mechanisms and the chain of causation, we know that malaria can cause fever, anemia, enlarged liver or spleen, kidney injury, and severe neurological symptoms associated with cerebral malaria, among other morbidities.247 Avoiding these symptoms could benefit physical and/or cognitive development. (More)
- Several additional quasi-experimental studies beyond Bleakley 2010 and Cutler et al. 2010 support direct effects of eradicating malaria on later-life income. (More)
- Our bottom-line long-term income effect size is broadly consistent with our findings for other programs for which we analyze long-run income effects, as well as macroeconomic trends in the relationship between malaria burden and economic growth. (More)
- While we value a small increase in adult income much less than averting a death, nets avert many more childhood malaria cases than deaths, adding up to a large total benefit.
Our main uncertainties about this evidence are:
- The best direct evidence we're aware of comes from two natural experiments, but these estimates are subject to several limitations, including that they are not guaranteed to be causal, use imprecise historical data to measure past income and disease burden, and may be subject to publication bias.
- Both studies are based on early-to-mid 20th century malaria programs outside of sub-Saharan Africa, and we are uncertain about how well the effects they estimate translate to today's contexts.
- We've only done a partial literature review for the long-term income effects from averting malaria, and it's possible that we'd update our effect size if we incorporated more evidence, particularly if we did a deeper investigation into the income effects of interventions that target other aspects of childhood health besides malaria.
Increase in annual income per child malaria case averted
The key parameter in our analysis of malaria's long-term economic effects is our estimate of a 0.6% increase in adult income per malaria case averted among children ages 0-14. This effect is based primarily on the findings of two natural experiments on the historical effects of malaria eradication on economic outcomes, Bleakley 2010 (U.S., Brazil, Colombia, and Mexico) and Cutler et al. 2010 (India) (more), which we adjust downward to account for our uncertainty about the quality of this evidence (more). The second important component of our reasoning is a sense check of our bottom line estimate against benchmarks from other GiveWell investigations and macroeconomic trends (more).
We make several uncertain assumptions to interpret the headline Bleakley and Cutler results. Under our assumptions, Cutler and Bleakley together imply an average 2.15% income effect per malaria case averted in childhood. We adjust this downward with a replicability adjustment of -70% and an external validity adjustment of -10% to reach our final estimate of a 0.6% income effect, as shown in the following table:
| What we are estimating | Bleakley | Cutler et al. | |
|---|---|---|---|
| Long-run income effect from eradicating malaria in childhood (more) | 16% | 4.2% | |
| Number of years in childhood (more) | 15 | 15 | |
| Annualized income effect size | 1.1% | 0.3% | |
| Corresponding reduction in population malaria incidence (more) | 36% | 10% | |
| Approx. ratio of malaria rates for ages 0-14 vs. all ages (more) | 135% | 135% | |
| Corresponding reduction in malaria incidence for ages 0-14 | 48% | 14% | |
| Long-run income effect per malaria case averted for ages 0-14 | 2.2% | 2% | |
| Weight on result (more) | 60% | 40% | |
| Subtotal: Increase in annual income per malaria case averted between ages 0 and 14, pre-adjustments | 2.15% | ||
| Replicability adjustment on malaria income effect (more) | -70% | ||
| Adjustment for external validity (more) | -10% | ||
| Total (Adjusted increase in annual income per malaria case averted between ages 0 and 14) | 0.6% | ||
Long-run income effect from eradicating malaria in childhood
16% and 4.2% represent the headline income effects in Bleakley and Cutler et al., respectively, which are based on difference-in-differences analyses comparing economic outcomes for cohorts born pre- and post- malaria eradication in malarious vs. non-malarious areas of each historical setting. To the best of our knowledge, these two papers represent the best available direct evidence of the relationship between malaria and long-run income. We provide more detail on these estimates below:
Bleakley 2010 analyzes the impact of four 20th century malaria elimination campaigns: the U.S. South in the 1920s and Colombia, Brazil, and Mexico in the 1950s. The paper finds that the campaigns were successful at reducing malaria rates and that cohorts who benefitted from reduced exposure saw faster income gains in adulthood relative to their peers in non-malarious areas.249 We focus on Bleakley's U.S. estimate among the four countries he studied because the U.S. historical malaria data appeared to be more accessible and reliable, and Bleakley's headline income effect estimates didn't vary much across countries.250
For the historical U.S., Bleakley reports an average difference in long-run income of 16% (a result of 14% or 18% depending on the economic indicator used) between areas with 95th and 5th percentile pre-eradication malaria burden, based on an average of difference-in-differences ordinary least squares (OLS) estimates.251 252 These results apply to cohorts of native-born white males and measure economic outcomes between ages 35 and 55.253
Cutler et al. 2010 uses a similar approach to Bleakley to assess the impact of the national malaria eradication program in India in the 1950s. The authors compare economic outcomes for cohorts born before and after eradication in areas with varying pre-eradication malaria prevalence. Their analysis suggests elevated economic gains (proxied by household expenditure rather than income because most of the sample did not work for wages) for men in districts that had higher pre-eradication malaria prevalence, although they do not find similar gains for women.254 The authors also find no evidence of improved educational attainment resulting from the campaign.255
Cutler et al. reports a 1.5% to 6.8% increase in consumption expenditure for men between ages 20 and 60 per 10 percentage point decrease in malaria incidence during the eradication period.256 We use the midpoint of this range, 4.2%, as our input for Cutler et al.'s result. The expenditure results vary considerably depending on which trends are included as control variables and whether the specification is OLS or uses instrumental variables, so we take the midpoint (details in footnote).257
There are good reasons to be cautious in using these studies as evidence that contemporary ITN campaigns will lead to economic gains. Both papers are retrospective, non-experimental studies assessing the impact of campaigns that took place decades ago and that did not use ITNs (the main intervention used was spraying of DDT insecticide).258 We believe that there are limits to the reliability and precision of estimates that we can obtain from this kind of evidence. Our specific uncertainties are:
- We have not seen any randomized controlled trials on the long-term economic effects of reduced malaria exposure. Bleakley and Cutler are both retrospective, non-randomized studies which we believe are at elevated risk of publication bias. We are generally hesitant to rely on this kind of evidence in our analysis.259
- We have not done a thorough review of the available evidence on the long-term income effects of malaria. There may be other published studies we have not seen that would lead us to update our income effect estimates.
- Both studies only find evidence of economic gains for men (and in Bleakley’s U.S. analysis, only white men are included in the sample used for analysis).260 Cutler et al.’s estimates of the eradication campaign on women’s economic outcomes are approximately zero.261 The authors attribute this to women’s lower levels of labor force participation in the decades around the campaign.262 We find this explanation plausible, but it does limit our confidence that the study’s findings are robust and generalizable. Bleakley does not include women in the study’s analytical sample because women had lower levels of labor force participation in the study period.263
- Both studies rely on historical source data. We expect this to be relatively unreliable and imprecise.264
- Because both studies are based on early-to-mid 20th century programs outside of Sub-Saharan Africa, the income effects they estimate may not have external validity to today's contexts. We use a -10% adjustment for external validity, but this is a rough guess (more).
Despite our concerns, we think there are reasons to put some weight on these studies:
- Bleakley and Cutler et al. find positive impacts on economic outcomes that are similar in magnitude to one another. We think this adds some weight to there being a true effect.
- The studies have a plausible strategy for separating the effects of malaria infection from effects of other things (such as poverty) that may correlate with malaria infection. Specifically, they exploit the fact that the eradication campaigns caused a relatively rapid drop in malaria infection rates (which was plausibly exogenous because of technological advancement) and that areas with higher initial malaria prevalence saw greater falls in malaria prevalence.265
- GiveWell Senior Advisor David Roodman subjected Bleakley 2010 to intense scrutiny, conducting a detailed review and reanalysis (see blog post here and detailed report here) and concluded that the link between malaria eradication and economic gains was plausible.266
Number of years in childhood
Bleakley and Cutler et al. estimate the long-run effects of reduced malaria exposure in childhood, but they don't capture at exactly which ages reduced exposure is impactful. We roughly guess that long-term income effects accrue over 15 years of childhood among children ages 0-14. We assume an equal future income effect per malaria case averted during this window, as we have not seen any direct evidence of differential effects. However, this assumption is highly uncertain since we lack relevant evidence. It's possible that income increases are larger for cases averted in younger children, who are at an earlier stage of development.
Corresponding reduction in population malaria incidence
To scale the economic benefits found in Bleakley and Cutler and make them portable, we need to know how much malaria rates fell after eradication in these historical contexts to generate the income effects they find. We believe that the Bleakley results imply a 16% income effect from a 36 percentage point decline in population malaria incidence in the United States, and the Cutler et al. results imply a 4.2% income effect from a 10 percentage point decline in population malaria incidence in India.267 Once we normalize each income result to per-malaria-case-averted terms using the corresponding reduction in malaria, Bleakley and Cutler predict similar annual income increases of 2.2% and 2% per malaria case averted, respectively.
These incidence reduction estimates are quite rough and uncertain since we only have approximate historical data on pre-eradication malaria rates to rely on:
- We use Cutler et al.'s estimate of a 10 percentage point decline in malaria incidence to scale benefits from this study. We have not deeply investigated the authors' data validation process for malaria incidence.
- For Bleakley, we roughly estimate the amount of incidence averted using historical estimates of malaria mortality and case fatality rates for the early 20th century U.S. from a contemporary source, Maxcy 1923. See here for our assumptions and calculations.
We discuss how we convert these reductions in malaria incidence into income effects from ITN campaigns today in the section below.
Ratio of malaria rates for ages 0 - 14 vs. all ages
We further adjust the changes in malaria rates in Bleakley and Cutler et al. to account for the age profile of malaria burden, which we assume was more concentrated in young children than in adults. Both studies present income effects based on reductions in population malaria burden, while long-term income increases accrue to reductions in childhood malaria burden. We estimate that the malaria rate for under-5 children was twice the population rate, implying that historical malaria eradication averted 35% more malaria among children ages 0-14 than in the population at large (calculations). Several benchmark values suggest that our assumption is appropriate, but we're somewhat uncertain about the exact conversion rates we chose.268
Weight on result
We apply 60% weight to Bleakley and 40% weight to Cutler et al. to reach a weighted average final income estimate from the literature of 2.15%. We apply slightly more weight to Bleakley because we have subjected it to more scrutiny, but the Cutler and Bleakley estimates are consistent with each other, so this assumption makes little difference.
Replicability adjustment on long-term income effect
Combining the above assumptions yields a 2.15% income effect per malaria case averted from the literature. We then account for our uncertainty about the Bleakley and Cutler et al. estimates of economic effects with a -70% replicability adjustment that reduces the 2.15% long-run income effect to a 0.65% income effect (2.15% x (1﹣70%) = 0.65%). There are two components to this adjustment:
- A 40% (i.e., -60%) subjective validity adjustment to account for the evidence being non-randomized and from a long time ago. We're uncertain about the size of this adjustment and discuss our reasoning for it and its plausibility in more detail below.
- A 75% (i.e. -25%) adjustment to account for gender disparities in income effects. Both studies only find evidence of economic gains for men (Bleakley’s analytic sample does not include women, and Cutler et al. find an effect of approximately 0 for women). We think it is plausible that averting malaria cases today would result in economic gains for women that Cutler et al. did not find (e.g., because of women’s higher labor force participation today than when the campaigns were conducted), but there may still be reasons why women would not see economic gains as large as men. To account for this, we apply a further adjustment of 75% to our estimate based on our guess that the effect for women might be around half as large as for men, and women comprise ~50% of the population.
- Combining these two components, the implied adjustment factor is 40% x 75% = 30%, so our final replicability adjustment is a 70% reduction in the Cutler and Bleakley effect size.269
External validity adjustment for long-term income effect
We also apply a -10% external validity adjustment to our income effects estimate, yielding an overall 0.6% effect on income per malaria case averted (0.65% x (100% - 10%) = 0.6%).270
The reasoning for this adjustment is that multiple measures of malaria burden exist:
- Incidence (the annual rate of clinical malaria cases).
- Prevalence (the proportion of people with detectable malaria parasites in their blood at a single point in time, regardless of symptoms).
In our analysis below, we translate Bleakley and Cutler’s findings into estimates of income effects today based on the number of clinical malaria cases that we think our funding will avert (incidence). But it’s possible that we should also put some weight on expected changes in malaria prevalence. This distinction is important because the Cochrane meta-analysis finds that ITN campaigns reduced malaria incidence considerably more than prevalence (45% vs 17%).271 We think the reduction in malaria incidence studied in Bleakley and Cutler would have been accompanied by a larger reduction in malaria prevalence than we would expect today. This suggests we would be overestimating the effect of ITNs on income by using an unadjusted estimate from Bleakley and Cutler’s findings.
We roughly estimate that 80% of the factors leading to income effects are correlated with changes in malaria incidence, and 20% are correlated with changes in prevalence. We also estimate that ITN campaigns avert roughly half as much malaria prevalence per malaria case averted today as the historical eradication campaigns. Together, this implies an overall income effect of 0.6% ((0.65% x 80%) + (0.65% x 20% x 50%)) per malaria case averted today. This equates to a -10% adjustment.
In more detail:
- We think it makes sense to put most weight on changes in malaria incidence.
- We believe the historical data on malaria burden that we rely on tracked something similar to population malaria incidence, because symptomatic malaria cases are easier to directly observe than alternatives in settings with limited technology.272 This means it makes sense to scale today's income benefits using comparable changes in malaria incidence burden.
- We also intuitively think that malaria episodes rather than passively carrying malaria parasites is likely to drive most of the negative health impacts of malaria that could impair development.
- But there may also be reasons why changes in malaria prevalence are correlated with income effects.
- After an active malaria infection, a person may still harbor malaria parasites for months, particularly if they don't receive treatment.
- Our understanding is that asymptomatic infections like this could suppress the immune system and make the host more susceptible to other infections, although we have not investigated this in detail.273
- Our best guess 80% / 20% split between incidence and prevalence is a rough and uncertain guess, based on our analysis of the burden of mortality caused directly by malaria vs indirectly from other infectious diseases (details in footnote).274
- Finally, we roughly estimate that ITN campaigns today avert half as much malaria prevalence per malaria case averted as the historical eradication campaigns analyzed by Bleakley and Cutler. We think that the income effects captured by these papers reflect both malaria incidence and prevalence falling to ~0% (because the campaigns led to malaria eradication). By contrast, the Cochrane meta-analysis finds that ITN campaigns reduce malaria incidence about 2.5x more than prevalence (45% vs 17%). We would guess that this ratio has fallen to 2x since the Cochrane studies were conducted (largely in the 1990s) as malaria treatment has become more widely available (since successful treatment clears the initial infection). This is a rough guess.
Counterfactual malaria incidence
We estimate a baseline annual malaria case rate of 103%275 for under-5s and 43% for ages 5-14 in Uganda in the counterfactual where nets are not distributed.276 We rely on Global Burden of Disease (GBD) estimates of malaria incidence as the basis for this value, but these estimates incorporate reductions in malaria burden from past net distributions. This means that baseline incidence in the absence of a distribution would be higher than reported incidence, so we adjust the GBD estimates upwards to capture counterfactual malaria rates if we did not fund net distributions in Uganda. We use the same process and assumptions to "reverse engineer" malaria incidence rates for people not using nets that we describe for our mortality estimates and have the same uncertainties.
Reduction in malaria incidence
We estimate the malaria reduction from net distribution in order to scale long-term income increases to each context. For AMF in Uganda, we estimate that sleeping under a net reduces malaria incidence by 51% (the same estimate that we use for malaria mortality discussed above).
Duration of benefits
- We assume that on average there are 10 years between receiving nets and when children start working and begin to accrue economic benefits:
- We assume children between the ages of 0 and 14 benefit from the long-run effects of reduced childhood exposure to malaria. Taking a simple average, we expect the average beneficiary is approximately 7 years old.
- Our best guess is that children are roughly 17 years old when they begin substantive work.277
- Our best guess is therefore that on average there are 10 years between receiving nets and starting work.
- We assume that economic benefits last for the beneficiary's full career. We roughly guess that people work for about 40 years.
- This is the same assumption we use for deworming.
- We apply a -10% adjustment for benefits decaying over time to deworming but not to malaria because historical evidence for the long-term income effects of malaria already accounts for economic outcomes over roughly the full career.278
Discount rate
- We calculate the present value of the stream of future income increases over each beneficiary's career by applying a 4% discount rate.
- This is the same rate we use for all economic benefits (described here).
Multiplier for resource sharing within households
- This multiplier accounts for people who receive long-term income increases from avoiding malaria in childhood sharing that benefit with future family members. Our assumed multiplier of 2 can be interpreted as each person receiving long-term income benefits contributing 50% of household income for a family of ~4 people over time.
- The value of 2 we chose is based on the same reasoning we use for deworming, described here.
Sense checks
It's important to think about the plausibility of the long-term income increases we've modeled due to our uncertainty about the evidence and how we've translated it to current programs. We adopt a cluster thinking approach to benchmark plausible effect sizes. This includes quantitative and qualitative benchmarks.
Quantitative sense checks
Our starting point is the 0.6% income effect size implied by Cutler and Bleakley and our subjective adjustments. We benchmark that in three ways:
- Benchmarking against other income effects we've modeled. We compared the bottom-line 0.6% income effect per malaria case averted to other programs we've considered with long-run income effects. This benchmarking exercise makes us think the 0.6% effect is broadly appropriate and consistent, though it involves making intuitive comparisons between the relative benefits of averting different types of health conditions in childhood. This estimate is comparable to our income estimates for:279
- Deworming: Averting one moderate intensity worm infection in a school-aged child for ~8 months. This seems consistent to us because we expect malaria symptoms to be more acute but last a shorter time (<1 month vs. a full year).
- Iron fortification: Averting a case of anemia for ~7 years in childhood. This is a rough estimate and we haven't deeply investigated the severity of these anemia cases. Our best guess is that on average this would be a case of mild anemia near the moderate threshold. We'd guess that 7 years of anemia cause more short-term morbidity than a single malaria episode, so the consistency of this comparison rests on the appropriateness of our assumption that the cognitive benefits of iron specifically aren't very durable—only ⅓ persist to adulthood.
- Low birthweight. Increasing birth weight by 2 oz, or ~7% of the distance from the low birth weight cutoff to average birth weight. Growth vs. disease are different, but this comparison seems reasonable because they both seem like moderate differences in respective outcomes (a modest birth weight increase vs. averting one disease episode).
- Sense-checking against macro evidence. Our 0.6% estimate for long-term income increases implies that nets have caused plausible rates of economic growth in sub-Saharan Africa since they were broadly introduced in the early 2000s.
- Annual malaria incidence has fallen by ~25 percentage points (a 40% drop) in Africa since 2000,280 which under our assumptions implies up to a 2.25% increase in GDP per capita for people who experienced reduced malaria burden throughout childhood. The population average is likely smaller, roughly 1%, because most current cohorts were not exposed to malaria interventions since birth.281
- Simultaneously, purchasing power parity adjusted per capita income in Africa has roughly doubled since 2000.282
- Comparing the two changes, reduced malaria is <3% of the explanation for the increase in GDP per capita over time, which doesn’t seem like an implausibly large effect.
- Our estimate of 1% to 2% growth from decreased malaria burden compares reasonably well to macro evidence on the relationship between malaria and GDP (details in footnote).283
- Benchmarking against other internal validity adjustments. We use a 40% internal validity adjustment for long-term income increases (the first component of our replicability adjustment). We compared our assessment of the quality of evidence and our chosen internal validity adjustment to other interventions we've looked at. This makes us think a value of ~40% is appropriate.
- Broadly, we have (as of December 2023) an internal validity adjustment range of 95% (-5%) for SMC (which is supported by a meta-analysis of multiple recent RCTs that report plausible effect sizes) to 13% (-87%) for deworming (which is supported by one RCT in an unusually high-burden setting with an implausibly large effect size). In between, we have set an internal validity adjustment of 74% (-26%) for vitamin A supplementation (which is also supported by a meta-analysis of multiple RCTs, but they were conducted long ago and the effect size they imply is somewhat implausible).284
- The quality of the evidence for long-term income increases from avoiding malaria in childhood is somewhere in between the extremes of our range, featuring two quasi-experiments, evidence of reduced malaria morbidity as a potential mechanism, and a plausible effect size. We think the quality of this evidence is weaker than for SMC and vitamin A supplementation, which are both supported by a meta-analysis of many RCTs, but stronger than for deworming, since even though there is no RCT, the income effect size for malaria is not nearly as implausibly high as for deworming.
Qualitative sense checks
We have also explored qualitative benchmarks that give us additional confidence that long-term income increases from averting malaria are meaningful. Each of these indicators suggests that there is some effect, though we have not tried to translate them into quantitative estimates of the effect size.
- Plausibility of mechanisms. We haven't deeply investigated potential mechanisms, but we've confirmed that malaria causes severe morbidities, and it seems intuitively plausible to us that some of these conditions could affect early life development.285
- Additional evidence. Several quasi-experimental studies support direct effects of eradicating malaria on later-life income. We did a shallow review of other literature on the income effects of both malaria and other health conditions and summarized it in this spreadsheet.
- There are several additional studies related to the long-run effects of malaria on economic or intermediate proxy outcomes that we have not incorporated into our analysis, as well as evidence on other infectious diseases and nutrition.
- To the best of our knowledge, there isn't higher quality evidence than Cutler and Bleakley or randomized evidence available on the connection between malaria and long-run income.
- Nevertheless, we are aware of a relatively large body of literature on this question, and the majority of sources seem to support that there are long-term income gains from improved childhood health, though no individual piece of evidence is necessarily very high-quality.
- But some papers that don't find effects and other potential null effects could be missing from the literature due to publication bias, which makes it less likely that studies finding null results will be published.
- To date, we haven't looked at these studies in detail or tried to quantify the size of the income effects they imply.
Key uncertainties and future research
Our key uncertainties that could have a big impact on our analysis of long-term income increases from ITN distribution are:
- Evidence quality and internal validity. We believe that Bleakley and Cutler et al. represent the most compelling existing evidence on the relationship between childhood malaria and long-term income, but we have several concerns about this evidence and whether it accurately estimates the long-run income effects of childhood malaria interventions. We have applied a replicability adjustment to account for these concerns, but it's possible that our adjustments could be substantially wrong in either direction:
- We include a -70% internal validity adjustment largely to account for publication bias, which may prevent us from seeing null evidence and cause us to overestimate the long-term income effect when looking only at positive studies. We're uncertain about this adjustment, though we believe it is most likely to fall within +/-15 percentage points of our chosen value.
- We make the uncertain assumption that women receive half of the long-run income benefits of men. Bleakley did not study outcomes for women, and Cutler et al. did not find much evidence of expenditure effects for women in a context with limited female labor force participation. This parameter could cause our income effect estimate to be off by up to 25%, if women in current programs either do not receive income benefits due to restricted labor market access or receive the same benefit as men.
- External validity. We are uncertain how well evidence on historic income gains from malaria eradication translates to current malaria programs. We have included a -10% external validity adjustment because net distributions probably reduce malaria prevalence less than historical eradication campaigns. There are several other differences that could be important, but we have not included an additional external validity adjustment because we believe there are compelling arguments for today's long-term income effects differing in either direction. There are several key points of difference in programs and settings:
- Both Cutler et al. 2010 and Bleakley 2010 study settings where p. vivax is the predominant strain of malaria, while our top charities work in countries where p. falciparum is endemic. We are uncertain whether the effect of p. falciparum is higher or lower than the effect of p. vivax on long run income. P. falciparum has a higher mortality rate than p. vivax. If malaria deaths are more likely in low-income households (who we would expect to have worse overall health and be at higher risk of malaria mortality), we would expect (all else equal) preventing these deaths to reduce average income.286 But p. falciparum causes more serious morbidity than p. vivax, which we would guess has a larger effect on long-run cognitive development.287
- The programs studied were different. Bleakley and Cutler studied large-scale malaria eradication efforts using DDT insecticide that removed all malaria exposure during childhood, not ITN distributions that have more moderate effects on malaria over a shorter time interval. It's possible that we're misinterpreting these effect sizes by annualizing them for each year of ITN coverage (i.e., assuming that one year of protection from malaria confers 1/15th of the effect of 15 years of protection).
- The economic context was also different in Cutler and Bleakley. We are uncertain how occupational differences between then and today (e.g., the proportion of workers employed in agriculture) may affect our estimates.
- Technology has advanced since the early-to-mid 20th century. In particular, more malaria tests and treatments are now available. Improvements in malaria treatments also have an ambiguous effect on income. Modern treatments may reduce the morbidity from infection and its negative effects on childhood development relative to historical settings, decreasing long-term income effects. However, more children with severe infections likely died due to lack of treatment in historical settings, reducing estimated historical income effects because the children who stood to gain the most from malaria eradication didn't survive to adulthood.
- Given all these uncertainties, we think a 25th/75th percentile range for the external validity adjustment is -30% to +10%.
- Historical malaria incidence. We are uncertain about the pre-eradication malaria burden estimates for children that we use to scale long-term income increases. It seems likely that these estimates could be off in either direction. We think a 25th/75th percentile range for historical malaria incidence averted is +/- 20% of our central estimates (29% to 43% for Bleakley and 8% to 12% for Cutler).
- Assumptions related to mortality benefits. Many of the key uncertainties that apply to our mortality benefits for nets also apply to long-term income effects, because we rely on the same assumptions to estimate the number of malaria cases that nets avert.
We skipped some work during this investigation that could potentially update us. We may prioritize looking into some of these questions in the future:
- Doing a deep dive and thorough review of the literature on the long-term income effects of childhood health conditions.
- Looking at evidence for intermediate outcomes like growth, cognition, schooling, etc. We haven't deeply investigated the potential mechanisms behind the impact of malaria on income. It's possible doing so would update us on the plausibility of different mechanisms and help us benchmark against how large an income effect we'd expect from each probable intermediate outcome.
- Funding more follow-up research on the relationship between childhood malaria and adult economic outcomes, especially randomized evidence.
- Getting expert feedback on our assumptions.
4.5 Supplemental intervention adjustments
Summary
Our cost-effectiveness analysis includes a number of additional adjustments that we have opted not to explicitly model.288 Instead, we incorporate these adjustments as rough best guess percentages.
As of December 2023, these adjustments increase our estimate of the impact of ITN distributions by 38% in Uganda. The impact across countries ranges from 38% to 48%.289 See the table below for a summary.
| What we are estimating | Value |
|---|---|
| Reduced malaria morbidity | 9% |
| Short-term anemia effects | 9% |
| Prevention of diseases other than malaria | 2% |
| Prevention of stillbirths | 9% |
| Investment of income increases | 3% |
| Treatment costs averted from prevention | 20% |
| Subnational adjustments | 2% |
| Mosquito insecticide resistance in trials underlying our estimates | 5% |
| Rebound effects / decreased immunity development | -4% |
| Marginal funding going to lower priority areas | -5% to -15% |
| Differences in mosquito species | -2% |
| Total (adjustment for supplemental benefits) | 38% (Uganda) |
We are particularly uncertain about these adjustments (details on our method in footnote)290 and they should be thought of as rough best guesses. See this spreadsheet for our full calculations.
Additional benefits
As of December 2023, we include the following additional benefits in our analysis:291
- Malaria morbidity (+9%). ITN distributions result in averted morbidity by reducing malaria cases. This includes averted morbidity from cerebral malaria, which can involve significant neurological and cognitive impairments, as well as epilepsy.292 Our current adjustment is based on rough calculations of how much malaria morbidity contributes to the total burden of malaria (details in footnote).293
- Short-term anemia effects (+9%). Malaria infection is a risk factor for anemia, and there is evidence that malaria control interventions reduce anemia.294 We account for this effect in our analysis with an adjustment of 9%.295
- Prevention of diseases other than malaria (+2%). ITNs may reduce the burden of other mosquito-borne diseases such as zika virus, dengue, yellow fever and encephalitis. We account for this with a 2% adjustment. This is a rough guess to reflect our understanding that the burden of these diseases is very low compared with the burden of malaria in areas with the highest malaria mortality rates, but we have not reviewed the evidence in detail.
- Prevention of stillbirths (+9%). Our understanding is that malaria in pregnancy increases the risk of stillbirth, although we have not reviewed the evidence for this in depth.
- Investment of income increases (+2.5%). We think that net recipients may see income gains in later life (see above). If this is correct, some recipients might invest a portion of their increased income. We include an adjustment to account for this. In part, this is to achieve consistency with our other cost-effectiveness analyses that estimate economic benefits.
- Costs saved from averted malaria (+20%). By preventing malaria, ITNs may also avert costs that would have been incurred for treatment. These savings include the direct costs of treating malaria (incurred by households or the medical system) as well as indirect costs (e.g., caregivers taking time off work to care for unwell children). We account for these savings with a 20% upward adjustment.296 This adjustment is consistent across all GiveWell’s top charities focused on improving child health.297 We chose to use a consistent figure because our model for estimating the value of costs of illness averted was very similar across these interventions (all around 20%),298 and we thought that explicitly modeling this benefit stream across countries would not be worth the added complexity. For more detail on our reasoning, see this summary.
- Subnational adjustments (+2%). Our analysis uses national-level data on malaria burden for most countries.299 We expect that, in general, net distributions will be targeted towards higher burden areas than average.300 To account for this, we include a 2% upward adjustment.
- Mosquito insecticide resistance in ITN trials (+5%). Our insecticide resistance adjustment301 assumes that the studies in Pryce et al. were conducted in contexts without insecticide resistance and adjusts for the growth in insecticide resistance since that time. However, insecticide resistance may have been present in some of these studies.302 We account for this here with a 5% upward adjustment.303
Negative and offsetting impacts
As of December 2023, we include the following negative adjustments and offsetting impacts in our analysis:
- Marginal funding goes to lower priority areas (-5% to -15%). If there is not enough funding available to fully reach entire populations with ITN distributions, our guess is that some countries will make prioritization decisions to exclude some lower-burden areas. In effect, providing additional funding for ITN distributions allows these lower-burden areas to be covered. This would imply we could be overestimating cost-effectiveness by using malaria burden data at the national level. We account for this with a downward adjustment (5% to 15%, depending on the location)304 . Our estimates are based on a best guess about how each country's government would allocate ITNs if we did not provide additional funding. To determine this, we (a) consider what the government did in past distribution rounds, and (b) have conversations with stakeholders about what's likely to happen in the next round. We use a value of 15% for most countries in our analysis, where we believe National Malaria Programs may target lower-burden areas last.305
-
Rebound effects / decreased immunity development (-4%). Some researchers have argued that ITNs, by protecting children from malaria in the short-term, may reduce opportunities to develop immunity and make them more susceptible to malaria over the long term.306 We account for this risk with a 4% downward adjustment. This adjustment is relatively small, in part because our assessment (based on a shallow review of the evidence) is that the studies we have seen that involve long-term follow-ups on ITN distributions have concluded that reductions in child mortality in the treatment group relative to the control group were sustained for several years after the initial study (details in footnote).307 In 2022, WHO held a technical consultation on the rebound phenomenon,308 but we have not yet reviewed this or considered how it could affect our estimate.
- Differences in mosquito species (-2%). Our insecticide resistance adjustment309 is based on resistance data from specific mosquito species in specific regions. The model assumes that the species represented in the resistance data are the same species that are prevalent in ITN distribution locations. If different species have differing levels of resistance to the insecticides used in ITNs, we may be misestimating cost-effectiveness. We evaluated this assumption and found that there may be differences in the species distributions that underlie our estimates and those that are prevalent in our locations of interest.310 We account for this with a 2% downward adjustment.311
Factors we have excluded
A number of potential benefits and offsetting impacts have been excluded from our model altogether. We exclude these factors either because we are uncertain how to interpret them, we expect their impact to be very small, or they are accounted for in other ways.
- Productivity effects. Averting malaria cases might have benefits for short-term economic productivity among adults.312 We know of two randomized controlled trials investigating the impact of ITNs on economic productivity (Fink and Masiye 2015 and Sedlmayr 2014). We have reviewed Fink and Masiye 2015 closely, and our assessment is that it does not provide strong evidence of productivity effects (details in footnote).313 We have not closely reviewed Sedlmayr 2014 but it appears to find no impact of ITNs on productivity.314 We separately account for some of the mechanisms through which malaria could lead to productivity increases (e.g., people taking less time off work while ill with malaria, or to care for sick children) in our adjustment for costs saved from averted malaria (discussed above).315
-
How might the effectiveness of ITNs vary across settings with different malaria transmission patterns? In a previous version of this report, we discussed the evidence that ITNs may be less effective in areas with malaria transmission patterns unlike those seen in sub-Saharan Africa. This concern is based on a randomized controlled trial conducted in Myanmar which found no effect of an ITN distribution on malaria.316 In short, we do not see this as a major concern for ITN distributions in sub-Saharan Africa, where GiveWell has supported distributions to date.
- Offsetting births. Life-saving interventions like ITN distributions might not increase the number of children alive if parents respond to lower mortality by having fewer children. We explain this concern in more detail in this 2016 blog post. This is not merely an empirical question, but also an ethical one—whether or not you view the program as less valuable if there are offsetting births or not depends on your ethical framework. Empirically, our read of the evidence is that child deaths in places where GiveWell funds ITN campaigns are likely to be only partially offset by additional births. In 2014, GiveWell Senior Advisor David Roodman published a detailed study exploring the evidence linking life-saving interventions and fertility and concluded that in places with high fertility rates (as is currently the case in much of sub-Saharan Africa),317 there is likely less than 0.5 offsetting births per child death.318 Given the ethical uncertainty in how to account for this effect, we do not account for it in our cost per life saved calculations. Stakeholders who have contributed to the moral weights that we use to compare life-saving to income-increasing programs may have taken it into account.
- Fire hazard from nets. ITNs can be flammable and may pose a fire hazard. We have seen evidence from two studies of ITN-related fires resulting in injury and death.319 Given the large number of people protected by ITNs (2.5 billion ITNs were globally distributed between 2004 and 2021),320 we'd expect that it would be visible to government malaria programs, the international global health community, and the media if there were a significant number of injuries and deaths due to ITNs. We have heard little about this concern from those sources.
- Allergic reactions. We have heard anecdotes of ITNs causing minor allergic reactions (e.g., itching skin). We have located no mention of this issue in the Cochrane reviews discussed above and have located very little information on it in general. We did discuss it with program staff during our visit to an ongoing ITN distribution (we were told that this issue affects few people and can be avoided by letting an ITN hang for a few days before use). We think this is a very minor concern.
- Equity concerns. It is possible that ITN distribution may cause conflicts if it is not perceived as fair and equitable. We have seen very little evidence on whether this is an issue. Because the programs we have funded to date (as of 2023) are mass campaigns that aim to reach all households and base the number of nets per household on the number of residents, we would expect this to be a relatively minor concern.
- Using ITNs for fishing in waterside, food-insecure communities. A 2015 New York Times article describes people using ITNs for fishing instead of sleeping under the nets to protect themselves from malaria-carrying mosquitoes. We believe this problem is unlikely to be widespread, and we see it as a much smaller problem than people lacking nets for preventing malaria (details in footnote).321
-
Undermining private markets. It is possible that giving away ITNs for free causes people to systematically expect that they will continue to receive them for free, and thus causes people to be unwilling to pay for them. We do not see this as a major concern (details in footnote).322
- Diverting skilled labor from other activities. ITN distributions require time investment from government officials and NGO partner staff at various stages of implementation. This may result in skilled labor being diverted from other activities (details in footnote).323 We attempt to account for the monetary cost of government officials’ time in our cost per net calculations, but this is an extrapolation from very little data (from one costing study of a campaign in a single district in Malawi in 2012).324
- Increasing development of resistance. Widespread distribution of ITNs is likely to contribute to future development of insecticide resistance. We agree that insecticide resistance is a serious concern and account for our expectation that resistance has increased over time via the insecticide resistance adjustment in our cost-effectiveness analysis. This adjustment does not account for increasing development of resistance in the future. Factors that mitigate our concern about increasing resistance include the development of next generation nets that are less susceptible to resistance and our understanding that most of the malaria community (including WHO) continues to support ITN distributions.325
4.6 Grantee-level adjustments
Our cost-effectiveness analyses also include adjustments relating to the specific organizations we recommend rather than the intervention itself. These reflect aspects of the organization’s delivery of a program that might have an impact on cost-effectiveness. Rather than explicitly model these, we apply them as rough percentage best guesses.
As of December 2023, we estimate that these factors reduce the cost-effectiveness of the ITN campaigns AMF supports by 4%.326 This reduction is fully accounted for by a downward adjustment of -4% to account for the quality of AMF’s monitoring and evaluation.327 This adjustment reflects our best guess at the extent to which methodological aspects of AMF’s monitoring could inflate its estimates of the number of people protected with ITNs.
AMF conducts monitoring surveys after the campaigns it supports to understand whether nets are in good physical condition, retained in households, and used as intended in the months and years after the campaign. See this section of our separate report on AMF for more details. We have some methodological concerns about these surveys, and to account for these, we apply a downward adjustment of -4% to our cost-effectiveness estimate.328
Other grantee-level factors in our analysis that we consider are:
- The risk of wastage (i.e., whether the program might use goods that are out of date, poorly made, left in storage, or otherwise ineffective).
- Our confidence that funds will be used for their intended purpose (i.e., whether our funding will actually be spent on ITNs in a timely manner).
We assign a 0% downward adjustment in each case either because we see the risk as minimal or because we account for this factor elsewhere in our analysis.329 See this section of our cost-effectiveness analysis for more details on our reasoning.
5. How does our funding affect other actors’ spending?
5.1 Summary
Part of our cost-effectiveness analysis involves asking what impact funding a program has on other actors’ spending. Funding for ITNs may lead other organizations or governments to spend more (we refer to this as "leveraging" or “crowding in” funding) or less (we refer to this as "funging," from “fungibility,” or “crowding out”) on nets than they otherwise would.
We include a “leverage and funging” adjustment in our cost-effectiveness analysis to account for this. As of December 2023, our leverage and funging adjustment is -14% to -42%, varying by location (e.g., this adjustment is -32% in Uganda).330 A summary of our calculations is below, using Uganda as an example:
| What we are estimating | Value |
|---|---|
| Grant size (arbitrary value) | $1,000,000 |
| Value of AMF’s spending in Uganda (more) | 0.077 (units of value per $) |
| Total units of value generated by AMF spending | 76,545 |
| Resources spent by other actors per $1m spent by AMF | |
| Ugandan government (more) | ~$47,000 |
| What would happen if we did not fund the program | |
| Nobody would replace AMF’s costs (more) | 60% probability |
| The Global Fund or PMI would have replaced AMF’s costs (more) | 40% probability |
| Estimated value of activities that would be funded by other actors instead of nets | |
| Activities funded by the Ugandan government (more) | 0.005 (units of value per $, ~1.5x as cost-effective as direct cash transfers)331 |
| Activities funded by the Global Fund or PMI (more) | 0.015 (units of value per $, ~4.5x as cost-effective as direct cash transfers)332 |
| Change in value under different scenarios | |
| Nobody would replace AMF’s costs (leverage) | -142 |
| The Global Fund or PMI would replace AMF’s costs (funging) | -24,445 |
| Final adjustments | |
| Adjustment for leverage | -0.19% |
| Adjustment for funging | -32% |
| Total: Adjustment for leverage and funging | -32% |
- Our analysis of how other actors will behave if we do not make a grant are necessarily subjective guesses, as we can only speculate about their future priorities and decisions.
- Our adjustments rely on estimates of the value of other programs that other actors might fund instead of nets. We outline the estimates and our reasoning for them below, but these are rough estimates based on limited information. We have also invested considerably less time into producing these estimates than we have in our main cost-effectiveness analyses, and they should be thought of as rougher guesses.
5.2 Leverage
Leverage refers to GiveWell’s funding causing other actors to contribute more funding to net distributions than they otherwise would. We already account for the main part of this effect in our cost per net calculations (where we exclude in-kind government resources that we think our funding leverages). This means the benefit of these resources is already baked into our main calculations. To account for these resources, we make a small negative adjustment here reflecting that they will not be used for other programs. Our adjustment for this effect reduces our initial cost-effectiveness estimate by a negligible amount (0.19% in Uganda).333
In more detail:
- We think that each $1 million spent by AMF causes the Ugandan government to incur approximately $47,000 of in-kind costs (e.g., staff time) (more above).
- We exclude these costs when we estimate the number of children sleeping under nets and the number of deaths averted in the main part of our cost-effectiveness analysis (more above). This means that the benefit of these resources is already incorporated in our initial impact calculations. We account for these resources by deducting the value of the programs we think they would have been spent on otherwise (see this blog post for more on why we use this approach).
- Our best guess is that if these resources were not used for nets, the Ugandan government would have used them for something ~6% as cost-effective as net campaigns.334 In total, diverting these funds away from other programs “costs” 236 units of value (calculation in footnote, more on units of value here).335
- We think there’s approximately a 60% chance that the additional nets that AMF funds would not be distributed in its absence. This implies that AMF’s funding causes the government to divert its resources away from other programs into net campaigns. For more information on our reasoning, see below.
- Our final leverage adjustment involves multiplying 236 units of value by 60%, and deducting the result (142) from our estimate of the total value generated by AMF’s spending (76,545 units of value).336 This equates to a -0.2% adjustment.337
- Intuitively, the reason this adjustment is small is that (i) we think the other activities the Ugandan government might fund are considerably less cost-effective than net campaigns, so the value lost from diverting these funds away from other activities is relatively small, (ii) only a small share of the total costs of the program (~4%) are borne by the government (more above).
5.3 Funging
Funging refers to AMF’s funding causing other actors to contribute less funding to net campaigns than they otherwise would. As of December 2023, we estimate that this effect reduces cost-effectiveness by ~32% in Uganda.338 We typically update the parameters this estimate is based on for each grant we make. Our reasoning for this estimate was most recently updated for a 2021 grant, for net campaigns to be conducted in 2023 (more here).
Our reasoning is:
- For the 2021 grant, we thought that there was a 40% chance that other malaria funders (the Global Fund or PMI) would replace AMF’s spending on nets in Uganda in AMF’s absence.339 This is a rough guess, based on our understanding of the malaria funding landscape in Uganda. See below for more details on our reasoning.
- If other malaria funders were to replace AMF’s spending in AMF’s absence, this would imply that the true impact of AMF’s spending is to free up other malaria funders’ resources for other activities.340 Our best guess is that the activities other funders might fund instead are approximately ⅕ as cost-effective as nets in Uganda,341 and therefore we would lose 61,112 units of value, relative to our initial estimate of the total value generated by AMF’s spending (76,545 units of value) (calculation in footnote).342
- We thought that there was a 40% chance that other malaria funders would replace AMF’s funding for nets in AMF’s absence. For our final funging adjustment, we therefore multiply 61,112 units of value by 40%, and deduct the result (24,445 units of value) from our estimate of the total value generated by AMF’s spending (76,545 units of value).343 This equates to a -32% adjustment.344
- Intuitively, the reason this adjustment is relatively large is that we think there’s a substantial (40%) chance that the real impact of AMF’s spending on nets in Uganda is simply to free up other malaria funders’ resources for other activities that we think are probably less cost-effective.
5.4 Breakdown of our analysis
This section provides a step-by-step walkthrough of our analysis to account for other actors’ spending (our “leverage and funging” analysis). Our detailed calculations are on this sheet.
Percentage of costs paid by different actors
We estimate the proportion of program costs paid for by different actors. These estimates are based on our cost analysis (discussed above) using cost data from AMF and estimates of in-kind government resources used for ITN campaigns based on a study of one distribution in Malawi in 2012.
What would happen if AMF did not fund nets?
We make guesses about what would happen to other actors’ spending on nets if AMF did not fund the net campaign.346 For Uganda, we most recently estimated these probabilities as part of a 2021 grant (for campaigns taking place in Uganda in 2023). We guessed that if GiveWell had not provided AMF funding for the campaign:347
- There was a 40% chance that the Global Fund or PMI would have replaced the funding (Scenario 2).
- There was a 60% chance that nobody would have replaced AMF’s funding (Scenario 4).
These guesses were based on our analysis of the malaria funding landscape (globally and in Uganda). Some of the points we considered were:
- Globally, malaria funding had been increasing in the years leading up to the grant.
- Between its 2018-20 and 2021-23 grant cycles, the Global Fund's malaria allocation for Uganda increased by a larger percentage than its allocation to ITN campaigns in Uganda.350
- Much of the funding increase went to other malaria programs and health systems strengthening.351 We thought it was possible that the Ugandan government may have chosen to allocate less to these other programs and more to ITN campaigns if AMF had not had a history of supporting campaigns in Uganda.
- The grant also included funding for ITN campaigns in Nigeria and Togo. We guessed that there was a 20% chance that the Global Fund or PMI would have replaced GiveWell’s funding in Nigeria and a 60% chance in Togo. Our reasons for using a value in between these in Uganda included:
- We do not believe Uganda is as underfunded for malaria overall as Nigeria.352
- Between the 2018-20 and 2021-23 grant cycles, the Global Fund's malaria allocation to Togo grew even more than its allocation to Uganda.353 All else equal, we thought this implied a higher chance that other funders would have replaced GiveWell’s funding in Togo than in Uganda.
See this spreadsheet and our grant page for more details on our reasoning.
How valuable are ITN distributions, compared to the activities that other actors might fund instead?
Our leverage and funging adjustments estimate the impact of shifting funding to or from ITN campaigns, relative to other activities that governments and malaria funders might fund instead. This means that we need to estimate the value of these other activities.
To do this, we compare activities in terms of "units of value," an arbitrary unit GiveWell uses to compare the moral value of different types of outcomes (e.g., increased income vs reduced deaths). We benchmark the value of each benefit to a value of 1, which we define as the value of doubling someone’s consumption for one year. See this document for more details on how we think about comparing value across different interventions.
Our analysis of leverage and funging for net campaigns in Uganda involves three specific estimates:
- AMF spending on nets in Uganda (before leverage and funging): 0.077 units of value per $ (more)
- Activities that domestic governments might fund instead of nets: 0.005 units of value per $ (more)
- Activities that the Global Fund might fund instead of nets: 0.015 units of value per $ (more)
Our estimates of the other activities that might be funded instead of nets are based on considerably less work than our main cost-effectiveness analysis, and so we think of them as rougher guesses.
AMF spending on nets in Uganda
We estimate that each $ spent by AMF on net campaigns in Uganda generates 0.077 units of value.354 This figure is the final output generated by our cost-effectiveness analysis, after factoring in all adjustments except leverage and funging.
Activities that domestic governments might fund instead of nets
We estimate that each $ of in-kind resources that the Ugandan government contributes to net campaigns would generate 0.005 units of value if used for other activities.355 This is around 1/15 as valuable.356
In summary, our approach is:
- We estimate that 80% of these resources would be used on health programs, 10% would be used for education programs and 10% would be used on social security programs.357 This is a very rough best guess, for which we have not done any in-depth research.
- Next, we estimate the value of spending in each category (details on our approach in footnote).358
This results in the following estimates:
- Health: 0.0056 units of value per $ spent
- Education: 0.0028 units of value per $ spent
- Social security: 0.0026 units of value per $ spent
- Finally, we take a weighted average of the value of each type of spending, with our guesses about how the spending would be allocated (80% health / 10% education / 10% social security) as the weights. This results in an overall estimate of 0.005 units of value per $ spent.
Activities that the Global Fund might fund instead of nets
We estimate that each $ that the Global Fund spends on other activities rather than net campaigns in Uganda generates 0.015 units of value.359 This is around ⅕ as valuable as our estimate of spending on ITN campaigns.360
Our calculations for this estimate are available in this spreadsheet. In summary, our approach is:
- The Global Fund funds HIV, tuberculosis (TB), and malaria programs. We assume that all funding that the Global Fund could use for net campaigns in Uganda but actually uses for other activities is spent on programs combating these diseases.
- We estimate the value of spending on each type of program (details on our approach in footnote).361
This results in estimates (here) that the Global Fund’s spending on HIV programs is 1.1x as cost-effective as direct cash transfers (GiveWell’s benchmark for comparing the value of different programs), and its spending on TB programs is 3.2x as cost-effective.
- For malaria, we conduct a more detailed analysis, breaking down Global Fund spending by seven types of malaria programs that it may fund instead of ITN campaigns in Uganda (varying in cost-effectiveness from 0.5 to 13.6x, depending on the program).362
- Finally, we estimate the overall value of the Global Fund’s spending on other activities. We calculate a weighted average of each of the programs discussed above in proportion to how likely we think it is to spend reallocated funding on that activity. These estimates are based on 2017-2019 data on how funding reallocated within the Global Fund portfolio in that period was used.363 We do not have permission to publish this data, so our full calculations are available on a separate spreadsheet (only available to GiveWell staff). This weighted average produces our overall estimate of 0.015 units of value per $ spent (equivalent to 4.6x as cost-effective as direct cash transfers).
6. Additional perspectives beyond our cost-effectiveness model
6.1 Summary
In theory, our cost-effectiveness analysis intends to capture the total impact of a program per dollar spent. But we recognize that our cost-effectiveness calculations are not able to capture every factor that could make a program more or less impactful. Focusing only on our cost-effectiveness model may mean we’re missing things that are difficult to quantify.
As a result, we think it’s helpful to look at other perspectives and types of evidence that may not be captured in our bottom line cost-effectiveness number. Some additional questions we have considered are:
- Is there evidence that large-scale net campaigns lead to reductions in malaria?
- Do experts and practitioners see ITNs as an effective investment?
- Would other ways of funding nets be more effective?
- Is GiveWell’s funding of nets crowding out other net funders over the long term?
- Is it intuitively plausible that nets are cost-effective?
- How does our cost-effectiveness model compare to others?
- Do nets have unintended negative consequences?
- How accurate was our analysis of nets in hindsight?
- Will nets remain impactful in the future?
We see asking these questions as a type of “cluster thinking,” or considering a program from multiple perspectives. The more additional perspectives we’ve considered, in general the more confident we are in our funding recommendations.
Overall, the additional perspectives we’ve considered give us some additional confidence that ITNs are a good investment. In particular, we find it encouraging that mass net distribution appears to have widespread support in the global health community.
But we have spent considerably less time and effort engaging with these questions than we have on our main cost-effectiveness model. Major gaps in our analysis include:
- We haven’t deeply investigated ways we could fund nets other than mass campaigns (e.g., through routine distribution or "market shaping" interventions). (More)
- Over the long term, GiveWell’s funding for nets could create an expectation of future funding. This could mean we crowd out funding from other funders (i.e., displace funding that would have gone to nets into investments that may be less cost-effective). We have found it challenging to find evidence either way on whether this is happening. (More)
- We have not deeply engaged with critics of mass net distribution. This is in part because our impression is that nets are widely supported in the malaria community. However, we have not specifically sought out critics of nets. It’s possible that this means we’re missing something important. (More)
We’re hoping to engage with these questions in more detail in the future.
6.2 Is there evidence that large-scale net campaigns lead to reductions in malaria?
Why is this important? We generally rely on randomized controlled trials (RCTs) for evidence about the causal impact of a program. But all else equal, it strengthens our confidence if there’s evidence that large-scale programs show similar impact to studies conducted in experimental conditions. We think this issue is particularly applicable to ITNs, since the RCTs we rely on for our main analysis were mostly conducted in the 1990s (more above). Changes since that time (e.g., the spread of insecticide resistance) could make the RCT findings less relevant to campaigns funded today. Delivery of large-scale programs may also not meet the same quality standards as studies conducted in experimental conditions.
How we’ve accounted for this
- In 2012-2013, we investigated whether it is possible to isolate the impact of ITNs on malaria via trends in malaria burden after ITNs were scaled up. Our discussion is on a separate page. At the time, we concluded that it was difficult to link changes in the burden of malaria to particular malaria control measures. Because the evidence was limited and incomplete, we decided not to factor this into our cost-effectiveness analysis.
- We still believe that estimates of malaria mortality are very uncertain.364 Some estimates (as in the case of the Global Burden of Disease Project) may already incorporate the expected impact of ITNs on mortality into their estimates.365 This means it is challenging to use these as evidence to evaluate the impact of different malaria interventions on mortality or malaria trends.
- Although we haven’t revisited this question in depth since 2013, we conducted some initial (unpublished) analysis in 2023 of six studies of large-scale malaria programs. Five of these looked specifically at net campaigns.366 All of these studies attributed declines in malaria to large-scale net programs. Our initial review also suggested the reduction was relatively consistent with the conclusions of our cost-effectiveness analysis, although we did not investigate this in detail.
- Using similar reasoning, we also conducted a rough (unpublished) analysis of how increases in net coverage over time in countries where GiveWell has funded ITNs367 compare to child mortality trends in those countries. Using data on the proportion of people sleeping under an ITN from the Malaria Atlas Project,368 our best guess that nets reduce malaria mortality by approximately 50% (more above), and estimates of the share of child mortality attributable to malaria, we estimated that 17% to 60% (depending on the country) of the fall in child mortality between 2010 and 2019 could be attributed to ITNs.369 These findings were higher than we were expecting. But we’re hesitant to put any weight on our analysis because so many other factors could affect child mortality trends other than ITN access (e.g., other malaria interventions, changing economic conditions, etc.) and we’re uncertain what a plausible range for nets’ contribution to child mortality would be.
- Because we thought that there were likely to be challenges in using these studies to demonstrate causation, we have not published this analysis or prioritized further work on this question.
6.3 Do experts and practitioners see ITNs as an effective investment?
Why is this important? We’re more confident in programs which have wide support from experts in malaria-endemic countries and the global health community more widely.
How we’ve accounted for this
- We have not investigated this question systematically, e.g., by analyzing or conducting polls of global health experts or national malaria program representatives.
- Through our work on nets, we have built up an impression over time that mass net campaigns are widely supported by the global health community. Evidence feeding into this impression includes:
- WHO recommends insecticide-treated net distribution as one of only two main recommended strategies for malaria vector control.370
- Nets have been by far the most widely used malaria prevention tool in recent decades. WHO estimates that 2.5 billion ITNs were supplied globally between 2004 and 2021, and the proportion of people in sub-Saharan Africa with access to at least one ITN rose from 5% to 68% between 2000 and 2021. This compares with 2.4% of the population in sub-Saharan Africa being protected with indoor residual spraying (IRS) in 2021.371 We interpret this as evidence of widespread support for nets.
- We have heard feedback from conversations with malaria stakeholders over time that net distributions are typically among the highest priority malaria prevention programs for national malaria programs.372
-
In 2023, we received feedback on our ITN research from David McGuire, Director of Access and Market Shaping at the Innovative Vector Control Consortium (IVCC), highlighting some concerns about ITN distribution. While emphasizing that ITNs are a good investment overall,373 he told us:
- External donors have been focused on ITNs as the primary intervention for vector control, and continue to shift resources away from other effective interventions such as Indoor Residual Spraying (IRS), despite evidence that removal of IRS often leads to increased malaria incidence.374
- Funders of ITNs have historically relied too little on advice from malaria experts in Africa when making decisions about how to best tailor vector control strategies using a broader mix of targeted interventions based on local context.375
- ITNs are an excellent tool to control malaria in high-transmission settings, but no country has used ITNs as a key intervention in the final stage of successful elimination.376
- ITNs generate large amounts of plastic waste.377
- Many people do not like using ITNs, meaning it is challenging to get mass uptake. This can be for various reasons including discomfort on hot nights, and standardized net designs not being adapted for people’s preferences.378
With the exception of the last of these (where we make explicit assumptions about net usage), we haven’t considered these criticisms of ITNs in detail, or thought through how they should affect our funding recommendations.
While we are relatively confident that net campaigns command overall support in the global health community, we may be missing downsides by not investigating this question more systematically. We may prioritize engaging with critics of net campaigns, and digging more into the questions raised by David McGuire, in the future.
6.4 Would other ways of funding nets be effective?
Why is this important? To date, GiveWell has only funded ITNs through mass campaigns. The large majority of our funding has also gone through one organization (AMF). It might be that we’re missing other effective ways of funding nets.
How we’ve accounted for this
- In addition to AMF, GiveWell has previously funded one other organization, Malaria Consortium, to fund net campaigns in two states in Nigeria in 2021-2022 (more here). Malaria Consortium used a different model to AMF, in which it handled both purchasing and distributing the nets. We are planning to continue exploring multiple different grantees for net campaigns in the future.
- We have not deeply investigated other ways of promoting nets other than mass campaigns (e.g., funding for “continuous distribution” of nets at touchpoints people have with the state or healthcare system, like antenatal appointments, or “market shaping” interventions to reduce net price or increase supply). We are actively considering whether these could be effective options to fund ITNs in the future.
6.5 Is GiveWell’s funding of nets crowding out other net funders over the long term?
Why is this important? Our adjustments for the impact of GiveWell funding on other actors’ spending mainly consider the probability that another actor would fund nets if we didn’t in the short term. They do not fully account for the long-term impact. For example, it might be that GiveWell’s funding could create an expectation of future funding, and displace other actors’ funding that would have gone on nets into other programs.
How we’ve accounted for this
- We have seen some evidence that GiveWell’s ITN funding has crowded out funding from other sources. For example, we have seen cases of national malaria programs subtracting the amount they expect to receive for nets from AMF from their Global Fund funding applications. This evidence is discussed here.
- We’re unsure how widespread this is, and how much it should affect our grantmaking. We attempt to incorporate this into our analysis of GiveWell’s impact on other actors’ spending here (+10% to +20% increase in the likelihood that other funders would replace GiveWell’s spending in our absence), but this is a very uncertain guess.
- We aim to mitigate this effect in our conversations with national malaria programs and other funders, by emphasizing that, to the extent possible, our goal is for the funding we direct to nets to add to the total pool of funding available, rather than to replace funding that would otherwise have been in that pool.
6.6 Is it intuitively plausible that nets are cost-effective?
Why is this important? In general, we are more confident in our funding recommendations if we can easily explain the intuitive case for why a program is cost-effective. Thinking through the intuition behind a program can help us reveal where we might have made mistakes.
How we’ve accounted for this
- Overall, we think that the intuitive case for ITNs (set out in detail in the report summary) is strong.
- In their most simple terms, GiveWell’s cost-effective analyses can be boiled down to the following components: (a) burden (does the intervention tackle a big problem), (b) impact (does the intervention have a significant impact on the problem), (c) cost (is the intervention cheap to deliver), and (d) impact of our funding the program on intervention uptake (does our funding lead to more people receiving the intervention). We believe that ITNs look like an effective investment on all these criteria, since:
- Malaria is a major cause of child deaths in sub-Saharan Africa (more above).
- ITNs are effective at reducing deaths due to malaria, based on randomized controlled trials, opinions from experts, and a clear mechanism (more above).
- Each ITN is cheap to deliver (roughly $4 to $6 per net, more above).
- If we didn’t fund mass net distribution, many fewer people would receive nets (more above).
6.7 How does our cost-effectiveness model compare to others?
Why is this important? GiveWell’s analysis is only one attempt to model the cost-effectiveness of different global health programs. We would find it concerning if other analyses found that ITNs are significantly less cost-effective than we currently estimate.
How we’ve accounted for this
- We’re aware of at least two other publicly available tools that we could check our model against. These are the Imperial College London Malaria Intervention Tool (MINT) (which allows users to analyze the most cost-effective option for deploying ITNs and IRS to avert the highest amount of malaria)379 , and the Lives Saved Tool (LiST), a tool to understand the impact of different maternal and child health interventions on mortality.380 There may be others we have not seen.
- To date (December 2023), we haven’t checked our cost-effectiveness analysis against either tool.
6.8 Do nets have unintended negative consequences?
Why is this important? When trying to estimate the total impact of distributing ITNs, we need to offset the benefits with any negative impacts.
How we’ve accounted for this
- We explicitly account for one negative impact from distributing ITNs—the possibility that they delay the development of immunity to malaria and make children more susceptible in the long term—with a -4% adjustment elsewhere in our analysis.
- We consider a range of other possible downsides and negative impacts in this section of the report. We exclude these factors from our cost-effectiveness analysis because we’re uncertain how to interpret them, we expect their impact to be very small, or they are accounted for in other ways.
- Overall, we think the negative impacts of distributing ITNs are relatively small, in comparison to the benefits, and in the same range as other programs we see as very effective. We’re reasonably confident about this conclusion, although we may not have considered all the possible downsides (see above) and we have not investigated some of these issues recently.
6.9 How accurate was our analysis of nets in hindsight?
Why is this important? Our cost-effectiveness analyses are “forward-looking.” They aim to project the future impact of funding a program at the time we make a grant decision. We would be concerned if backwards checks of our analysis found significant problems we hadn’t considered at the time we made our decisions, or were overly optimistic in general.
How we’ve accounted for this
- In general, GiveWell has paid less attention to backwards checks to understand how accurate our predictions were, and more attention to making our forward projections as accurate as possible. This is a weakness in our approach and something we aim to improve in the future.
- As part of our research on ITNs, we have conducted backward-looking analysis to inform our best guess of various parts of our cost-effectiveness analysis (details in footnote).381
- We have not yet conducted a backwards-looking analysis of our ITN cost-effectiveness as a whole, to understand how accurate our predictions were. We are hoping to prioritize this in the future. There are also a number of other types of backwards-looking analysis we have considered doing, but not yet prioritized (details in footnote).382
6.10 Will nets remain impactful in the future?
Why is this important? Our cost-effectiveness analysis aims to model the impact of our funding at the time we make a grant, but this may reflect program delivery several years in the future. We could be making mistakes if we don’t anticipate likely changes in the malaria landscape.
How we’ve accounted for this
- We have generally paid attention to making our analysis accurate at the time we make a grant. We want to improve this aspect of our work in the future and think in more detail about possible future changes, although this is inherently uncertain.
- One particular uncertainty in our analysis is the impact of malaria vaccines. As of December 2023, WHO has recommended two malaria vaccines.383 We expect a significant amount of future malaria funding to go towards the vaccine rollout. Our best guess is that this will make nets less cost-effective (because the overall burden of malaria will be lower), but we have not analyzed this systematically.
- We’re also unsure about future developments in insecticide resistance. It’s possible that resistance will develop to chlorfenapyr in the same way it has for pyrethroids, but we’re unsure over what timescale this could take place. This could also be offset by the developments of new types of nets in the future, as happened with PBO and chlorfenapyr nets. We haven’t investigated this question in detail.
-
We have also seen reports of other changes to mosquitoes and malaria epidemiology that could affect our analysis in the future:
- The spread of the anopheles stephensi mosquito from Asia to sub-Saharan Africa. Our understanding is that these mosquitoes may transmit malaria more easily in urban areas.384
- Mosquitoes becoming more likely to bite during the day, when people don't usually use nets.385
- An increase in malaria burden among school-age children.386
We have not investigated these questions in detail, or understood how they could affect our work on ITNs. We plan to monitor them closely in the future.
7. Previous ITN grants
Sources
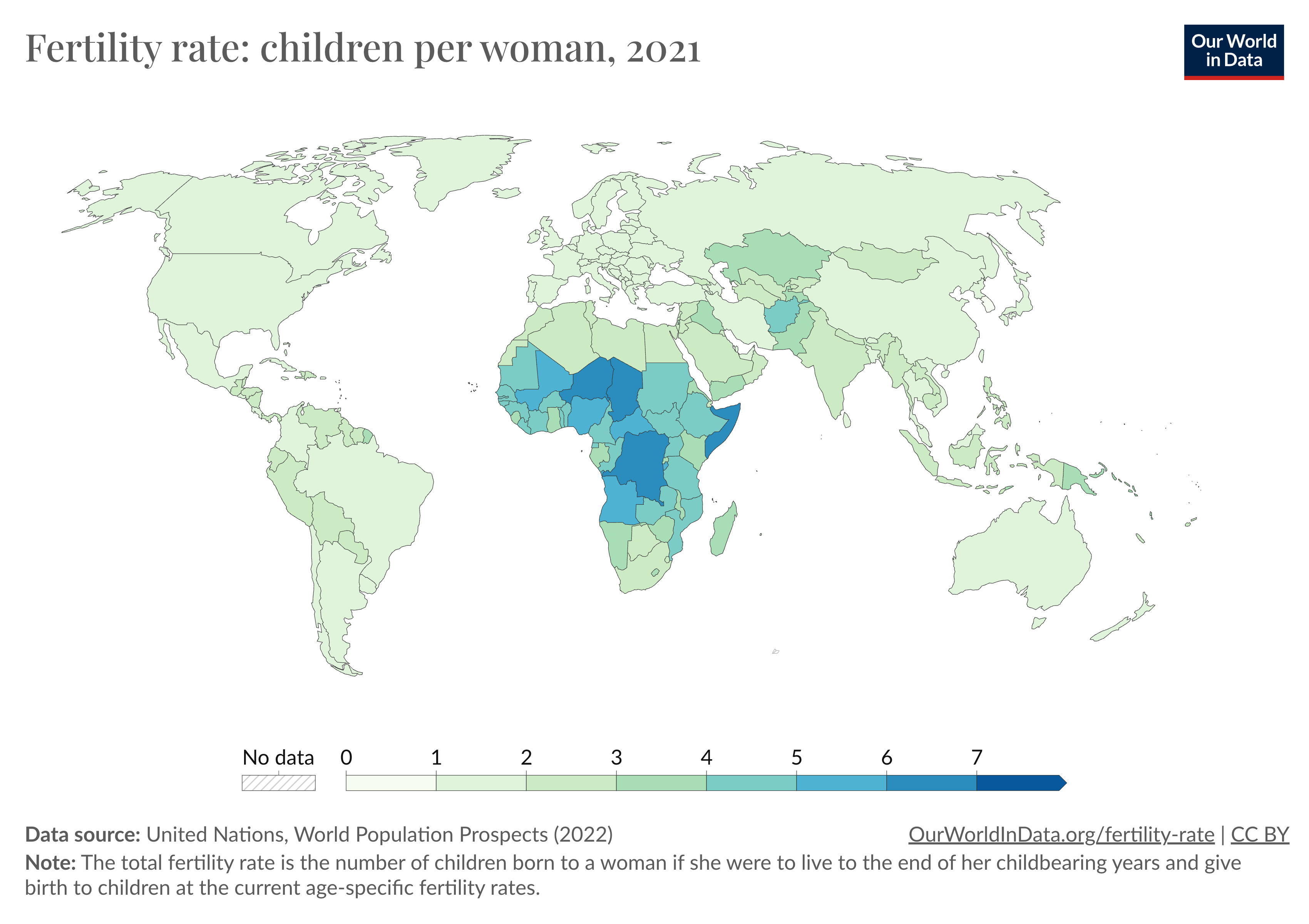{kind=link}
- 1
"Malaria is a life-threatening disease spread to humans by some types of mosquitoes. It is mostly found in tropical countries. It is preventable and curable…The infection is caused by a parasite and does not spread from person to person…There are 5 Plasmodium parasite species that cause malaria in humans and 2 of these species – P. falciparum and P. vivax – pose the greatest threat. P. falciparum is the deadliest malaria parasite and the most prevalent on the African continent. P. vivax is the dominant malaria parasite in most countries outside of sub-Saharan Africa." World Health Organization (WHO), "Malaria," 2023
- 2
"The most common early symptoms of malaria are fever, headache and chills… Some types of malaria can cause severe illness and death." WHO, "Malaria," 2023
- 3
"Infants, children under 5 years, pregnant women, travellers and people with HIV or AIDS are at higher risk." WHO, "Malaria," 2023
- 4
"Globally, malaria deaths reduced steadily over the period 2000–2019, from 897 000 in 2000 to 577 000 in 2015 and to 568 000 in 2019. In 2020, malaria deaths increased by 10% compared with 2019, to an estimated 625 000. Estimated deaths declined slightly in 2021 to 619 000." WHO, World Malaria Report 2022, p. xxi.
- 5
- 6
"The WHO African Region continues to carry a disproportionately high share of the global malaria burden. In 2021 the Region was home to about 94% of malaria cases (233 million) and 95% (580 000) of malaria deaths." WHO, "Malaria," 2023
- 7
The WHO defines an insecticide-treated net as: “A mosquito net that repels, disables or kills mosquitoes that come into contact with the insecticide on the netting material. Insecticide treated nets (ITNs) include those that require treatment and retreatment (often referred to as conventional nets) and those are “long-lasting” (see definition of long-lasting insecticidal net).” WHO, WHO Malaria Terminology 2021 Update, p. 19.
- 8
WHO definition: “A factory-treated mosquito net made of material into which insecticide is incorporated or bound around the fibres. The net must retain its effective biological activity for at least 20 WHO standard washes under laboratory conditions and 3 years of recommended use under field conditions.” WHO, WHO Malaria Terminology 2021 Update, p. 17.
- 9
- “Interventions that are recommended for large-scale deployment in terms of malaria vector control are those that have proven protective efficacy to reduce or prevent infection and/or disease in humans and are broadly applicable for populations at risk of malaria in most epidemiological and ecological settings. Vector control interventions applicable for all populations at risk of malaria in most epidemiological and ecological settings are: i) deployment of insecticide-treated nets (ITNs) that are prequalified by WHO, and ii) indoor residual spraying (IRS) with a product prequalified by WHO.” WHO, WHO guidelines for malaria, 16 October 2023, p. 41.
- Indoor Residual Spraying is defined by the WHO as: “Operational procedure and strategy for malaria vector control involving spraying interior surfaces of dwellings with a residual insecticide to kill or repel endophilic mosquitoes.” WHO, WHO Malaria Terminology 2021 Update, p. 25.
- WHO defines vector control as: “Measures of any kind against malaria-transmitting mosquitoes, intended to limit their ability to transmit the disease. Note: Ideally, malaria vector control results in reduction of malaria transmission rates, by reducing the vectorial capacity, to a point at which transmission is interrupted.” WHO, WHO Malaria Terminology 2021 Update, p. 14.
- 10
“To achieve and maintain optimal ITN coverage, countries should apply a combination of mass free net distribution through campaigns and continuous distribution through multiple channels, in particular through ANC clinics and the EPI. Mass campaigns are the only proven cost-effective way to rapidly achieve high and equitable coverage. Complementary continuous distribution channels are also required because coverage gaps can start to appear almost immediately postcampaign due to net deterioration, loss of nets, and population growth.
Mass campaigns should distribute one ITN for every two persons at risk of malaria. However, for procurement purposes, the calculation to determine the number of ITNs required needs to be adjusted at the population level, since many households have an odd number of members. Therefore, a ratio of one ITN for every 1.8 persons in the target population should be used to estimate ITN requirements, unless data to inform a different quantification ratio are available.” WHO, WHO guidelines for malaria, 16 October 2023, p. 62. - 11
- “Pyrethroid-PBO ITNs (2022)
Pyrethroid-PBO ITNs instead of pyrethroid-only LLINs can be deployed for the prevention and control of malaria in children and adults in areas with ongoing malaria transmission where the principal malaria vector(s) exhibit pyrethroid resistance.
Remark: The conditionality of this recommendation is largely driven by the current higher unit cost of pyrethroid-PBO ITNs compared to pyrethroid-only LLINs and therefore the uncertainty of their cost-effectiveness.” WHO, WHO guidelines for malaria, 16 October 2023, p. 6.- Our understanding is that WHO first issued an interim recommendation for PBO nets in 2017. “In 2017, WHO started to recommend a new type of ITN that combines pyrethroids with piperonyl-butoxide (PBO), a chemical that enhances the potency of pyrethroids against resistant mosquitoes.” WHO, "WHO publishes recommendations on two new types of insecticide-treated nets," 2023
- 12
“New recommendations, published today in the WHO Guidelines for malaria, cover 2 new classes of dual ingredient ITNs with different modes of action:
Pyrethroid-chlorfenapyr nets combine a pyrethroid and a pyrrole insecticide to enhance the killing effect of the net…
...New recommendation on pyrethroid-chlorfenapyr nets vs pyrethroid-only nets
WHO is issuing a strong recommendation for the deployment of pyrethroid-chlorfenapyr ITNs vs pyrethroid-only nets to prevent malaria in adults and children in areas where mosquitoes have become resistant to pyrethroids.” WHO, "WHO publishes recommendations on two new types of insecticide-treated nets," 2023
- 13
“New recommendation on pyrethroid-pyriproxyfen nets vs pyrethroid-only nets
WHO is issuing a conditional recommendation for the deployment of pyrethroid-pyriproxyfen nets instead of pyrethroid-only nets to prevent malaria in adults and children in areas with pyrethroid resistance.
The conditionality of the recommendation is based on the GDG’s concerns around the poor cost-effectiveness of pyrethroid-pyriproxyfen nets compared to pyrethroid-only nets; the extra resources currently required to purchase these ITNs may have a negative impact on coverage and equity.”
Note that, unlike chlorfenapyr nets, WHO conditionally recommended against using pyriproxyfen nets over pyrethroid-PBO nets.
“New recommendation on pyrethroid-pyriproxyfen nets vs pyrethroid-PBO nets
WHO has issued a conditional recommendation against the deployment of pyrethroid-pyriproxyfen nets instead of pyrethroid-PBO nets.
The conditionality of the recommendation is based on the GDG’s judgement that the balance of effects favours pyrethroid-PBO nets over pyrethroid-pyriproxyfen nets and that, based on current cost and efficacy data, pyrethroid-PBO nets are more cost-effective.” WHO, "WHO publishes recommendations on two new types of insecticide-treated nets," 2023 - 14
- PBO nets: “Data from experimental hut trials suggest that the PBO component of pyrethroid‐PBO nets is lost after repeated washing, as enhanced mortality caused by the synergist nets is not maintained after 20 washes. As yet, no trials on the durability of pyrethroid‐PBO nets under operational conditions have been published, although monitoring is under way.” Gleave et al. 2021, p. 20.
- Chlorfenapyr nets and pyriproxyfen nets: “Based on results up to 24 months post-ITN distribution from these trials, the WHO has recently released a strong recommendation for pyrethroid-chlorfenapyr ITNs over pyrethroid-only nets and a conditional recommendation for pyrethroid-pyriproxyfen nets over pyrethroid-only ITNs for malaria control in areas where vectors have become resistant to pyrethroids. Following the WHO recommendation, an increased uptake of pyrethroid-chlorfenapyr and pyrethroid-pyriproxyfen nets is expected in the coming years. However, to be considered long-lasting, new ITNs need to be evaluated for their physical and insecticidal durability over 3 years of operational use.” Ngufor et al. 2023, p. 2.
- 15
Note that many of GiveWell’s research materials on ITNs were originally developed before next-generation nets were in wide use, and so use the generic term “LLIN” to refer to all nets that don’t require retreatment with insecticide.
- 16
The WHO recommends that endemic countries should use a combination of both approaches:
“To achieve and maintain optimal ITN coverage, countries should apply mass free net distribution through campaigns, combined with other locally appropriate delivery mechanisms such as continuous distribution using antenatal care (ANC) clinics and the Expanded Programme on Immunization (EPI).” WHO, WHO guidelines for malaria, 16 October 2023, p. 8. - 17
“Mass campaigns should distribute 1 ITN for every 2 persons at risk of malaria. However, for procurement purposes, the calculation to determine the number of ITNs required needs to be adjusted at the population level, since many households have an odd number of members. Therefore a ratio of 1 ITN for every 1.8 persons in the target population should be used to estimate ITN requirements, unless data to inform a different quantification ratio are available. In places where the most recent population census is more than five years old, countries can consider including a buffer (e.g. adding 10% after the 1.8 ratio has been applied) or using data from previous ITN campaigns to justify an alternative buffer amount. Campaigns should also normally be repeated every three years, unless available empirical evidence justifies the use of a longer or shorter interval between campaigns.” WHO, Guidelines for Malaria Vector Control, 2019, pp. 39-40.
- 18
“To achieve and maintain universal ITN coverage, countries should apply a combination of mass free net distribution through campaigns and continuous distribution through multiple channels, in particular through antenatal care (ANC) clinics and the Expanded Programme on Immunization (EPI). Mass campaigns are the only proven cost-effective way to rapidly achieve high and equitable coverage. Complementary continuous distribution channels are also required because coverage gaps can start to appear almost immediately post-campaign due to net deterioration, loss of nets, and population growth…
…Continuous distribution through ANC and EPI channels should remain functional before, during and after mass distribution campaigns. School based distribution should be discontinued in campaign years to avoid over-supply of ITNs. In areas where school-based distributions are operating at scale and achieve high coverage, these distributions may even be sufficient to replace mass distribution campaigns.” WHO, Guidelines for Malaria Vector Control, 2019, pp. 39-40. - 19
We focus on universal distribution of ITNs (aiming to protect everyone in a community) rather than targeted distribution (targeting ITNs at populations at high risk, like young children). We discuss the relative benefits of each approach in a previous version of this report. We do not discuss it in detail here because the national malaria programs we have seen conduct universal distributions (following the WHO recommendation) and we have only supported universal distributions to date.
- 20
We are unsure about the strength of the case for investing in continuous distribution if an area is already being reached by a mass campaign and that campaign is achieving high coverage. However, we have not yet investigated the cost-effectiveness of continuous ITN distribution in depth.
- 21
Our understanding of the key role of NMPs in delivering ITN campaigns is based on numerous conversations with our grantees, other malaria stakeholders and national governments over multiple years.
NMP names and acronyms vary by country. Names we have seen include the “National Malaria Control Program” (NMCP) or “National Malaria Elimination Programs” (NMEP). In Francophone countries, NMPs are commonly known as the “Programme National de Lutte Contre Le Paludisme” (National Program for the Fight Against Malaria) or PNLP. We provide some illustrative examples below:- Nigeria: “The National Malaria Elimination Programme (NMEP) in Nigeria is the body responsible for formulating and facilitating policy and guidelines, coordinate the activities of partners and stakeholders on malaria control activities, provide technical support to states malaria programs, LGAs and stakeholders; mobilize resources, monitor and evaluate progress and outcomes in malaria elimination efforts across the country." National Malaria Elimination Programme (Nigeria), "About NMEP"
- Senegal: “La mission du PNLP est de mettre en œuvre la Politique de lutte contre le paludisme au Sénégal.” (The mission of the PNLP is to put in place policies to fight against malaria in Senegal). Ministére de la Santé et de L'action Sociale (Senegal), "Programme National de Lutte contre le Paludisme (PNLP)"
- Uganda: “The mission of the Ministry of Health’s National Malaria Control Programme is to provide quality assured services for malaria prevention and treatment to all people in Uganda.” Republic of Uganda Ministry of Health, "National Malaria Control Program"
- 22
These locations are: Chad, Democratic Republic of Congo (DRC), Guinea, Nigeria (Global Fund states), Nigeria (PMI states), South Sudan, Togo, and Uganda.
Note: We separate Nigeria into two groups of states depending on which external funder supports malaria programs in those states. This is because these funders have historically restricted their funding to specific designated states (more here) and we expect the specific funder to have a bearing on cost-effectiveness (e.g. via our adjustment for other actors’ spending, discussed here).
- 23
This range excludes Chad and South Sudan. We exclude these countries from the ranges in this report because GiveWell has not previously supported net campaigns in either location, and so we think the other locations in our analysis are a better reflection of the cost-effectiveness of GiveWell grants to net campaigns.
- Chad: We added Chad to our analysis when previously considering making a grant to AMF to support a net campaign in Chad, but declined to make the grant because we estimated the campaign would be under our cost-effectiveness bar.
- South Sudan: We previously made a grant to AMF to support net campaigns in South Sudan, contingent on AMF providing GiveWell with information we could use to update our cost-effectiveness analysis. In fact, AMF signed an agreement with the National Malaria Program in South Sudan before sharing the agreed information, and we later concluded that the campaign was under our cost-effectiveness bar. As a result, AMF agreed to save the grant funding for another opportunity and funded the campaign in South Sudan using its own funds. More on this grant page.
- 24
We used the following process:
- Three GiveWell staff members familiar with our research on ITNs gave confidence intervals for the parameters in the Simple CEA sheet of our cost-effectiveness analysis. The intervals were for AMF’s program in Uganda (the example program we discuss in this report). These intervals address the following question: “For each parameter, provide an upper and lower bound for the range of values that you think has a 50% probability of containing the true value (i.e., a 25% probability the true value is lower than the range, and a 25% probability the true value is higher).”
- Where we felt that it was difficult to form an intuitive judgment about a parameter (e.g., because it comprised several separate parameters), we gave intervals for each individual parameter.
- For example, our estimates of the cost per child reached with a net are calculated from four component parameters: (i) cost per net distributed, (ii) proportion of distributed nets used, (iii) number of people sleeping under each net, (iv) proportion of people sleeping under nets aged <5. We gave confidence intervals for each of these parameters.
- A fourth GiveWell staff member reviewed the intervals given by the first three staff members and decided upon a final interval for each parameter, using their subjective judgment.
- We applied the intervals used for Uganda to other countries as follows:
- We first calculated both the relative differences and absolute differences between our best guesses and our 25th and 75th percentile values for each parameter. For example, if our best guess value for a parameter was 50% with 25th and 75th percentile values of 25% and 75%, then the relative differences would be -50% and +50%, and the absolute differences would be -25 percentage points and +25 percentage points.
- We assigned confidence intervals to each country that matched the widths of our confidence intervals for Uganda, putting some weight on the relative difference between the confidence interval bounds and the best guess and some weight on the absolute difference. The higher our best guess value for a parameter in a country was compared to our best guess for Uganda, the more weight we put on the absolute difference between the confidence interval bounds and our best guess. The purpose of this method was to avoid assigning extremely wide confidence intervals to parameters in countries where our best guess was much higher than our best guess for Uganda.
- Finally, we used monte carlo simulations to transform the confidence intervals for individual parameters into an aggregated confidence interval for each parameter. These are the intervals that appear in the summary of this page, and the Uganda columns in the Sensitivity Analysis sheet of our cost-effectiveness analysis.
- Three GiveWell staff members familiar with our research on ITNs gave confidence intervals for the parameters in the Simple CEA sheet of our cost-effectiveness analysis. The intervals were for AMF’s program in Uganda (the example program we discuss in this report). These intervals address the following question: “For each parameter, provide an upper and lower bound for the range of values that you think has a 50% probability of containing the true value (i.e., a 25% probability the true value is lower than the range, and a 25% probability the true value is higher).”
- 25
$1 million is an arbitrary amount that we use to quantify the benefits of the program in the rest of our analysis. See this row in our cost-effectiveness analysis.
- 26
We estimate that it costs roughly $18 to $26 for one additional child under age five to sleep under a net. $1 million / $18 = ~56,000 and $1 million / $26 = ~38,000. See these rows in our cost-effectiveness analysis for the cost per child under five reached and the number of children under five reached per $1 million by country. This range includes DRC, Guinea, Nigeria (Global Fund and PMI states), Togo, and Uganda only (excluding Chad and South Sudan) for the reasons discussed in this section.
- 27
See this row in our cost-effectiveness analysis for the years of effective net coverage by country. This range includes DRC, Guinea, Nigeria (Global Fund and PMI states), Togo, and Uganda only (excluding Chad and South Sudan) for the reasons discussed in this section.
- 28
- See this row in our cost-effectiveness analysis for the full estimated cost per net distributed in each country.
- We estimate the majority of these costs are direct costs. Excluding in-kind government contributions like staff time, we estimate that it costs approximately $3.50 to $5.50 to distribute one net in an AMF-supported program. See this row in our cost-effectiveness analysis.
- 29
AMF, comment on a draft of GiveWell’s report on AMF, December 12, 2023.
- 30
GiveWell, analysis of AMF’s cost per net, March 2023 (unpublished).
- 31
Note that this includes AMF’s research and organizational costs. GiveWell, analysis of AMF’s cost per net, March 2023 (unpublished).
- 32
GiveWell, analysis of AMF’s cost per net, March 2023 (unpublished).
- 33
See this row of our cost-effectiveness analysis. We use this figure to denominate the number of nets distributed (e.g., $1 million / $4.25 = 235,489 in Uganda).
- 34
Because we do not have permission from the Global Fund to publish its costs, for the purposes of our cost-effectiveness analysis, we present AMF as covering all non-governmental costs for each campaign (96% of total costs in most locations, with in-kind government contributions accounting for the rest). See this row in our cost-effectiveness analysis.
This does not affect our bottom line, because:- Unlike the in-kind government contributions, we think that AMF’s funding does not increase the Global Fund’s spending on a given campaign. Instead, we think that AMF’s funding changes the way the Global Fund’s spending is allocated between net purchase and distribution costs (more in our separate review of AMF). We refer to the Global Fund’s costs as “upstream” of AMF for this reason.
- This implies, for example, that if AMF spends an additional $1 million on a campaign in Uganda we think the impact of that spending is for an extra 235,489 nets to be delivered ($1 million / $4.25). This is true even though we think in practice AMF pays for all the purchase costs for a larger number of nets, and only a small portion of the non-net costs.
- 35
These estimates use GiveWell’s analysis of data collected by AMF and its partners on the number of ITNs distributed in each campaign. See this section of GiveWell’s separate report on AMF’s program for more details on this data.
AMF notes that these data reflect the proportion of nets not distributed in the intended campaign, but most nets are retained for future (e.g. through “continuous distribution” of nets in health clinics) and so will eventually be used. AMF’s data indicates that less than 1% of purchased nets (0.5% as of December 2023) do not reach recipients as intended once this is taken into account. AMF, comment on a draft of GiveWell’s report on AMF, November 14, 2023 (unpublished) and email to GiveWell, December 19, 2023 (unpublished).
We haven’t investigated this in detail, and we don’t have a strong understanding of how AMF’s process for redistributing nets that weren’t distributed in the campaign works or how effective it is at reaching people with nets.
- 36
AMF refers to these surveys as its “post-distribution monitoring” (PDM) surveys. See our Against Malaria Foundation review for our discussion of the PDMs.
- 37
See cell B34 on the "Summary" sheet of our 2018 cost per net analysis here. The value of these contributions may have varied by country and over time, and our analysis does not account for this. However, the precise estimate we use does not make a large difference to our bottom line (partly because estimates are a small proportion of total costs) and so we have not prioritized further work on it.
- 38
We would expect this estimate to vary between campaigns according to the non-net costs of the campaign, not the purchase price of each ITN. We therefore adjust the $0.13 estimate in proportion to the total estimate of non-net costs for each location.
- 39
- AMF’s partners (either national health agencies or in-country non-profit organizations) gather data at the distribution stage of each campaign on the number of nets distributed to households. AMF has shared this data with GiveWell for previous campaigns.
- Our main uncertainty about this data is that we have very little visibility into how it was collected. We have not investigated in detail the methodology used to collect the data or possible sources of bias. Additionally, our understanding is that the distribution data is not audited. This reduces our confidence in the data and limits our ability to check its accuracy.
- See this section of our review of AMF for more detail.
- 40
We also use an (unpublished) costing study conducted by another GiveWell grantee, Malaria Consortium, for an ITN campaign in Ondo state, Nigeria in 2021 (more detail on the campaign and costing study are available on this page). We do not place much weight on data from this study for locations outside Nigeria because we would expect the cost of distributions to vary significantly in different operating environments.
- 41
Definitions of net usage vary. We define usage as the proportion of distributed nets which are hung. Separately, we estimate that the number of people sleeping under each net is approximately two per net each night (discussed below).
- 42
- Our analysis focuses exclusively on the analysis of ITNs compared to no nets, as this is the comparison we model in our cost-effectiveness analysis.
- “Our updated search identified three new trials. A total of 23 trials met the inclusion criteria, enrolling more than 275,793 adults and children. The included studies were conducted between 1987 and 2001.
ITN versus no nets
Insecticide‐treated nets reduce child mortality from all causes by 17% compared to no nets (rate ratio 0.83, 95% CI 0.77 to 0.89; 5 trials, 200,833 participants, high‐certainty evidence). This corresponds to a saving of 5.6 lives (95% CI 3.6 to 7.6) each year for every 1000 children protected with ITNs. Insecticide‐treated nets also reduce the incidence of uncomplicated episodes of Plasmodium falciparum malaria by almost a half (rate ratio 0.55, 95% CI 0.48 to 0.64; 5 trials, 35,551 participants, high‐certainty evidence) and probably reduce the incidence of uncomplicated episodes of Plasmodium vivax malaria (risk ratio (RR) 0.61, 95% CI 0.48 to 0.77; 2 trials, 10,967 participants, moderate‐certainty evidence).
Insecticide‐treated nets were also shown to reduce the prevalence of P falciparum malaria by 17% compared to no nets (RR 0.83, 95% CI 0.71 to 0.98; 6 trials, 18,809 participants, high‐certainty evidence) but may have little or no effect on the prevalence of P vivax malaria (RR 1.00, 95% CI 0.75 to 1.34; 2 trials, 10,967 participants, low‐certainty evidence). A 44% reduction in the incidence of severe malaria episodes was seen in the ITN group (rate ratio 0.56, 95% CI 0.38 to 0.82; 2 trials, 31,173 participants, high‐certainty evidence), as well as an increase in mean haemoglobin (expressed as mean packed cell volume) compared to the no‐net group (mean difference 1.29, 95% CI 0.42 to 2.16; 5 trials, 11,489 participants, high‐certainty evidence).
ITN versus untreated nets
Insecticide‐treated nets probably reduce child mortality from all causes by a third compared to untreated nets (rate ratio 0.67, 95% CI 0.36 to 1.23; 2 trials, 25,389 participants, moderate‐certainty evidence). This corresponds to a saving of 3.5 lives (95% CI ‐2.4 to 6.8) each year for every 1000 children protected with ITNs. Insecticide‐treated nets also reduce the incidence of uncomplicated P falciparum malaria episodes (rate ratio 0.58, 95% CI 0.44 to 0.78; 5 trials, 2036 participants, high‐certainty evidence) and may also reduce the incidence of uncomplicated P vixax malaria episodes (rate ratio 0.73, 95% CI 0.51 to 1.05; 3 trials, 1535 participants, low‐certainty evidence).”
Pryce et al. 2018, p. 2. - 43
See our analysis in this spreadsheet. The five studies analyzed in this spreadsheet are those included in Analysis 1.2 in Pryce et al., which estimates the impact of ITNs on uncomplicated episodes of P. falciparum malaria vs no nets. See Pryce et al. 2018, Analysis 1.2, p. 56. See this section of the report for a discussion of why we focus on these five studies in particular.
- 44
The weight assigned to each of the three trials (Nevill et al. 1996, Sexton et al. 1990 and Sochantha et al. 2006) was 25%, 20% and 12% respectively. 25 + 20 + 12 = ~57%. See our analysis here.
- 45
Note that two of these studies (Nevill et al. 1996 and Sexton et al. 1990) measured usage through household visits, whereas Sochantha et al. 2006 estimated usage via self-reported survey data. We include an adjustment for self-report bias in our estimate of usage in Sochantha et al. 2006, See our calculations for further details.
- 46
Our understanding is based on the wording used in each study.
"During the dry, hot season (January-March) 65% of intervention children were found to be using the net correctly and during the wet, cooler months of highest malaria transmission observed bednet use was 77% among the target childhood population." Nevill et al. 1996, p. 142.
“…unannounced visits on 2 occasions at 2100 and 2200 hours demonstrated that only 70% and 73% of the families who were in bed at that hour were using their bed-nets, respectively.” Sexton et al. 1990, p. 14."Reported ITN use suggested a high coverage in intervention villages, with the proportion sleeping under a net the previous night increasing from 12% at baseline to 87% at the second cross-sectional survey. By contrast, reported coverage in control villages went up from 12% at baseline to only 14%, indicating little contamination between trial arms." Sochantha et al. 2006, p. 1170.
- 47
For example, in a situation where net coverage is high and households have more nets than they need, the proportion of ITNs used might be low and the proportion of people sleeping under nets might be high.
- 48
70% x (100% - 10%) = 63%. See this row in our cost-effectiveness analysis.
- 49
“The bulk of data in this review describe impact under ideal trial conditions (efficacy) rather than impact under large-scale programme conditions (effectiveness). While the difference between efficacy and effectiveness is likely to be small for certain medical interventions (such as vaccination or surgery), it can potentially be large for preventive interventions such as ITNs.
Some of the consequences of moving from a scientific trial towards a large-scale programme is illustrated by the results of the two mortality trials carried out in The Gambia. The first trial was carried out under well-controlled implementation conditions, with a high coverage rate in the target population (Gambia (Alonso)). Unfortunately it was not randomized and hence not included in the present analysis. The second one was the evaluation of a national impregnation programme carried out by primary health care personnel and which faced some operational problems...and a lower coverage rate (around 60%) of the target population (Gambia (D’Alessandro)).The difference of impact between the two studies is important: the first trial achieved a total reduction in mortality of 42%, while the protective efficacy in the second trial was 23%." Lengeler 2004a
- 50
See our summary of Against Malaria’s post-distribution monitoring surveys in this spreadsheet.
- 51
The 2010 World Malaria Report finds three countries in sub-Saharan Africa with greater than 100% apparent usage (this could be a function of more than two people covered by each ITN in some cases, combined with possible over-reporting of usage in surveys), two countries with very low apparent usage (Swaziland, 0%, and Nigeria, 40%), and seven countries with apparent usage ranging from 69% to 85%.
The 2012 World Malaria Report uses a slightly different methodology and finds slightly higher usage rates. In 17 sub-Saharan African countries that conducted surveys from 2009-2011, the median net usage rate was 91%, with an interquartile range of 82% to 98% usage.
We base our estimate of over-reporting on one study included in Pryce et al. where actual usage (as assessed by spot visits to homes) was 70% to 73% while reported usage was 85% (See this row in our supplementary analysis). If we assume an equal amount of over-reporting in the national surveys as in the small-scale study, and apply this adjustment to the 2010 World Malaria Report data, actual net usage rates would range from 57% to 73%. If this adjustment were applied to the 2012 World Malaria Report data, the interquartile range for net usage rates would be 68% to 84%. WHO, World Malaria Report 2010, Table 4.2, p. 19; WHO, World Malaria Report 2012, Annex 5, p. 212.
- 52
“Seasonal variation in the proportion of the population using an insecticide-treated net (ITN) is well documented and is widely believed to be dependent on mosquito abundance and heat, driven by rainfall and temperature. However, seasonal variation in ITN use has not been quantified controlling for ITN access. Demographic and Health Survey and Malaria Indicator Survey datasets, their georeferenced data, and public rainfall and climate layers were pooled for 21 countries. Nine rainfall typologies were developed from rainfall patterns in Köppen climate zones. For each typology, the odds of ITN use among individuals with access to an ITN within their households (“ITN use given access”) were estimated for each month of the year, controlling for region, wealth quintile, residence, year, temperature, and malaria parasitemia level. Seasonality of ITN use given access was observed over all nine rainfall typologies and was most pronounced in arid climates and less pronounced where rainfall was relatively constant throughout the year. Peak ITN use occurred 1–3 months after peak rainfall and corresponded with peak malaria incidence and average malaria transmission season. The observed lags between peak rainfall and peak ITN use given access suggest that net use is triggered by mosquito density. In equatorial areas, ITN use is likely to be high year-round, given the presence of mosquitoes and an associated year-round perceived malaria risk. These results can be used to inform behavior change interventions to improve ITN use in specific times of the year and to inform geospatial models of the impact of ITNs on transmission.”
Koenker et al. 2019, p. 371. - 53
We are aware of research summaries on this topic, such as Koenker et al. 2023, but have not yet reviewed this literature in detail.
- 54
There is evidence of this from one of the studies included in the Pryce et al. meta-analysis, which found self-reported usage rates of 85% compared to 70% to 73% when assessed by spot visits to homes. "Eighty five per cent of those with bed-nets claimed they had used the nets every night during the preceding 7 days; however, unannounced visits on 2 occasions at 2100 and 2200 hours demonstrated that only 70% and 73% of the families who were in bed at that hour were using their bed-nets, respectively. The remainder stated that they had "forgotten" to use their nets or that it was too hot to use them." Sexton et al. 1990, p. 14. See GiveWell, Summary of ITN RCTs, “1. Studies from Pryce et al. 2018” sheet.
- 55
- This is approximately the ratio recommended by the WHO. The WHO recommends that ITN campaigns distribute one ITN for every two people at risk of malaria (at a population level, the recommended ratio is one ITN per 1.8 people to account for some households having an odd number of residents).
“Mass campaigns should distribute 1 ITN for every 2 persons at risk of malaria. However, for procurement purposes, the calculation to determine the number of ITNs required needs to be adjusted at the population level, since many households have an odd number of members. Therefore a ratio of 1 ITN for every 1.8 persons in the target population should be used to estimate ITN requirements, unless data to inform a different quantification ratio are available." WHO, Guidelines for Malaria Vector Control, 2019, p. 39.
- See this spreadsheet for our calculations. The overall average across countries is 1.94, and the range is from 1.72 (Togo) to 2.15 (DRC). We have not seen survey results from distributions in Chad, Nigeria, or South Sudan, so we rely on our "overall" people per net estimate for these countries.
- 56
"Insecticidal activity (bioefficacy) is the degree of knock-down, mortality or inhibition of blood-feeding induced in susceptible mosquitoes, as determined by st
See this section of our review of Against Malaria Foundation for further details on these surveys. - 57
- Our analysis is based on data from eight countries from surveys conducted between 2014 and 2020. The countries included in the dataset are DRC, Ghana, Guinea, Malawi, Papua New Guinea, Togo, Uganda, and Zambia. See this sheet for a breakdown of surveys by timepoint and country.
- There are some discrepancies between the data we rely on shared by AMF for this analysis and data we were able to pull from another source of AMF data for the same campaigns. In most cases, these discrepancies are small (~0 to 1%), but for some specific campaigns the differences are much larger (e.g., Uganda in 2020). See this section of our analysis for a comparison between the two data sources. Because these discrepancies are largely small and we do not have an easy way to assess which source is more reliable, we think the chance that this could bias our estimates substantially is small. We rely on the unadjusted estimates in this spreadsheet in our analysis.
- 58
We have not reviewed any data to directly measure or validate our adjustment. Instead, we arrive at the 6% figure as follows:
- Intuitively, we would assume some social desirability bias (more people report sleeping under nets than actually sleep under them). This is likely to be partly mitigated because the outcome is only measured for nets already found hanging by data collectors (cutting out the possibility of false reports from people who don't hang their nets at all). Our starting point for the analysis was that the adjustment required to account for social desirability bias was likely to be in the -3% to -15% range.
- We identify a point in this range by evaluating the data against five criteria which could indicate bias. For example, one of the criteria we selected is the average number of people per household in each country surveyed. We would expect more than two people sleeping under each net to be more likely in larger households. The data suggests that this is broadly true across countries. We interpret this as indicating low bias for this criterion.
- We then weight each of the five criteria according to our level of confidence in our assessment. Finally, we take a weighted average of our confidence-weighted bias assessments across all five criteria and round this to the nearest percentage point for simplicity and to reflect our uncertainty.
- See this section of our "Number of people covered per net" analysis for these calculations.
Note that this is a rough adjustment with a high level of uncertainty. Although none of the criteria we assessed the data against indicated a high risk of bias, some criteria were only loosely connected to the data we were attempting to validate (the average number of people sleeping under a net). We think it is plausible that a different source of data might update us to a different conclusion.
- 59
See this row in our cost-effectiveness analysis. This range includes DRC, Guinea, Nigeria (Global Fund and PMI states), Togo, and Uganda only (excluding Chad and South Sudan) for the reasons discussed in this section.
- 60
The population estimates we use are drawn from the Institute for Health Metrics and Evaluation (IHME)'s 2019 Global Burden of Disease (GBD) model. We adjust separately in our analysis for the possibility that older children and adults use nets at lower rates than young children (more).
- 61
See here in our cost-effectiveness analysis for the effective coverage years provided per net by country.
- 62
The WHO recommends that ITN campaigns take place at three-year intervals. “Campaigns should also normally be repeated every three years, 40 unless available empirical evidence justifies the use of a longer or shorter interval between campaigns.” WHO, Guidelines for Malaria Vector Control, 2019, pp. 39-40.
- 63
Note: one weakness in our analysis is that this comparison is based on data from analysis 1.1 in the meta-analysis (from five studies that measured all-cause mortality) and not analysis 1.2 (based on a separate set of five studies that measured malaria incidence, with one study overlapping). This is a concern because we use the reduction in malaria incidence from the meta-analysis as the main input in our cost-effectiveness analysis. See this section for more details.
- 64
Note: a more detailed discussion of net durability is available on a separate page (last updated in 2020, and some aspects are out of date).
- 65
WHO definition: “A factory-treated mosquito net made of material into which insecticide is incorporated or bound around the fibres. The net must retain its effective biological activity for at least 20 WHO standard washes under laboratory conditions and 3 years of recommended use under field conditions.” WHO, WHO Malaria Terminology 2021 Update, p. 17.
- 66
Three years is the distribution cycle recommended by the WHO. “Mass campaigns should distribute 1 ITN for every 2 persons at risk of malaria. However, for procurement purposes, the calculation to determine the number of ITNs required needs to be adjusted at the population level, since many households have an odd number of members. Therefore a ratio of 1 ITN for every 1.8 persons in the target population should be used to estimate ITN requirements, unless data to inform a different quantification ratio are available. In places where the most recent population census is more than five years old, countries can consider including a buffer (e.g. adding 10% after the 1.8 ratio has been applied) or using data from previous ITN campaigns to justify an alternative buffer amount. Campaigns should also normally be repeated every three years, 40 unless available empirical evidence justifies the use of a longer or shorter interval between campaigns.” WHO, Guidelines for Malaria Vector Control, 2019, pp. 39-40.
- 67
Note: President’s Malaria Initiative monitoring guidelines recommend a fourth outcome, insecticidal activity (i.e., a net’s efficacy at killing or knocking down mosquitoes). We do not focus on insecticidal activity in our main analysis because:
- Sufficient insecticidal activity for our reference net (the PermaNet 2.0) is implicitly baked into our model because it has undergone Phase III testing. This means that it met WHO's requirements for this factor in 3-year field tests.
- We used insecticide content over insecticidal activity in our comparison between ITNs and the nets used in the original studies of the impact of nets on mortality (see this section) out of convenience, because this is the comparison data available (in Kilian et al. 2011).
We factor insecticidal activity into our -15% adjustment for generic LLINs being less durable than the PermaNet 2.0. This is the main factor driving generic nets being less durable (see our calculations here).
"Insecticidal activity (bioefficacy) is the degree of knock-down, mortality or inhibition of blood-feeding induced in susceptible mosquitoes, as determined by standard WHO test procedures and criteria (i.e. cone bioassay, tunnel test) (1). Insecticidal activity is associated with the type and content or availability of insecticide. The insecticide content is expressed as g/kg or mg/m2 of the LN and is determined by the method outlined in WHO specifications for LNs. This information is of value in interpreting data on bioefficacy. Insecticidal activity can be assessed as a function of length of use." WHO, Guidelines for monitoring the durability of long-lasting insecticidal mosquito nets under operational conditions, 2011, p. 4.
- 68
- In 2011, WHO established field durability monitoring guidelines for LLINs. The President's Malaria Initiative (PMI) also maintains LLIN field durability monitoring advice for practitioners and a database of field durability sites. Under current guidelines, a full battery of LLIN durability monitoring tracks these four outcomes:
“LLIN monitoring measures the effect of normal daily use on four outcomes: 1. Attrition (survivorship), as measured by the loss of nets from households, 2. Physical durability, as measured by the number and size of holes in the net, 3. Insecticide effectiveness, as measured directly but imprecisely by bioassay, and 4. Insecticide content analysis, as measured accurately by chromatography.” USAID, LLIN durability monitoring guidelines, 2019, p. 1.
- "The following definitions, descriptions and indicators are proposed for the elements of durability: Survivorship is the proportion of distributed nets still available for use as intended in the households to which they were given after a defined period, e.g. 1, 2, 3 or more years.
Attrition (opposite of survivorship) is the proportion of nets no longer in use as intended after a defined period after their distribution to the households. Attrition can be categorized by the main reasons why a net is no longer used, namely decay (e.g. destroyed, so torn and worn out that it is considered useless for protection against mosquitoes), absence (e.g. stolen, given away, moved) or used for other purposes.
Physical or fabric integrity reflects the number, location and size of holes in each net. When possible, the assessment can also be categorized by type of hole (burn, tear, seam failure, nibbled or chewed by animals). The physical or fabric integrity of the surviving nets can be assessed as a function of length of use, until deterioration leads to the net being discarded or used for another purpose.
Insecticidal activity (bioefficacy) is the degree of knock-down, mortality or inhibition of blood-feeding induced in susceptible mosquitoes, as determined by standard WHO test procedures and criteria (i.e. cone bioassay, tunnel test) (1). Insecticidal activity is associated with the type and content or availability of insecticide. The insecticide content is expressed as g/kg or mg/m2 of the LN and is determined by the method outlined in WHO specifications for LNs. This information is of value in interpreting data on bioefficacy. Insecticidal activity can be assessed as a function of length of use."
WHO, Guidelines for monitoring the durability of long-lasting insecticidal mosquito nets under operational conditions, 2011. - 69
“Attrition (opposite of survivorship) is the proportion of nets no longer in use as intended after a defined period after their distribution to the households. Attrition can be categorized by the main reasons why a net is no longer used, namely decay (e.g. destroyed, so torn and worn out that it is considered useless for protection against mosquitoes), absence (e.g. stolen, given away, moved) or used for other purposes.” WHO, Guidelines for monitoring the durability of long-lasting insecticidal mosquito nets under operational conditions, 2011, pp. 3-4.
- 70
”The solution to the problem is to use pHI cut-offs that distinguish the following categories:
- LLIN in “good” condition where there is no reduction of efficacy compared to an undamaged net
- LLIN in “acceptable” condition in the sense that their effectiveness is somewhat reduced but still provide significantly more protection than no net at all.
- LLIN “torn” where its protective efficacy for the user is in serious doubt and the net should be replaced as soon as possible.
WHO, Vector Control Technical Expert Group Report to MPAC September 2013, p. 7. Also see p. 8, Table 1.
- 71
- “Insecticide content is the amount of active ingredient per gram of the LN as determined by chemical assay.” WHO, Guidelines for monitoring the durability of long-lasting insecticidal mosquito nets under operational conditions, 2011, p. 14.
- This is a lower priority measure, in part because there is evidence that insecticidal efficacy is poorly correlated with insecticide content. "The measurement of insecticidal content is a supplementary tool for the monitoring of insecticidal activity that may be done on the same cohort of nets sampled for bioassays. Content testing should not be done independently of bioassays. Determination of insecticidal content can be used to confirm the bioassays and estimate insecticide retention rates across different settings and in different LLIN products. However, measurement of insecticidal content requires highly specialized capacity that is likely limited or absent in nearly all PMI countries. Therefore, this must be done either at CDC or at a WHO collaborating center where the cost of analysis is approximately $150 - $350 per sample. Furthermore, in some cases there is a poor correlation between insecticidal content and insecticidal activity, particularly for some LLINs made of polyethylene with insecticide directly incorporated into the fiber. We do not generally recommend carrying out content testing for nets types which incorporate insecticide in solution in the net fiber." USAID, LLIN durability monitoring guidelines, 2019, p. 3.
- 72
We chose the PermaNet 2.0 to serve as a reference net for the following reasons:
- Relevance. One of our grantees for LLIN distribution campaigns, Against Malaria Foundation, has purchased significant quantities of PermaNet 2.0s in the past. See this spreadsheet.
- Data availability. There appears to be a particularly large amount of field monitoring data available for the PermaNet 2.0. Studies are available from several different countries, and multiple studies have long follow-up duration up to 36 months.
- Tractability. Focusing on one key brand of net as a starting point for our model was easier and clearer to execute than other possible sub-divisions of the literature.
- 73
These studies are summarized on this sheet of our model estimating LLIN durability.
- 74
Results are not available for every time point for every study, so each point-in-time estimate is generally based on fewer than 11 results.
- 75
Note: for studies that do not provide data after 24 months, we project results to 36 months based on durability trends between 24 and 36 months in studies which capture data during the whole 36 month period. See this section of our model estimating LLIN durability.
- 76
See our discussion of these nets in the section above.
- 77
The five studies we rely on for the durability comparison measured the impact of ITNs on all-cause mortality, and are listed here. These are different from five different studies measuring the impact of ITNs on malaria cases (listed here). One study, Nevill et al. 1996, overlapped and measured both outcomes.
This is a concern because we use the reduction in malaria cases from the second group of studies as the main input in our cost-effectiveness analysis to model the impact of nets on mortality (more here). Our durability calculations estimate the length of time that a net provides protection at a level equivalent to the protection in these studies, so any discrepancies in net durability between the two sets of studies in the meta-analysis could impact our bottom line.
The reason for this is that we conducted the analysis for our durability analysis when using an older version of our cost-effectiveness analysis, which primarily relied on the all-cause mortality data. Our best guess based on some initial (unpublished) analysis is that updating our model to incorporate data from the studies which measured incidence will not substantially change our bottom line. This is because some of the factors informing our analysis are present in both sets of studies (although the amount of data available is limited). These factors include shorter duration compared to the lifespan of contemporary LLIN distributions and activities to train participants on net care and use in some studies.
- 78
I.e., the number of nets available for use was the same at the end of the studies as at the beginning.
- 79
Note that we do not count ITNs which are given away and used by other people at risk of malaria as attrition for the purposes of this adjustment. Our analysis is based on rough best guesses about what proportion of ITNs are likely to be given away and used over the course of a three-year cycle. We guess that 90% of nets lost in year one are given away, 50% in year two, and 0% in year three. Of the nets given away, we roughly guess that 50% are used. See this section of our analysis for our estimates.
- 80
- We focus on Phillips-Howard et al. 2003 because it carries the majority of the statistical weight for the estimate of child mortality reduction in the mortality meta-analysis we use. Phillips-Howard et al. 2003 is given 66% weight in Pryce et al. 2018. See p. 55, Analysis 1.1.
- Of the 1,488 ITNs issued to the households we sampled, we found 1,372, or 92%, still in place. The percentage of ITNs present in houses that were in use was 73.5% in 1997 and 67.5% in 1998, but this difference was not statistically significant (P = 0.10)." Alaii et al. 2003 (companion to Phillips-Howard et al. 2003 RCT).
- 81
Phillips-Howard et al. 2003 also provided additional nets in the second year to cover immigrants and newborns, amounting to a ~25% addition over the nets originally distributed (+4,600 nets in addition to about 17,000 initially distributed). The source is somewhat unclear if the 8% attrition figure takes into account the additional nets or not, but we believe that it does not (it cites the initial number of nets distributed as the denominator on the survival calculation), which means it's likely that there were actually more total nets present in the community in year 2 than in year 1, although these these nets did not directly replace lost nets. "Upon ITN distribution in November and December 1996, participants were shown how to hang ITNs over either beds or floor mats, and were provided with twine and nails if needed. By the beginning of 1997, more than 17,000 permethrin-treated dark green bed nets (Siamdutch Mosquito Netting Co., Bangkok, Thailand) had been distributed in the 40 of 79 villages randomized to receive ITNs in Asembo. Our aim was to cover all previously counted and measured sleeping places (beds or mats) with an ITN of appropriate size. During 1998, an additional 4,600 ITNs were distributed for new immigrants and newborns." Alaii et al. 2003 (companion to Phillips-Howard et al. 2003 RCT)
- 82
See this section of our analysis for our calculations.
- 83
- See this sheet in our summary of Pryce et al. Note that Smithuis et al. 2013 lasted only one year. However, because it accounts for only 0.1% of the meta-analysis weight for this outcome, we exclude it from our analysis.
- Information on meta-analysis weights for Pryce is taken from Pryce et al. 2018, p. 55 (Analysis 1.1).
- 84
“Mass campaigns should distribute 1 ITN for every 2 persons at risk of malaria. However, for procurement purposes, the calculation to determine the number of ITNs required needs to be adjusted at the population level, since many households have an odd number of members. Therefore a ratio of 1 ITN for every 1.8 persons in the target population should be used to estimate ITN requirements, unless data to inform a different quantification ratio are available. In places where the most recent population census is more than five years old, countries can consider including a buffer (e.g. adding 10% after the 1.8 ratio has been applied) or using data from previous ITN campaigns to justify an alternative buffer amount. Campaigns should also normally be repeated every three years, 40 unless available empirical evidence justifies the use of a longer or shorter interval between campaigns.” WHO, Guidelines for Malaria Vector Control, 2019, pp. 39-40.
- 85
- Phillips-Howard et al. 2003 provided subjects with intensive training on net care and use. Researchers provided subjects with extensive training on net use and care, quarterly monitoring visits, and materials for net repair at each monitoring point. Another trial, Nevill et al.1996, also reported extensive training and support for net recipients.
- "The ITN project, described in detail elsewhere, incorporated extensive educational activities, including community wide meetings in every village, informal discussions with traditional birth attendants associated with the project, participatory educational theater, an art competition for a calendar design involving schoolchildren that attracted hundreds of entries, and distribution of information sheets in Luo. Messages stressed through all media were 1) take ill children to health clinics promptly, 2) sleep under ITNs all year round every night and tuck in ITNs to keep mosquitoes from entering, 3) correct and consistent ITN use can reduce illness and death in young children, 4) wash ITNs only just before insecticide retreatment, and 5) keep ITNs in good condition by sewing up holes." Alaii et al. 2003, pp. 137-138 (companion to Phillips-Howard et al. 2003 RCT).
- "Bed nets were pre-impregnated with 0.5 g of permethrin/m2 of netting and were re-treated to that target dose every 6–9 months. At each retreatment exercise, net and sewing materials were provided to residents whose ITNs were in need of repair. The ITNs were distributed to residents of the 39 control villages in the first quarter of 1999." Alaii et al. 2003, p. 138 (companion to Phillips-Howard et al. 2003 RCT).
- "Bednets were distributed between June and July 1993 to each intervention household and issued according to the 'bed' registers of each house. Distribution was accompanied by pre-tested demonstrations of correct hanging and care of nets by trained field staff. Education in bednet use was continued the following day by government public health technicians who reviewed net hanging and held discussion meetings with small groups of mothers. Posters and school-based bednet plays and interactive learning sessions continued to be used throughout the trial (Marsh et al. in press). Local bednet committees were formed through the existing primary health care system to identify, resolve or report subsequent bednet issues, losses and difficulties within their communities." Nevill et al. 1996, p. 142.
- 86
See this sheet in our durability model for this comparison.
- 87
- See this sheet in our durability model for this calculation. Rather than collate data on insecticide decay from PermaNet 2.0 monitoring studies, this analysis is based on one study which directly compares insecticide content in LLINs compared to conventional ITNs over a 42 month period (Kilian et al. 2011). Kilian et al. finds that the insecticide content of conventional ITNs decayed considerably faster than for LLINs. We use this data and an assumption that conventional ITNs are retreated every six months to estimate the average level of insecticide for each type of net over the relevant time period (24 months for the ITNs in Pryce, 36 months for LLINs).
- "The loss rate was...approximately 20% per year irrespective of the differing initial doses and deltamethrin being used in the other LLIN brands...In contrast, the median alpha-cypermethrin concentration for the conventional ITN [without retreatment] decreased by 69% after 12 months to a median of 7.5 mg/m2 and by 93% after two years with 1.6 mg/m2." Kilian et al. 2011, p. 7.
- 88
Note: This is an average figure over a three-year period. In practice, we estimate that the protection provided in year 1 is high (0.98 equivalent coverage-years) and falls substantially in year 2 (0.77 coverage-years) and year 3 (0.52 coverage-years).
- 89
There are three phases for full product qualification for a "reference" (innovator) LLIN with respect to insecticidal protection. Phase I: laboratory tests of regeneration time, wash resistance index, and active ingredient content, Phase II: hut trials that serve as small-scale field tests to validate Phase I results and Phase III: a full 3-year field evaluation.
Not all LLIN products approved for use by WHO have the same level of evidence backing. Products are broadly divided into reference class LLINs (which have undergone at least one long-term field trial of protective effectiveness) and generic LLINs (which perform similarly to reference class nets in short-term lab tests) (WHO, Determination of equivalence for public health pesticides and pesticide products, 2016, p. 28, Annex 3). To obtain "Equivalence" product certification for a generic LLIN, the product must show identical chemical and physical properties/performance to a reference class LLIN, based only on results of Phase I laboratory testing.
“Currently, equivalent LLINs must demonstrate they have identical chemical and physical properties and release characteristics as the reference (“comparator”) nets. The chemical and physical properties are defined within WHO specifications. These include description of the LLIN, active ingredient (identity, content), wash resistance index, physical properties (mesh, dimensional stability, bursting strength, weight of netting), flammability and storage stability. Release characteristics are defined in Phase I laboratory testing and include regeneration time and wash resistance index. These must be identical to the reference LLIN for equivalency.” See WHO, Determination of equivalence for public health pesticides and pesticide products, 2016, p. 23.
- 90
See our discussion above of different kinds of next-generation net.
- 91
See our calculations here. Note that we rounded our calculated value (17.1%) to the nearest multiple of five to reflect our uncertainty about this input. The underlying studies are Randriamaherijaona, Raharinjatovo, and Boyer 2017, Ahogni et al. 2020(a), Rahaivondrafahitra et al. 2017, and Ketoh et al. 2018.
- 92
Note that some PBO nets are also "generic" (i.e., they have received product prequalification from the WHO, but have not undergone Phase III field testing). We do not apply the -15% generic durability discount to these nets. This is because our analysis is based on weighting different nets’ durability by the proportion of those nets purchased by Against Malaria Foundation (AMF). At the point of analysis, a very high proportion of the PBO nets purchased by AMF were non-generic ("reference class"). An uncertainty in our analysis is that we have not revisited the purchase volume data since 2020, and have not checked if AMF is buying a higher proportion of generic PBOs than in previous years.
- 93
See this row of our accompanying spreadsheet.
- 94
PMI, Durability Monitoring of LLINs in Democratic Republic of Congo, Final report after 36 months follow-up, 2019. Our analysis of the PMI data is available in this sheet.
- 95
Our reasoning for thinking this for each location:
- DRC: "The benefits of being able to commit now to funding nets that will be distributed in DRC in 2022 and 2023 are significant. First, it allows our co-funding partner, the Global Fund, not to scale back its allocation of funding in the first two years of the three year funding cycle. Without confirmation of our funding, reprogramming would be necessary, including scaling back of interventions and delayed distributions. This would be required to spread funds evenly and avoid a significant lack of funds for the final year of the funding cycle. Any resulting delays to distributions mean that households have to wait longer than three years to receive new nets. In the third year, nets wear out and so delays extend the period during which households are less well protected which can lead to malaria resurging." AMF, "AMF agrees to fund a further 16.4 million nets for distribution in DRC in 2023," 2021.
- Nigeria: AMF told us that it expected the impact of additional funding for distributions in states supported by PMI would be to reduce the amount of time between distributions from four years to three years. See this page.
- South Sudan: our understanding is that the Global Fund is the only major external funding source for malaria prevention in South Sudan but hasn't funded net campaigns in all of the country's ten states during any given three-year grant cycle. As a result, net campaigns have been occurring on a rolling basis at the state level, often delayed past the three-year interval that most countries aim to achieve. See this grant page for further details.
- 96
We use the term "coverage" synonymously with the term "protection" used earlier in this report. We think “protection” is a more intuitive term, but have opted to use the term "coverage" in this section to maintain consistency with the language used in our calculations and supplementary spreadsheets.
- 97
See this row in our cost-effectiveness analysis.
- 98
For example, our analysis suggests the deterioration rate was ~50% in year 3. We assume this increases to 67% in year 4 and 80% in year 5. See this section of our calculations.
- 99
Note: AM disputes that this is the impact of its funding in the longer term. AMF believes that when taking a longer term (over several funding cycles) and nationwide view of the situation, the second situation equates to the first, i.e. AMF funding increases the number of people who receive nets. AMF, comment on a draft of GiveWell’s report on AMF, November 13th, 2023.
- 100
0.98 effective years of coverage in year one, 0.77 years in year two, and 0.52 years in year three. See this section in our cost-effectiveness analysis.
- 101
Our approach (calculations on this sheet):
- First, we estimate the proportion of nets which are surviving and in serviceable condition during and at the end of years 1 - 3 based on the durability data we have reviewed (discussed above). We estimate 85% of nets will survive and be serviceable at the end of year 1, 61% at the end of year 2 and 30% at the end of year 3. The estimates during each year are 92%, 71% and 45% respectively. See this section in our supplementary analysis.
- Note: These estimates are different from our effective coverage year estimate because they are absolute measures. Our equivalent coverage year figure is a relative estimate which compares the amount of protection nets provide now to the level of protection provided by nets in the Cochrane RCTs.
- The fall from 61% of nets being in serviceable condition at the end of year 2 to 30% in year 3 implies a deterioration rate of 50% by the end of three years. We extrapolate to years 4 - 6 by assuming that this rate will increase over time as nets get older. We roughly guess that the deterioration rate will be 67% in year 4, 80% in year 5, and 100% in year 6. This implies:
- 10% of nets will survive and be in serviceable condition at the end of year 4 (30% x (100% - 67%))
- 2% at the end of year 5 (10% x (100% - 80%))
- 0% at the end of year 6. See this section in our supplementary analysis.
- We estimate the proportion of nets surviving and in serviceable condition during each year (rather than at the end) by taking the average of one year end and the next year end. This gives estimates of:
- 20% of nets surviving and in serviceable condition at the midpoint of year 4 ((30% + 10%) / 2)
- 6% at the midpoint of year 5 ((10% + 2%) / 2)
- 1% at the midpoint of year 6 ((2% + 0%) / 2). See this section in our supplementary analysis.
- Next, we convert the % of nets surviving and in serviceable condition in years 4 - 6 back into an estimate of equivalent coverage years as follows:
- We take the ratio between % of nets surviving and in serviceable condition at the midpoint of years 1 - 3 and equivalent coverage years in years 1 - 3. On average, the coverage year figure is 10% higher (calculation here).
- We assume that this ratio will be the same in years 4 - 6, and multiply our estimates of the proportion of nets surviving and in serviceable condition at the midpoint of each year by 10%.
- This gives final estimates of:
- 0.22 years of effective coverage during year 4 (20% x 10%)
- 0.07 years during year 5 (6% x 10%)
- 0.01 years during year 6 (1% x 10%)
- First, we estimate the proportion of nets which are surviving and in serviceable condition during and at the end of years 1 - 3 based on the durability data we have reviewed (discussed above). We estimate 85% of nets will survive and be serviceable at the end of year 1, 61% at the end of year 2 and 30% at the end of year 3. The estimates during each year are 92%, 71% and 45% respectively. See this section in our supplementary analysis.
- 102
As discussed above, the figures for years of effective coverage are based on the PermaNet 2.0 only. We estimate that generic LLINs have 15% lower durability relative to the PermaNet 2.0. We calculate this -7% adjustment based on their durability being 15% lower, and our estimate that 47% of LLINs purchased by AMF between 2018 and 2020 were generic (15% x 47% = 7%). See this section in our cost-effectiveness analysis for our calculations.
- 103
This adjustment is based on the same data that we use to estimate 17% lower overall durability in DRC (discussed above). We break down the durability penalty by year in these calculations (-12% in year one, -16% in year two, and -32% in year three) based on the data analyzed in this spreadsheet. For years four to six, for which we do not have field monitoring data, we roughly guess that the percentage difference between the adjustment values for years 3 and 4 will be the same as the percentage difference between the adjustment values for years 2 and 3. We roughly guess that this pattern would continue into years 5 and 6 following a distribution, which in practice leads the adjustment to reach its maximum of 100% during year 5. See this section of our cost-effectiveness analysis.
- 104
See this section in our cost-effectiveness analysis.
- 105
For example, we think that nets in DRC provide 0.81 years of effective coverage in year 1 and 0.60 years of effective coverage in year 2. These figures are averages for each year, so we assume that they apply to the midpoint of each year (6 and 18 months respectively). We then assume linear decay in each successive month between these figures. See this sheet for our calculations.
- 106
See this cell for this calculation.
- 107
See this section in our cost-effectiveness analysis.
- 108
For our reasoning by location, see the following sources:
- DRC: This is our rough best guess of the average campaign interval based on information we have received from AMF on the distribution schedule for past and future campaigns.
- South Sudan: This spreadsheet contains a summary of our best guess about the likely interval between campaigns in each province with and without AMF funding.
- Nigeria: Our reasoning in Nigeria (discussed in this spreadsheet) is based on unpublished sources about the schedule of future distributions.
- 109
See this section of our cost-effectiveness analysis.
- 110
See this row in our cost-effectiveness analysis.
- 111
See this row in our cost-effectiveness analysis.
- 112
See this row in our cost-effectiveness analysis.
- 113
Our approach is:
- We estimate the number of years of effective coverage remaining per net at the point we think new campaigns are most likely to happen without AMF funding (see this row in our analysis).
- We then estimate the number of years of effective coverage remaining per net at the point we think new campaigns are most likely to happen with AMF funding (see this row in our analysis). This is based on our analysis of the likely impact of AMF’s funding in these countries (discussed above).
- We deduct the coverage years lost from residual nets being discarded if AMF does not provide funding from the coverage years lost from residual nets if it does provide funding, to calculate the overall change in coverage years lost due to residual nets as a result of AMF’s funding. See this section for our calculations.
Note: our calculations also factor in our estimates that ITNs have lower durability in DRC (discussed above).
- 114
See this row in our cost-effectiveness analysis.
- 115
See this row in our durability model.
- 116
This study is Kilian et al. 2011.
- 117
“First, there is as yet no clear definition of the minimal effective dose still acceptable and its equivalent in bio-assay tests. The WHOPES cut-off of 80% of nets effective in WHO cone bioassays (with ≥95% Knock-Down or ≥80% mortality) or tunnel tests (≥80% mortality or ≥90% blood-feeding inhibition) is designated as the optimal level required after three years of use to decide on recommendation for public health use, not as an end-of life determination or a minimally acceptable performance. Existing data suggests that high Knock-Down rates and mortality can be achieved at very low levels of insecticide, much lower than what has been seen after three years in WHOPES Phase III evaluations (see WHOPES reports).” WHO, Vector Control Technical Expert Group Report to MPAC September 2013, p. 9.
- 118
This is because we conducted the analysis feeding into our durability model when using an older version of our cost-effectiveness analysis, which primarily relied on the all-cause mortality data.
See this sheet for the details of our analysis. - 119
Our best guess based on some initial (unpublished) analysis is that updating our model to incorporate data from the studies which measured incidence will not substantially change our bottom line. This is because some of the factors informing our analysis are present in both sets of studies (although the amount of data available is limited). These factors include shorter duration compared to the lifespan of contemporary LLIN distributions and activities to train participants on net care and use in some studies.
- 120
Our net durability calculations are based on studies that: i) provide free bed nets to households; ii) follow-up to see how long these bed nets were in use. These studies were conducted much more recently (mostly in the 2010s) than the mortality/incidence trials. If people were getting nets from other sources after having received a free net, this should "show up" in these studies (and our durability assumptions).
- 121
In particular, baseline coverage in the control group was “very low” in Marbiah 1997; 6% in Nevill et al. 1996, 9% in Sexton et al. 1990, and 12% in Sochantha et al. 2006.
- 122
See calculations here, which look at Demographic and Health Survey (DHS)/Malaria Indicators Survey (MIS) data on bed net access in Uganda, Nigeria, Guinea and Togo. Note that this relates to households that own bed nets; when we look at the whole sample (i.e., not conditional on ownership), 53% of households in Guinea received a bed net from a mass distribution campaign, 44% in Nigeria, 59% in Togo, and 77% in Uganda.
- 123
“We find that uptake drops by 60 percentage points when the price of ITNs increases from zero to $0.60 (i.e. from 100 to 90 percent subsidy), a price still $0.15 below the price at which ITNs are currently sold to pregnant women in Kenya.” Cohen and Dupas 2010, p. 1.
- 124
This is still substantially less than the cost of a net. If people had to pay the full price, we’d expect demand to dip even lower.
- 125
For reference, across the whole of Guinea in 2021, 9% of households received nets from continuous channels and 1% from shops. We’d expect this would be higher if we netted out the impact of mass distribution campaigns, since we’d expect people to respond to no mass campaigns by seeking out nets elsewhere. See GiveWell, DHS/MIS data on net access for our analysis of net sources.
- 126
In the simplest possible case, if counterfactual coverage was 0% in the trials and we think it would be 20% today, this would cash out as a 20% reduction in counterfactual impact/cost-effectiveness. Since coverage in the control group was not 0% in the trials, we need to account for some counterfactual coverage already being "baked-in" to the treatment effect. That’s done in this back-of-the-envelope calculation.
- 127
One reason why continuous distribution channels might not be able to "step up" in the absence of mass distribution campaigns is if there are significant logistical challenges with keeping multiple health centers/touchpoints continuously restocked. We plan to investigate whether this is something we can help improve in the future.
- 128
See this section of our cost-effectiveness analysis.
- 129
See this row and this row in our cost-effectiveness analysis. Note that Chad and South Sudan are included in our cost-effectiveness analysis but fall under our cost-effectiveness bar. GiveWell previously considered making a grant to AMF to support a net campaign in Chad, but declined to make the grant because we estimated the campaign would be under our cost-effectiveness bar. GiveWell previously made a grant to AMF’s program in South Sudan, contingent on AMF providing GiveWell with updated cost-effectiveness information. After receiving the data, we concluded that the program in South Sudan fell under our cost-effectiveness bar. As a result, AMF agreed to save the grant funding for another opportunity and funded the campaign in South Sudan using its own funds.
- 130
See this row in our cost-effectiveness analysis. Note that this is our initial estimate before we apply supplemental adjustments.
- 131
See this row in our cost-effectiveness analysis. This range includes DRC, Guinea, Nigeria (Global Fund and PMI states), Togo, and Uganda only (excluding Chad and South Sudan) for the reasons discussed in this section.
- 132
Pryce et al. 2018, Analysis 1.2, p. 55.
- 133
See this row in our cost-effectiveness analysis. This range includes DRC, Guinea, Nigeria (Global Fund and PMI states), Togo, and Uganda only (excluding Chad and South Sudan) for the reasons discussed in this section.
- 134
See here in our cost-effectiveness analysis.
- 135
Cochrane, formerly known as the Cochrane Collaboration, is a not-for-profit research organization which synthesizes health research in systematic reviews.
“Cochrane is an international network with headquarters in the UK, a registered not-for-profit organization, and a member of the UK National Council for Voluntary Organizations.
…There are now over 7,500 Cochrane Systematic Reviews which we publish in the Cochrane Library. We also play a key role in developing new methods in evidence synthesis.” Cochrane, "About us" - 136
Pryce et al. 2018 is an update to an earlier Cochrane meta-analysis, Lengeler 2004a, and assesses the impact of insecticide resistance on ITN effectiveness since Lengeler 2004a was published. It incorporates three RCTs that were not included in Lengeler 2004a and excludes two RCTs which were previously included.
“A previous version of this Cochrane Review identified that insecticide-treated nets (ITNs) are effective at reducing child mortality, parasite prevalence, and uncomplicated and severe malaria episodes. Insecticide-treated nets have since become a core intervention for malaria control and have contributed greatly to the dramatic decline in disease incidence and malaria-related deaths seen since the turn of the millennium. However, this time period has also seen a rise in resistance to pyrethroids (the insecticide used in ITNs), raising questions over whether the evidence from trials conducted before resistance became widespread can be applied to estimate the impact of ITNs on malaria transmission today.” Pryce et al. 2018, p. 1.
"After searching for relevant trials up to 18 April 2018, we identified three new randomized controlled trials (studies in which participants are assigned to a treatment group using a random method). In total, we included 23 trials, enrolling more than 275,000 adults and children, to evaluate the effectiveness of ITNs for reducing the burden of malaria." Pryce et al. 2018, pp. 2-3.
"We also screened the full texts of the 22 trials included in the previous version of the review against the inclusion criteria of the review update. Of these, we identified 20 trials for inclusion in the updated review." Pryce et al. 2018, p. 11.
"A previous version of this Cochrane Review [Lengeler 2004a] identified that insecticide-treated nets (ITNs) are effective at reducing child mortality, parasite prevalence, and uncomplicated and severe malaria episodes." Pryce et al. 2018, p. 1.
After revising the review, the authors concluded that the evidence continues to support the main conclusions from Lengeler 2004a: "ITNs, whether compared to no nets or to untreated nets, continue to be effective at reducing child mortality and malaria-related illness in affected areas." Pryce et al. 2018, p. 3
- 137
See GiveWell, Summary of ITN RCTs (March 2023), "1. Studies from Pryce et al. 2018" sheet, "When was the study conducted?" column
- 138
See GiveWell, Summary of ITN RCTs (March 2023), "1. Studies from Pryce et al. 2018" sheet, "Who received nets?" column.
- 139
"Curtains were installed in the 78 intervention villages in June and July 1994 and in the 80 control villages in June and July 1996. All house openings, doors, windows and eaves were covered with mosquito netting. The netting was impregnated by dipping in permethrin, with a target dose of 1 gm/m2. Habluetzel et al. 1997, p. 857. See GiveWell’s Summary of ITN RCTs (March 2023) for all studies.
- 140
"The effectiveness of permethrin-impregnated (0.5 g/m2) bed-nets and curtains as malaria control measures was evaluated in Uriri, Kenya in 1988. One hundred five families were randomly assigned to 1 of 3 study groups (control, bed-net, or curtain)." Sexton et al. 1990, p. 11. See GiveWell’s Summary of ITN RCTs (March 2023) for all studies.
- 141
See GiveWell’s Summary of ITN RCTs (March 2023), "1. Studies from Pryce et al. 2018" sheet, "What was the intervention?" column.
- 142
See GiveWell’s Summary of ITN RCTs (March 2023), "1. Studies from Pryce et al. 2018" sheet, "What they did to ensure that ITNs were used and used properly" column.
- 143
See our discussion of usage here and net durability here. Note that some contemporary LLIN distributions we have seen involve promotional activities to notify households about the upcoming distribution and encourage net usage, but we have not seen campaigns involving post-distribution visits to a meaningful proportion of households to encourage high usage and better maintenance.
- 144
- Our best guess is that all the ITNs evaluated in Pryce et al. were conventional ITNs, although we cannot say for sure. See this column in our summary of the studies underlying Pryce. Most studies explicitly mentioned the need for nets to be retreated (indicating that the nets were conventional ITNs, not LLINs), but in some cases no information on retreatment was provided. Our impression is that LLINs were less common in the 1980s and 1990s when most of the studies were conducted, and so it is unlikely that LLINs would have been used.
- One study, Smithuis et al. 2013, states that nets were factory-treated by the manufacturer before the study began. This implies that the nets may have been LLINs, although this is not certain. Smithuis only receives a very small amount of weight in the meta-analysis of all-cause mortality in Pryce (0.07%), so we do not weigh this uncertainty very highly in our analysis.
- “More than 5000 ITN were distributed. The ITN (green colour, polyester, size 130 × 180 × 150 cm (11.6 m2) or 190 × 180 × 150 cm (14.5 m2), Siam-Dutch Co, Thailand) were already impregnated with deltamethrin (25 mg/m2) by the manufacturer.” Smithuis et al. 2013, p. 4.
- Source for meta-analysis weights: Pryce et al. 2018, p. 55 (analysis 1.1).
- 145
See GiveWell, Summary of ITN RCTs (March 2023), "Did nets need to be retreated?" column. The frequency of retreatment in the studies in Pryce is a factor in our analysis of ITNs durability compared to the conventional ITNs evaluated in Pryce (see this section of the review for more information).
Note that our analysis of durability in Pryce et al. is based on the studies which measured all-cause child mortality, not the studies measuring malaria incidence that we primarily rely on in our cost-effectiveness model. We have not yet updated our durability model to account for any differences between the studies measuring all-cause child mortality and the studies measuring malaria incidence.
- 146
“Of the 23 RCTs meeting the inclusion criteria, two were individually randomized. The remaining 21 trials were cRCTs. In 15 trials, the unit of randomization was the village or larger administration unit, while six trials used households as the unit of randomization.” Pryce et al. 2018, p. 13.
- 147
See GiveWell, Summary of ITN RCTs (March 2023), "Time between distribution and outcome measurement?" column.
- 148
See this column in GiveWell’s Summary of ITN RCTs (March 2023). The study durations were:
- Henry 2005: 1 year
- Marbiah 1998: 1 year
- Nevill et al. 1996: 2 years
- Sexton et al. 1990: 15 weeks
- Sochantha et al. 2006: 10 months
- 149
See this column in GiveWell’s Summary of ITN RCTs (March 2023). Smithuis et al. 2013 was shorter than the other studies (10 months), but receives only a tiny percentage of the meta-analysis weight (more here).
- 150
“Campaigns should also normally be repeated every three years, unless available empirical evidence justifies the use of a longer or shorter interval between campaigns.” WHO, Guidelines for Malaria Vector Control, 2019, pp. 39-40.
- 151
See GiveWell, Summary of ITN RCTs (March 2023), "Net usage" columns.
- 152
Our cost-effectiveness analysis uses the five studies which estimate the impact of ITNs vs no nets on uncomplicated episodes of P. falciparum malaria as its starting point for estimating reductions in child mortality. These are summarized in Pryce et al. 2018 Analysis 1.2, p. 55. Our reasoning for focusing on these studies specifically is discussed here.
- 153
“A previous version of this Cochrane Review identified that insecticide-treated nets (ITNs) are effective at reducing child mortality, parasite prevalence, and uncomplicated and severe malaria episodes. Insecticide-treated nets have since become a core intervention for malaria control and have contributed greatly to the dramatic decline in disease incidence and malaria-related deaths seen since the turn of the millennium. However, this time period has also seen a rise in resistance to pyrethroids (the insecticide used in ITNs), raising questions over whether the evidence from trials conducted before resistance became widespread can be applied to estimate the impact of ITNs on malaria transmission today.” Pryce et al. 2018, p. 1.
- 154
See GiveWell, Insecticide resistance adjustment analysis, 2019, pp. 11-18.
Note that our analysis looks only at studies included in an earlier version of the Cochrane meta-analysis, Lengeler 2004a, as well as one new study (Sochantha et al. 2006) which was included in Pryce et al. but not Lengeler (and in which our best guess is that mosquito populations were susceptible to insecticide). We have not updated our analysis of insecticide resistance to account for all the changes between Lengeler and Pryce. However, only one study (Smithuis et al. 2013) comparing ITNs vs no nets (as opposed to ITNs vs untreated nets) was added to Pryce but is not included in our analysis. We do not expect our conclusions would significantly change if we reviewed Smithuis. - 155
GiveWell, Insecticide resistance adjustment analysis, 2019. Note that the figures summarized here differ from the summary on p. 17 of this analysis, because we also include Sochantha et al. 2006 (where the resistance level was unknown) in our summary.
- 156
Our cost-effectiveness analysis uses the five studies which estimate the impact of ITNs vs no nets on uncomplicated episodes of P. falciparum malaria as its starting point for estimating reductions in child mortality. These are summarized in Pryce et al. 2018, Analysis 1.2, p. 55. Our reasoning for focusing on these studies specifically is discussed here.
- 157
GiveWell, Insecticide resistance adjustment analysis, 2019, pp. 12-13.
- 158
Pryce et al. also analyzes the impact of ITN distributions compared to untreated nets. We focus on the findings relating to ITNs vs no nets in our analysis, as we expect that in the absence of ITN distributions, people are more likely to not use nets at all rather than use untreated nets.
- 159
All analyses summarized in Pryce et al. 2018, pp. 4-5.
- 160
Note that two of the studies providing data for this estimate included children up to age 10 in their analysis (Binka 1996 and Smithuis 2013). These studies comprise only ~15% of the meta-analysis weight for this outcome, so we feel relatively confident that this estimate is a good approximation of the effect for children under age five.
- 161
- Incidence is the rate of new cases in a given unit of time. This contrasts with prevalence, the proportion of people with a disease or condition at or during a particular time period (regardless of when they first contracted it).
“Incidence refers to the number of new cases of disease in a given population. An incidence rate expresses the number of new cases of a disease divided by the total number of persons at risk for the disease…Prevalence is the proportion of a population with a specific disease or condition. It is a measure of the total number of cases in a defined population at a particular time or during a given time period.” National Library of Medicine, Finding and Using Health Statistics, "Conditions"
- The specific definitions used in the studies in Pryce et al. were site specific. Prevalence was measured by estimating parasitaemia; incidence was measured using site-specific definitions, including measured or reported fever, with or without parasitological confirmation.
“Uncomplicated clinical episodes: measured using site-specific definitions, including measured or reported fever, with or without parasitological confirmation. Measurements were usually done in the frame of prospective longitudinal studies, as a rate of episodes per unit of time (incidence). We also included trials using validated retrospective assessments in the frame of cross-sectional surveys, providing a percentage of the population who had experienced an uncomplicated episode in a unit of time (cumulative incidence). When reported separately, P falciparum and P vivax episodes were analysed separately. We also included trials that reported the incidence of episodes of any Plasmodium species.
Parasite prevalence: parasite prevalence due to P falciparum and P vivax was obtained using the site-specific method for estimating parasitaemia, usually thick or thin blood smears or both. When more than one survey was done, the reported prevalence result is the average prevalence of all the surveys.” Pryce et al. 2018, p. 9.
- 162
“The public health burden posed by P. vivax is no longer regarded as benign, causing severe morbidity and death. Nevertheless, P. falciparum remains the single most important threat to public health at a global scale, accounting for more than 90% of the world’s malaria mortality.” Snow 2015, p. 1.
- 163
Pryce et al. 2018, p. 55 (Analysis 1.1 and Analysis 1.2). Nevill et al. 1996 is the only study included in both Analysis 1.1 and Analysis 1.2.
- 164
Prevalence is the proportion of people with a disease or condition at or during a particular time period (regardless of when they first contracted it).
“Incidence refers to the number of new cases of disease in a given population. An incidence rate expresses the number of new cases of a disease divided by the total number of persons at risk for the disease…Prevalence is the proportion of a population with a specific disease or condition. It is a measure of the total number of cases in a defined population at a particular time or during a given time period.” National Library of Medicine, Finding and Using Health Statistics, "Conditions" - 165
Pryce et al. 2018, Figure 2. "Risk of bias' summary: review authors' judgements about each risk of bias item for each included study," pp. 14-15.
- 166
See this row in our cost-effectiveness analysis.
- 167
- Since the studies in Pryce were conducted, child mortality from various causes has fallen significantly. See our analysis of changes in all cause under-five mortality in this spreadsheet. This analysis is based on estimates from the Global Burden of Disease Project.
- We also believe that using reductions in malaria cases as the starting point for our analysis and assumptions about non-malaria deaths indirectly averted makes our analysis relatively simple and transparent, compared to modeling reductions in all-cause mortality and then accounting for a changing share of all-cause mortality being attributable to malaria over time. See this version of our cost-effectiveness analysis for a previous version which used a different method, based directly on the estimated reduction in all-cause mortality from Pryce et al.
- 168
The two studies are Sexton et al. 1990 and Sochantha et al. 2006. See this spreadsheet for further details.
- 169
See this section of the review for further details.
- 170
We confirmed with the author of the previous version of this review (Lengeler 2004a) that the all-cause mortality figures are based on an "intention to treat" analysis—i.e., "protected" refers to children in the treatment group, not to children who were confirmed to own or use ITNs; we assume this remains the case in Pryce et al. 2018 because the studies that make up the analysis are largely unchanged.
- 171
45% / 70% = 64%. See this row in our cost-effectiveness analysis.
- 172
We have previously heard from malaria researchers that community effects are likely to be some portion of the protection provided by nets, but that the level of protection provided by these effects has not been well quantified.
"When you're moving from protecting only children to protecting everybody, you multiply your costs by a factor of five, but you also get at least twice as much effect and we know that from both modeling and empirical impact assessments … I don't think we will ever really have the reply to that question [about the relative magnitude of community-level effects]." Christian Lengeler, author of Cochrane Review of insecticide-treated bed nets, phone conversation with GiveWell, November 2, 2011
"There are empirical studies that show that there seems to be a community-level impact of ITNs. There are theoretical studies that show that there ought to be a community-level effect. What I don't think there is is any attempt to estimate the magnitude of the community-level effect from empirical data. We've done this with mathematical models, but haven't completed the linkage with empirical data that could help with this estimate." GiveWell's non-verbatim summary of a conversation with Thomas Smith on November 8, 2011
"The argument for ITNs has always been that ITN coverage is a public good. Some of the good accomplished is not internalized to the person using the net. Some people argue that there's a negative externality as well - unprotected people are getting bitten by the mosquitoes that would have bitten the protected people - but I don't think you can make that argument with ITNs … What I do is analysis of data using mathematical models. In general, the leading models say that the more people use the nets, the bigger the positive externalities are … If you're talking about the marginal dollar for more nets, there's a lot more uncertainty on the cost-effectiveness of that than we'd like. The only data that we have is bad data. Improved surveillance would be helpful." GiveWell's non-verbatim summary of a conversation with Dave Smith on November 4, 2011
- 173
We’re not sure whether this could lead us to overestimate or underestimate the impact of using nets. Some factors informing our thinking are:
- All five studies measuring malaria incidence in the Cochrane meta-analysis were cluster randomized, not individually randomized (more here). Four of these, accounting for ~80% of the meta-analysis weight for this outcome, were randomized at the community or village level. We would guess that in these studies the benefits of nets on reducing malaria transmission would be concentrated within each community in the intervention group, and there would be few positive “spillovers” (from reduced malaria transmission) to control group communities.
- One study (Sexton et al. 1990, accounting for ~20% of the meta-analysis weight) randomized at the household level (more here). This implies that some households in the control group living in the same communities may have also received some benefit as a result of reduced malaria transmission. This implies that this study’s reported findings are likely to underestimate the impact of nets.
- Within all the studies, there are likely to be some positive spillovers from people who did use nets to people who did not within the intervention group, so long as they are living in the same communities. This implies that we could be overestimating the benefits of using nets with a simple conversion from intention-to-treat to treatment-on-the-treated, because we're attributing all the benefits of nets to people who use them whereas actually some benefits accrue to people who don't use them.
- We don’t think the latter point is a significant concern if levels of usage now are similar to usage in the underlying studies. Although we would be overestimating the benefit to individuals using nets compared to those not using nets, we don’t think we would be overestimating the overall impact of the program.
Note: our analysis of Seasonal Malaria Chemoprevention (one of our other top recommended programs, as of December 2023), includes an estimate of reduced mortality from spillovers to older children and adults not receiving the program (Seasonal Malaria Chemoprevention is usually targeted at children under five). We do not use this approach for nets because we would expect the main benefit for older children and adults comes from actually using nets themselves (which we account for separately, more in this section).
- 174
See this row in our cost-effectiveness analysis. This range includes DRC, Guinea, Nigeria (Global Fund and PMI states), Togo, and Uganda only (excluding Chad and South Sudan) for the reasons discussed in this section.
- 175
See the "Insecticide Resistance" sheet of our cost-effectiveness analysis for our full calculations.
- 176
- “Insecticide-treated bed nets and curtains (ITNs) compared to no nets for preventing malaria
Patient or population: people of all ages living in malaria transmission settings
Setting: Burkina Faso 1996 (Halbluetzel 1996); Cameroon 1992 (Moyou-Somo 1995); Cambodia 2002 (Sochantha 2006); Ghana 1995 (Binka 1996); Ivory Coast 2000 (Henry 2005); Kenya 1988 (Sexton 1990); Kenya 1995 (Nevill 1996) and 1998 (Phillips-Howard 2003); Myanmar 1999 (Smithuis 2013); Sierra Leone 1993 (Marbiah 1998); Pakistan 1991 (Rowland 1996); Tanzania 1996 (Fraser-Hurt 1999)" Pryce et al. 2018, p. 4.- "Insecticide-treated bed nets and curtains (ITNs) compared to untreated nets (UTNs) for preventing malaria
Patient or population: people of all ages living in malaria transmission settings
Setting: Colombia 1993 (Kroeger 1995 (Colombia)); Ecuador 1992 (Kroeger 1995 (Ecuador)); Gambia 1993 (D'Alessandro 1995); Gambia 1985 (Snow 1987); Madagascar 1994 (Rabarison 1995); Nicaragua 1996 (Kroeger 1999); Peru Amazon 1992 (Kroeger 1995 (Peru Amazon)); Peru Coast 1993 (Kroeger 1995 (Peru Coast)); Thailand 1988 (Kamol- Ratanakul 1992); Thailand 1991 (Luxemburger 1994); Venezuela 2000 (Magris 2007).” Pryce et al. 2018, p. 6. - 177
“A previous version of this Cochrane Review identified that insecticide-treated nets (ITNs) are effective at reducing child mortality, parasite prevalence, and uncomplicated and severe malaria episodes. Insecticide-treated nets have since become a core intervention for malaria control and have contributed greatly to the dramatic decline in disease incidence and malaria-related deaths seen since the turn of the millennium. However, this time period has also seen a rise in resistance to pyrethroids (the insecticide used in ITNs), raising questions over whether the evidence from trials conducted before resistance became widespread can be applied to estimate the impact of ITNs on malaria transmission today.” Pryce et al. 2018, p. 1.
- 178
See this section of the report for further details.
- 179
“The WHO insecticide susceptibility bioassay that is the subject of these revised guidelines is a simple direct response-to-exposure test. Mosquitoes are exposed to known concentrations of an insecticide for a fixed period of time at the end of which the number of fatalities is recorded. In its present form, the test is designed to distinguish between baseline susceptibility and resistance to insecticides in adult mosquitoes. As such, the test is intended to be used as a field and laboratory surveillance tool with the limitation that it gives little information on the underlying mode(s) or mechanism(s) conferring resistance where detected.” WHO, Test procedures for insecticide resistance monitoring in malaria vector mosquitoes, 2013, p. 4.
- 180
See this sheet in our supplementary analysis.
- 181
See here for this range.
- 182
See our summary in this cell note. This is a very rough adjustment based on a single estimate from a 2018 WHO report, which found that resistance to permethrin (a common type of insecticide used in ITNs) increased by five percentage points from 2010 to 2016 (0.83 percentage points per year on average).
Note: this is measured between the average date that the tests were conducted and the next year we expect nets to be distributed in each country.
“Trends analyses were conducted to determine whether there were any significant changes between 2010 and 2016 in malaria vector resistance to specific insecticides, and in specific vector groups (Fig. 4.4 and Fig. 4.5). A global increase in resistance frequency was observed for all pyrethroid insecticides tested. Increases were greatest for etofenprox (44% rise, from 7% to 51%), alphacypermethrin (40% rise, from 10% to 50%) and cyfluthrin (28% rise, from 4% to 32%). The increase was less pronounced for the other pyrethroids although these also had a higher initial resistance frequency in 2010: deltamethrin (14% rise, from 20% to 34%), permethrin (5% rise, from 40% to 45%) and lambda-cyhalothrin (3% rise, from 33% to 36%). This indicates that increasing resistance is an issue for all pyrethroids, and that reductions in susceptibility are most marked for those insecticides for which susceptibility was highest in 2010. Further evaluations will be undertaken to identify whether there are differences in resistance frequency and trends over time between insecticides of the pyrethroid class, in order to guide requirements for insecticide resistance monitoring.” WHO, Global report on insecticide resistance in malaria vectors: 2010–2016, p. 20.
- 183
"Although there are limited options for [resistance management] with LLINs, they may retain an effect despite increased resistance to pyrethroids. Firstly, nets provide a physical barrier against biting by mosquitoes as long as they are intact (2). Secondly, in most vector species, resistance to pyrethroids does not completely reduce the effect of the insecticide. It has also been observed that the irritancy of pyrethroids (‘hyperexcitatory response’) may reduce mosquito blood-feeding or encourage diversion to other hosts by certain vector species that do not feed exclusively on human hosts. This effect can vary, however, by species and geographical location." WHO, Global Plan for Insecticide Resistance Management in Malaria Vectors, 2012, p. 45.
- 184
This estimate is based on comparing the protective efficacy of ITNs compared to no nets against the efficacy of ITNs compared to untreated nets in the Cochrane meta-analysis. Because untreated nets offer a physical barrier to mosquitoes but no protection from insecticide, we can infer the proportion of benefits attributable to insecticide vs the physical barrier from this comparison. We:
- Compare the protective efficacy of ITNs vs no nets against ITNs vs untreated nets across eight outcomes reported in the Cochrane review.
- We exclude two outcomes which we believe are outliers (malaria prevalence at <1 year follow-up for P. falciparum and P. vivax malaria). Each outcome is estimated based on only one study, and indicates that ITNs had a negative impact compared to either no nets or untreated nets.
- We infer the proportion of the benefit attributable to insecticide for each outcome.
- Finally, we calculate a weighted average using the number of studies calculating each outcome as the weights. This produces the final estimate that 73% of the total benefits in the Cochrane review were attributable to insecticide.
Our calculations are available on this sheet. Note that our analysis is based on earlier version of the Pryce et al. 2018 meta-analysis, Lengeler 2004a. We have not updated our analysis to account for the differences between Lengeler and Pryce.
- Compare the protective efficacy of ITNs vs no nets against ITNs vs untreated nets across eight outcomes reported in the Cochrane review.
- 185
Our calculations use the following method:
- We multiply our estimate of mosquito mortality for each country by the proportion of benefits attributable to insecticide (e.g., 38% x 73% in Uganda).
- Next, we add the 27% of the protection we estimate is attributable to the physical protection of the net.
- From this we can calculate the reduction in effectiveness from insecticide resistance (38% x 73%) + 28% = 55% effectiveness compared to the meta-analysis we rely on, or a -45% reduction in effectiveness.
See this section of our analysis for our calculations. Note: Madagascar is excluded from this range because it is not (as of December 2023) one of the countries in our cost-effectiveness analysis.
- 186
This is because, for the purposes of this adjustment, we assume insecticide resistance was not present in the studies in the meta-analysis (more here). We incorporate a +5% adjustment elsewhere in our analysis because we have seen some data suggesting resistance may have been present in some studies in the meta-analysis (more here).
- 187
See this section of the report for further details on each type of next-generation net, and the March 2023 WHO recommendations.
- 188
See our analysis on this sheet.
- 189
See this sheet in our analysis for the full dataset we have analyzed.
- 190
See this row in our analysis for our calculations.
- 191
The WHO recommends that only locations with mono-oxygenase based resistance mechanisms are susceptible to PBO treatment and recommended for PBO net deployment.
“Pyrethroid-PBO nets prequalified by WHO are conditionally recommended for deployment instead of pyrethroid-only LLINs where the principal malaria vector(s) exhibit pyrethroid resistance that is: a) confirmed, b) of intermediate level,3 and c) conferred (at least in part) by a monooxygenasebased resistance mechanism, as determined by standard procedures.” WHO, Guidelines for Malaria Vector Control, 2019, p. xvii.
For more on different types of insecticide resistance, see this section of our separate report on insecticide resistance. This is old and some sections may be out of date. - 192
For this estimate, we use data from the WHO Malaria Threat Map and IR Mapper to estimate:
- The proportion of test sites with detected pyrethroid resistance (e.g., 99% in Uganda).
- The proportion of test sites with mono-oxygenase based resistance (as our understanding is that PBOs will only be more effective in locations with this type of resistance) (e.g., 83% in Uganda).
We multiply these figures together (e.g., 99% x 83% = 82% in Uganda) to produce an estimate of the proportion of each country where we think PBOs are likely to be more effective than standard LLINs. See this section of our analysis.
- 193
See this row in our analysis.
- 194
See this grant page for further details.
- 195
We updated our estimates for DRC only because AMF has told us that, if it contributes funding to 2024 campaigns in the DRC, it plans to purchase and distribute a substantial number of nets treated with a second insecticide (chlorfenapyr), as well as a smaller number of other Dual AI nets. This update was time-sensitive for DRC because we planned to use these estimates for a pending grant decision. We have not yet updated our estimates for other countries, because our analysis of chlorfenapyr nets is still ongoing. See this changelog entry for further details.
- 196
- 197
The recommendations cover:
- Chlorfenapyr nets, which use both chlorfenapyr insecticide and a pyrethroid.
- Pyriproxyfen nets, which combine a pyrethroid with an insect growth regulator (IGR). The IGR disrupts mosquito growth and reproduction.
“New recommendations, published today in the WHO Guidelines for malaria, cover 2 new classes of dual ingredient ITNs with different modes of action:
Pyrethroid-chlorfenapyr nets combine a pyrethroid and a pyrrole insecticide to enhance the killing effect of the net.
Pyrethroid-pyriproxyfen nets combine a pyrethroid with an insect growth regulator (IGR). The IGR disrupts mosquito growth and reproduction…
…New recommendation on pyrethroid-chlorfenapyr nets vs pyrethroid-only nets
WHO is issuing a strong recommendation for the deployment of pyrethroid-chlorfenapyr ITNs vs pyrethroid-only nets to prevent malaria in adults and children in areas where mosquitoes have become resistant to pyrethroids.
The recommendation considers that, compared to pyrethroid-only nets or pyrethroid-PBO nets, pyrethroid-chlorfenapyr ITNs should have an increased killing effect against pyrethroid-resistant malaria vectors and, thus, a greater impact against malaria.
New recommendation on pyrethroid-chlorfenapyr nets vs pyrethroid-PBO nets
WHO is issuing a conditional recommendation for the deployment of pyrethroid-chlorfenapyr ITNs instead of pyrethroid-PBO nets to prevent malaria in adults and children in areas with pyrethroid resistance.
The conditionality of the recommendation is based on the judgement of the WHO Guidelines Review Group (GDG) that the balance of desirable and undesirable effects probably favours pyrethroid-chlorfenapyr nets over pyrethroid-PBO nets. The recommendation is based on evidence drawn from only one trial in Africa.” WHO, "WHO publishes recommendations on two new types of insecticide-treated nets," 2023
- 198
"Although there are limited options for [resistance management] with LLINs, they may retain an effect despite increased resistance to pyrethroids. Firstly, nets provide a physical barrier against biting by mosquitoes as long as they are intact (2). Secondly, in most vector species, resistance to pyrethroids does not completely reduce the effect of the insecticide. It has also been observed that the irritancy of pyrethroids (‘hyperexcitatory response’) may reduce mosquito blood-feeding or encourage diversion to other hosts by certain vector species that do not feed exclusively on human hosts. This effect can vary, however, by species and geographical location." WHO, Global Plan for Insecticide Resistance Management in Malaria Vectors, 2012, p. 45.
- 199
See this row in our insecticide resistance adjustment calculations.
- 200
The five studies we rely on most are those which estimated reductions in malaria incidence from ITN distributions compared to no nets (as discussed in this section). Data from IR Mapper suggests that there was substantial insecticide resistance in the part of Côte d’Ivoire in 1999-2000 where one of these studies, Henry 2005, took place in 1999-2000. See GiveWell, Insecticide resistance adjustment analysis, 2019, pp. 12-13.
- 201
This adjustment is discussed separately in this report.
- 202
Other adjustments reflecting the differences between the studies included in Pryce et al. and contemporary distributions that we discuss elsewhere in this report:
- 203
Pryce et al. 2018, Analysis 1.8, p. 57.
- 204
Extrapolating this finding to estimate the impact on malaria mortality (as opposed to all-cause mortality) is challenging and requires additional assumptions, because we do not have direct data from the studies on the share of deaths attributable to malaria and because we think that some non-malaria deaths may be indirectly caused by malaria. We discuss this issue further in this section.
- 205
See this row in our cost-effectiveness analysis. This range includes DRC, Guinea, Nigeria (Global Fund and PMI states), Togo, and Uganda only (excluding Chad and South Sudan) for the reasons discussed in this section.
- 206
See this row in our cost-effectiveness analysis. This range includes DRC, Guinea, Nigeria (Global Fund and PMI states), Togo, and Uganda only (excluding Chad and South Sudan) for the reasons discussed in this section.
- 207
See our summary of this data here.
- 208
See our state-level estimates for Nigeria here.
- 209
See this row in our cost-effectiveness analysis. This range includes DRC, Guinea, Nigeria (Global Fund and PMI states), Togo, and Uganda only (excluding Chad and South Sudan) for the reasons discussed in this section.
- 210
This understanding is based on multiple conversations with IHME researchers. Detailed modeling assumptions for the GBD estimates are available in the GBD 2019 methods appendix.
- 211
"Despite its importance, current knowledge on the nature and drivers of changing endemicity in sub-Saharan Africa is remarkably weak. National health records in 32 highly endemic countries (together accounting for about 90% of the global malaria burden) are considered inadequate to assess trends in malaria cases. This stems from low care-seeking rates (many malaria cases are not seen at formal health facilities), incomplete record keeping and curation (many recorded cases are never captured in surveillance databases), and historically poor access to parasitological diagnosis (malaria cases were often diagnosed presumptively with poor specificity).” Bhatt et al. 2015, p. 2.
- 212
This is based on the following rough analysis: GiveWell, Analysis of malaria case fatality rates, 2023.
- 213
We have not yet received permission from Rethink Priorities to publish this report: Rethink Priorities, Malaria Deaths: A Comparison of WHO and IHME Estimates, 2023 (unpublished).
- 214
“That data, in fact, shows that WHO mortality estimates are on aggregate nearly 17% less than those published by the IHME, for the assessed year 2019.”
“Later in this report, we will discuss the methodological changes that resulted in the clear split between pre-2021 and post-2021 WHO data. At a glance, the interested viewer can tell that the World Health Organization’s recent changes adjusted aggregate deaths upward significantly, by about 18% over the assessed period 2000-2019.” Rethink Priorities, Malaria Deaths: A Comparison of WHO and IHME Estimates, 2023 (unpublished). - 215
“The bulk of malaria deaths come from the sub-Saharan Africa (SSA) region (85%-91%, depending on the source). In this region, the difference between the 2021 WHO data and the most recent IHME model is around 7% for the assessed years 2017-2019, compared to a global gap of around 11%. Over the period 2000-2019, the overall difference for sub-Saharan Africa is around 12%, whereas the global gap between the two organizations' estimates is closer to 17%.” Rethink Priorities, Malaria Deaths: A Comparison of WHO and IHME Estimates, 2023 (unpublished).
- 216
“As deaths for children under 5 are a significant component of GiveWell’s model, we looked further into whether adults are indeed the root of the remaining gap between the IHME and WHO datasets. Our primary finding is that the World Health Organization consistently reports about 20-30% higher deaths of children under five than the IHME, whereas its figures for adult deaths are about 50% lower.“ Rethink Priorities, Malaria Deaths: A Comparison of WHO and IHME Estimates, 2023 (unpublished).
- 217
“There is significant controversy over verbal autopsy data and adult deaths. One of the experts we interviewed expressed a worry that IHME data overstates adult mortality and understates child mortality as a pervasive modeling flaw. Indeed, we have found that there is an ongoing debate in the literature about the age structure of malaria mortality. In the 1990s and 2000s, it was widely accepted that in endemic areas, malaria was mostly fatal to children under 5.
When the IHME’s 2012 estimates were released, researchers noticed that the large estimated number of deaths in people older than 5 years in Africa was out of step with other estimates, and criticized the IHME’s reliance on verbal autopsy data, stating “We do not believe that verbal autopsy can distinguish severe malaria from other severe febrile illnesses and so is fundamentally flawed as an estimator of malaria mortality” (White et al, 2012, p. 560).” Rethink Priorities, Malaria Deaths: A Comparison of WHO and IHME Estimates, 2023 (unpublished).
- 218
"During randomized controlled intervention trials aimed at reducing the incidence of infection (but not 100 percent protective), the all-cause mortality of children is often reduced more than would be attributed by VA diagnosis of malaria. For example, in Kilifi the proportion of deaths of children under five years attributed to malaria by VA was 34 percent (R. W. Snow, unpublished data). During a randomized controlled trial of insecticide-treated bednets in the same area, the incidence of malaria infection was reduced by 50 percent (Snow et al. 1996), which was sufficient to reduce all-cause mortality by 33 percent (Nevill et al. 1996). More dramatically, in The Gambia, insecticide-treated bednets reduced all-cause mortality by over 60 percent, and yet the VA-diagnosed contribution of malaria to all-cause mortality among control populations was only 16 percent (Alonso et al. 1993). This has led some to speculate that malaria infection is a contributor to broad causes of mortality beyond the direct fatal consequences of infection (Molineaux 1997)." Jamison et al. 2006, p. 204.
"Data on all-cause mortality of children under five from DSS studies undertaken across a broad range of malaria transmission settings in Sub-Saharan Africa were analyzed against the prevalence of P. falciparum infection at each site. Weighted least-squares regression was used to model the contiguous relationships between all-cause mortality and parasite prevalence rates, allowing for the square of parasite prevalence (for possible saturation of parasite prevalence), timing, location, and the sampling precision of each study (Snow, Korenromp, and Gouws 2004). The unadjusted median all-cause child mortality rate for low prevalence areas of childhood infection (less than 25 percent) was 10.9 per year per 1,000 children under five (IQR 7.8–17.6). This rose dramatically to 39.1 per year per 1,000 children (IQR 32.8–52.2) among populations exposed to childhood parasite prevalence risks greater than or equal to 25 percent. In the regression model, mortality increased significantly with parasite prevalence, but this effect leveled off at higher prevalence rates. The model suggested that, in rural DSS sites throughout Sub-Saharan Africa, all-cause mortality increases by more than twofold (25–30 deaths per 1,000 children under five years old) over the prevalences of malaria infection covered by the DSS sites, and parasite prevalence explained 64 percent of the variation between sites in all-cause under-five mortality. By contrast, the direct estimation of malaria-specific mortality presented earlier for children living under stable endemic conditions was only 28.2 percent." Jamison et al. 2006, p. 206.
- 219
“Indirect consequences of P. falciparum infection include anemia (unless anemia is linked to acute high-density parasitemia as a direct cause), low birthweight, growth retardation, or undernutrition. In addition, malaria infection can increase the severity of other comorbid infectious diseases through immune suppression or enhanced invasive capacities across physical barriers to infection (for example, blood and tissue). Previous approaches to the global burden of disease have assumed that each death must be attributed to a single cause and can be fitted into the fixed disease-mix matrix of all causes (Murray and Lopez 1997).” Jamison et al. 2006, p. 206.
- 220
See this row in our cost-effectiveness analysis.
- 221
Specifically, our analysis of the five studies in Pryce et al. which measured all-cause mortality of ITNs vs no nets implies that to achieve an all-cause mortality reduction of 17%:
- ITN distributions reduced malaria incidence by 45%, and the ratio of direct to indirect malaria deaths is 1.5.
- ITN distributes reduced malaria incidence by 75%, and the ratio of direct to indirect malaria deaths is 0.5.
- Or somewhere in between these, e.g., ITN distributions reduced malaria incidence by 60%, and the ratio of direct to indirect malaria deaths is 0.9.
All of these calculations are based on estimates from the Global Burden of Disease project about the share of malaria deaths at the times and in the countries where the studies were conducted. Overall, we estimate that malaria accounted for 15% deaths in the times and countries where the studies were conducted.
These estimates are uncertain, as discussed in this section of the report. This is one reason why we put only limited weight on the findings of this analysis.
Our calculations for these estimates are available here.
- 222
“Summary of findings for the main comparison. Insecticide-treated bed nets and curtains compared to no nets for preventing malaria Insecticide-treated bed nets and curtains (ITNs) compared to no nets for preventing malaria
Patient or population: people of all ages living in malaria transmission settingsSetting: Burkina Faso 1996 (Halbluetzel 1996); Cameroon 1992 (Moyou-Somo 1995); Cambodia 2002 (Sochantha 2006); Ghana 1995 (Binka 1996); Ivory Coast 2000 (Henry 2005); Kenya 1988 (Sexton 1990); Kenya 1995 (Nevill 1996) and 1998 (Phillips-Howard 2003); Myanmar 1999 (Smithuis 2013); Sierra Leone 1993 (Marbiah 1998); Pakistan 1991 (Rowland 1996); Tanzania 1996 (Fraser-Hurt 1999)...
…Summary of findings 2. Insecticide-treated bed nets and curtains compared to untreated nets for preventing malaria
Insecticide-treated bed nets and curtains (ITNs) compared to untreated nets (UTNs) for preventing malaria
Patient or population: people of all ages living in malaria transmission settingsSetting: Colombia 1993 (Kroeger 1995 (Colombia)); Ecuador 1992 (Kroeger 1995 (Ecuador)); Gambia 1993 (D'Alessandro 1995); Gambia 1985 (Snow 1987); Madagascar 1994 (Rabarison 1995); Nicaragua 1996 (Kroeger 1999); Peru Amazon 1992 (Kroeger 1995 (Peru Amazon)); Peru Coast 1993 (Kroeger 1995 (Peru Coast)); Thailand 1988 (Kamol- Ratanakul 1992); Thailand 1991 (Luxemburger 1994); Venezuela 2000 (Magris 2007)” Pryce et al. 2018.
- 223
See our analysis of changes in all cause under-five mortality in this spreadsheet. This analysis is based on estimates from the Global Burden of Disease Project.
- 224
We do not have documentation from these conversations and so our notes are unpublished.
- 225
“As an example, after all adjustments we estimate that in-line chlorination in Kenya reduces all-cause mortality by 11% in children under five and 2% in people five and over.117 In contrast, an estimate obtained by multiplying the reduction in diarrhea risk caused by in-line chlorination by the GBD estimate of under-five deaths caused by enteric infections in Kenya is 2.9%, suggesting that our estimate is about 3.7 times as large as expected based on indirect estimation methods.118 This implies that for each enteric infection death averted in children under five, 2.7 deaths are averted from other causes.” See this section of our report on water quality interventions.
- 226
See this row in our cost-effectiveness analysis.
- 227
Alexandra Walker, Engagement Officer, IHME, email to GiveWell, July 21, 2021 (unpublished).
- 228
See this row in our cost-effectiveness analysis. This range includes DRC, Guinea, Nigeria (Global Fund and PMI states), Togo, and Uganda only (excluding Chad and South Sudan) for the reasons discussed in this section.
- 229
This calculation uses the following formula:
- Mortality overall = (Mortality among those not using nets x % not using nets) + (Mortality among those using nets x % using nets). This is equal to:
- (Mortality among those not using nets x % not using nets) + (Mortality among those not using nets x relative risk of mortality from using nets x % using nets). This implies:
- Mortality among those not using nets = Mortality overall / (relative risk of mortality from using nets x % using nets + % not using nets).
See this row in our cost-effectiveness analysis.
- 230
See this row in our cost-effectiveness analysis.
- 231
This issue is discussed further in relation to the protective effect of using ITNs in this section of the report.
- 232
GiveWell also supports SMC campaigns and an organization implementing SMC campaigns (Malaria Consortium) is one of GiveWell’s top recommended organizations. See our SMC report here for further details.
- 233
See Malaria Consortium’s Seasonal Malaria Chemoprevention 2021 Philanthropy report for details by country.
- 234
Alexandra Walker, Engagement Officer, IHME, email to GiveWell, July 21, 2021 (unpublished).
- 235
See this row in our cost-effectiveness analysis.
- 236
See this row in our cost-effectiveness analysis. This range includes DRC, Guinea, Nigeria (Global Fund and PMI states), Togo, and Uganda only (excluding Chad and South Sudan) for the reasons discussed in this section.
- 237
See this section in our cost-effectiveness analysis for estimates of the number of malaria deaths for people age five and over in the countries in our analysis. This data is drawn from IHME’s Global Burden of Disease project.
- 238
See this row in our cost-effectiveness analysis.
- 239
In 2017, GiveWell spoke to malaria researchers who told us that this topic is not well studied. It may be impractical and expensive to collect large enough sample sizes to detect a statistically significant effect of nets on 5-and-over mortality, among other challenges. Our findings are available at a separate page. We have not conducted any additional investigation into this topic since 2017.
- “Malaria mortality in adults has not been closely studied via empirical research. This is likely because adult malaria mortality is difficult to measure in resource-poor settings. Adults in these settings may die of malaria without entering health systems. Post-mortems will not always be performed to determine causes of death. Although there is not substantial empirical evidence, it is reasonable to expect that ITNs will avert some adult mortality. Nets will likely be less effective at averting adult deaths in high transmission areas, since adults in high transmission areas typically have high levels of malaria immunity.” GiveWell's non-verbatim summary of a conversation with Immo Kleinschmidt on May 25, 2017.
- “GiveWell: We have been unable to find much empirical research the impact of ITNs on adult malaria mortality. Is there substantial research that we have not seen, and why do you think we have not been able to find more research?
Dr. Churcher: It is true that there are not many clear estimates on these issues. This is largely because the complex nature of immunity makes impacts on adult malaria mortality very hard to estimate. Young children will have fairly similar responses to an anti-malaria intervention because they have not yet developed immunity. Adults are much more variable: in high transmission areas almost all have considerable immunity, which reduces the chance that a case of malaria will result in death.” GiveWell's non-verbatim summary of a conversation with Thomas Churcher and Hilary Ranson on May 31, 2017.
- 240
GiveWell asked Dr Thomas Churcher and Professor Hilary Ranson about sleeping patterns in our conversation in 2017. We heard: “We investigated mosquito biting times and the times people are under a bed net, and generally did not find large differences between adults and children, though it did vary substantially from site to site.” We include it in our adjustment nonetheless because we believe the mechanism is plausible and because of the shortage of empirical evidence on this topic. GiveWell's non-verbatim summary of a conversation with Thomas Churcher and Hilary Ranson on May 31, 2017.
- 241
As above, GiveWell asked Dr Thomas Churcher and Professor Hilary Ranson about net usage in our conversation in 2017. We heard: “Bed net usage rates among adults are quite good overall; they mostly share a sleeping place with young children. Again, there is very little research out there and quite a lot of variability. For example, one study found the lowest usage is often among teenagers as, unlike young children, adolescents often don’t share sleeping spaces with their parents.” GiveWell's non-verbatim summary of a conversation with Thomas Churcher and Hilary Ranson on May 31, 2017.
- 242
GiveWell has spoken to a number of malaria researchers on this topic, all of whom agreed that the community-level effect of ITNs is likely to be a significant component of their effect. However, none believe that this effect has been conclusively demonstrated or well-quantified.
“The argument for ITNs has always been that ITN coverage is a public good. Some of the good accomplished is not internalized to the person using the net. Some people argue that there's a negative externality as well - unprotected people are getting bitten by the mosquitoes that would have bitten the protected people - but I don't think you can make that argument with ITNs … What I do is analysis of data using mathematical models. In general, the leading models say that the more people use the nets, the bigger the positive externalities are … If you're talking about the marginal dollar for more nets, there's a lot more uncertainty on the cost-effectiveness of that than we'd like. The only data that we have is bad data. Improved surveillance would be helpful." GiveWell's non-verbatim summary of a conversation with Dave Smith on November 4, 2011.
For a detailed discussion from a previous version of this report, see here. - 243
Note: We summarize additional evidence on the impact of ITNs on older children and adult mortality on a separate page. This was published in 2017 and certain references may be out of date, but our overall reasoning has not changed—as of 2023, we have not done more work on this topic since publishing that page.
- 244
This excludes our supplemental adjustments discussed in sections 4.5 and 4.6.
- 245
See this row in our cost-effectiveness analysis. This range includes DRC, Guinea, Nigeria (Global Fund and PMI states), Togo, and Uganda only (excluding Chad and South Sudan) for the reasons discussed in this section.
- 246
For ease of modeling, we quantify our uncertainty ranges for benefits other than mortalities averted among people under age 5 as percentage adjustments applied to other modeled benefits of the program. For Uganda:
- Our 25th to 75th percentile range for income effects is a +24% adjustment to a +73% adjustment (to the total modeled benefits of the program). See this row in the “Sensitivity analysis” sheet of our cost-effectiveness analysis.
- This roughly translates to between 19% and 42% of the total modeled benefits of the program, as shown in the table above.
- This conversion is imperfect because varying the proportion of the program's total impact that is contributed by one type of benefit will also affect the proportion of impact contributed by other types of benefits, but we think the values presented in the table are a reasonably good approximation of our uncertainty level for this parameter.
- 247
For a list of symptoms of uncomplicated and severe malaria episodes, see CDC, "Disease - About Malaria"
- 248
See the table above for this cost-effectiveness range. For ease of modeling, we quantify our uncertainty ranges for benefits other than mortalities averted among people under age 5 as percentage adjustments applied to other modeled benefits of the program. For Uganda:
- In our model, an income effect of 0.3% to 0.9% implies a +24% adjustment to a +73% adjustment. See this row in the “Sensitivity analysis” sheet of our cost-effectiveness analysis.
- This implies a cost-effectiveness range of 13x - 18x (see this row).
- Note that the 0.3% to 0.9% range is intended to incorporate uncertainty not just around our main estimate of the effect of malaria on later life income, but other aspects of our calculations too (e.g. the duration of benefits). This should therefore be interpreted as a rough and illustrative summary of our uncertainty.
- 249
“Relative to non-malarious areas, cohorts born after eradication had higher income as adults than the preceding generation. These cross-cohort changes coincided with childhood exposure to the campaigns rather than to pre-existing trends. Estimates suggest a substantial, though not predominant, role for malaria in explaining cross-region differences in income.” Bleakley 2010, p. 1.
- 250
However, we have not deeply investigated the evidence on malaria incidence in the three remaining countries (Brazil, Colombia, and Mexico). It's possible that more research would lead us to believe that these estimates are more varied than they currently appear to be, which could update our estimate.
- 251
U.S. results for occupational income score and Duncan's index, Table 5, Bleakley 2010.
Note: Bleakley also presents instrumental variables estimates that give slightly higher results, but we use the OLS estimates for convenience because Bleakley selects these estimates and re-normalizes them by the difference between 95th and 5th percentile malaria intensity in his final outcomes analysis."The reduced-form differences are taken from Tables 1, 2, and 3, for the indicated outcomes. Reported are averages of the OLS point estimates, divided by the difference between 95th and 5th percentile malaria intensity." Notes to Table 5, Bleakley 2010.
Incorporating the instrumental variables estimates would not make much difference. In our rough calculations, Bleakley's IV specifications yield income effect estimates that are only ~10% higher than the OLS estimates. - 252
Bleakley presents an average of OLS results for two measures of U.S. malaria burden (proportion of mortality and an ecological index) that is normalized to the contextual malaria burden. "The reduced-form differences are taken from Tables 1, 2, and 3, for the indicated outcomes. Reported are averages of the OLS point estimates, divided by the difference between 95th and 5th percentile malaria intensity." Notes to Table 5, Bleakley 2010.
- 253
"For the United States, the base sample consists of native-born white males in the Integrated Public Use Micro Sample or IPUMS (Ruggles and Sobek, 1997) and North Atlantic Population Project (NAPP, 2004) datasets between the ages of 35 and 55, inclusive, for the census years 1880–2000, which includes cohorts with years of birth ranging from 1825 to 1965. I consider males rather than females because their labor-force participation is higher and more consistent across the wide swath of years." Data sources and definitions, Bleakley 2010.
- 254
"The human capital analyses draw on literacy and primary school attainment data, whereas the economic status analyses use household-level expenditure data.13 Past research has used earnings or occupational wage data to estimate the productivity effects of childhood malaria exposure (e.g., Bleakley 2010), under the implicit assumption that employers pay workers their marginal product. However, only 7 percent of the NSS sample has a nonzero wage, and three-quarters of workers aged 20–60 (68 percent of men, 78 percent of women) report one of two occupations (out of 463 in the classification), both agricultural. Given the unsuitability of the labor force data, we use the survey’s rich data on household consumption (including goods produced in the household) to measure the effects of eradication on economic status, measured by log household monthly per capita expenditure (measured in 1987 rupees). We trim the top and bottom 1 percent of the expenditure data to remove implausible values." Cutler et al. 2010, p. 81.
- 255
“We use the national malaria eradication program in India in the 1950s as a quasi experiment and exploit geographic variation in malaria prevalence prior to the eradication campaign. We compare gains for cohorts born before and after the program in areas with varying pre-eradication prevalence. These differences-in-differences estimates show no gains in literacy or primary school completion between areas that experienced large reductions in malaria and those that experienced small reductions in malaria. We do, however, observe modest relative increases in economic status (proxied by household per capita household expenditure) for prime age men. This effect is robust to using localized sources of geographic variation and to instrumenting for pre-eradication prevalence using geographic and climate factors, although in our most demanding specification (identified using within-region variation and including district linear trends) the point estimates remain similar but become imprecise. We do not observe significant increases in expenditure as a result of the program for women, and these gender differences cannot be explained by differences in the household composition of treated men and treated women.” Cutler et al. 2010, p. 73.
- 256
- "The rescaled OLS and IV point estimates indicate that a 10 percentage point decrease in incidence raises per-capita expenditure of between 1.5 and 6.8 percent. For women’s human capital, the OLS results do not imply positive treatment effects. However, the rescaled IV estimates imply that a 10 percentage point decrease in incidence increases female primary school attainment and literacy by 2.5 to 5.6 percentage points, with the most demanding specification (column 7 of Table 4) yielding estimates at the bottom of this range." Cutler et al. 2010, p. 92.
- "We use data on human capital attainment and economic status from the forty third round of the Indian National Sample Survey (NSS) conducted in 1987. The NSS is an all-India representative household consumer expenditure survey run by the Government of India starting in 1950. The NSS has four “thick” rounds that have the largest samples: namely, 1983, 1987, 1993, and 1999. We use the forty-third round (1987) because it is the earliest thick round that contains district identifiers." Cutler et al. 2010, p. 81.
- Economic status results are shown in terms of log per capita household expenditure for individuals aged 20-60. Cutler et al. 2010, Table 3, p. 85.
- 257
The instrumental variables results are generally larger than OLS. See Cutler et al. 2010, Tables 3, 4, and 5, pp. 85-86, 90. The authors do not choose a preferred specification but rather interpret the results as a range. We have not done a deep dive into the assumptions behind this range of results to see if we should prefer a certain specification. Without further investigation, we think taking the midpoint is the most reasonable interpretation.
- 258
- “The NMCP’s main operational activity was to conduct two annual rounds of DDT spraying of human dwellings and cattle sheds. By 1956, 112 million people were estimated to be protected (NMEP 1986). In 1958, the program was reformulated as the NMEP with the goal of completely eradicating malaria from the nation, and by 1960–1961, the entire country was brought under the program (Web Appendix Table 1).” Cutler et al. 2010, p. 75.
- “The Rockefeller Foundation, having mounted a successful campaign against hookworm in the early 1910s, also funded antimalarial work later in the decade through its International Health Board (IHB). These two groups sponsored demonstration projects in a number of small, rural towns across the South. They employed a variety of new methods (spraying of larvacides, water management, window screening, and mass administration of quinine) and most of these demonstrations were highly successful, resulting in 70% declines in morbidity (i.e., sickness that does not result in mortality).
The federal government’s large-scale efforts against malaria in the South began with World War I (WWI). In previous wars, a significant portion of the troops were made unfit for service because of disease contracted in or around encampments. The PHS, working now with both a strong knowledge base on malaria control and greatly increased funding, undertook drainage and larviciding operations in Southern military camps as well as in surrounding areas. After the War, the IHB and PHS expanded the demonstration work further. By the mid-1920s, the boards of health of each state, following the IHB/PHS model, had taken up the mantle of the malaria control in all but the most peripheral areas of the region (Williams, 1951)...
The World Health Organization (WHO) proposed in the early 1950s a worldwide campaign to eradicate malaria. While the WHO mostly provided technical assistance and moral suasion, substantial funding came from USAID and UNICEF. The nations of Latin America took up this task in the 1950s. While individual nations had formal control of the design and implementation of the programs, their activities were comparatively homogeneous as per the dictates of their international funders. The central component of these programs was the spraying of DDT, principally in the walls of houses. Its purpose was not to kill every mosquito in the land, but rather to interrupt the transmission of malaria for long enough that the existing stock of parasites would die out. After that, the campaigns would go into a maintenance phase in which imported cases of malaria were to be managed medically.” Bleakley 2010, pp. 4-6.
- 259
We think that major economics journals would be less likely to publish studies finding that there was no impact of malaria eradication on economic outcomes. Relying only on these two studies could mean we are systematically overestimating long-term income effects in our analysis.
- 260
“I focus on US whites for several reasons. First, a only small proportion of blacks lived outside of the most malarious states among the earlier cohorts, which means that they make for an imprecisely measured point of comparison. Second and more importantly, that same population of blacks was less likely to have been enslaved, which means that they make for an inappropriate control group for those blacks born into slavery in the malarious South. The estimates reported below (for whites) are similar to those obtained if I include native blacks in the base sample. Estimates using blacks only, however, are imprecise and sensitive to control sets employed. Race was not measured consistently in the Latin America sample, so I work with native males of any race/ethnicity.” Bleakley 2010, p. 8.
- 261
“Notably, we do not observe significant effects of the program on per capita household expenditure for treated women (panel B). The coefficients on post × malaria index are significantly higher for men in all specifications other than the one with district linear trends.” Cutler et al. 2010, p. 86.
- 262
“We do not observe significant increases in expenditure as a result of the program for women, and these gender differences cannot be explained by differences in the household composition of treated men and treated women. In most, but not all, of our specifications, the gender differences are statistically significant. This suggests that improved labor market productivity may underlie the observed effects for men, given their much higher rates of labor force participation…
…Men’s labor force participation rates are well over 90 percent for most of this age interval, while women’s labor force participation rates never rise above 50 percent. Therefore, we focus our attention on men in this age group…” Cutler et al. 2010, pp. 73-74, 81. - 263
“I consider males rather than females because their labor-force participation is higher and more consistent across the wide swath of years.” Bleakley 2010, p. 9.
- 264
Specific examples include:
- Cutler et al. uses a physical map of malaria endemicity by district as its data source for pre-eradication malaria burden. The authors state that the map is based on spleen rate surveys (enlarged spleens are a common symptom of malaria) and climatic factors, but that the “the exact mechanism by which category boundaries were constructed is not known.” They validate the map by correlating pre-eradication endemicity categories by state with measures of the child spleen rate in each state. (Cutler et al. 2010 pp. 78-79).
- Bleakley uses an index of pre-eradication malaria endemicity for each country. While we have not vetted this index in detail, our understanding is that the categories are based in part on expert opinion. We think it is unlikely that estimates from the study period (1920s - 1950s) had accurate methods for measuring malaria prevalence, like modern microscopy or biomarker testing to verify parasitemia. Our best guess is therefore that the index is composed of extremely rough estimates.
- “What was the range of pre-eradication malaria infection within each country? Molineaux (1988) reports on the WHO typology of malaria intensity (and associated malaria-infection rates among children): non-endemic (0%), hypoendemic (0–10%), mesoendemic (10–50%), hyperendemic (50–75%), and holoendemic (75–100%). Molineaux also reports estimates of the spatial distribution of different endemic zones throughout the world. (Both the typology and its associated geography are derived from the experience of many experts and do not simply reflect the opinion of that one author, however.) Taking the midpoint of the reported intervals, information about the types of endemicity within each country is used to estimate the cross-area differences in malaria burden prior to the campaigns. The pre-eradication malaria burden in the US ranged from malaria free to mesoendemic, representing a within-country difference in malaria-infection rates of approximately 0.3. Areas within each of the three Latin American countries varied from essentially zero to hyperendemic, for a range of 0.625 in infection probability.” Bleakley 2010, p. 18.
- 265
“How realistic is the assumption that areas with high infection rates benefited more from the eradication campaign? Mortality and morbidity data indicate drops of 50 to 80 percent in the decade after the advent of the eradication efforts. Such a dramatic drop in the region’s average infection rate, barring a drastic reversal in the pattern of malaria incidence across the region, would have had the hypothesized effect of reducing infection rates more in highly infected areas than in areas with moderate infection rates. Data on malaria cases by Colombian departments allow us to examine this directly. The decline in malaria incidence as a function of intensity prior to the eradication campaign is found in panel B of Figure 1. The basic assumption of the present study, that areas where malaria was highly endemic saw a greater drop in infection than areas with low infection rates, is borne out. (Similar results are seen for US and Mexican states. Data for Brazilian states were not available.)
Finally, the timing of the eradication campaign should induce variation in childhood malaria infection that has a marked pattern across year-of-birth cohorts. The present study considers the effects of childhood malaria infection on later-life outcomes, so it is useful to characterize childhood exposure to an eradication campaign. This is shown in Figure 2. Consider a campaign that starts in year zero and takes effect instantaneously. Cohorts born after this date will be exposed to the campaign for their entire childhood. On the other hand, those cohorts who were already adults in year zero will have no childhood exposure to the campaign, while the “in-between” cohorts will be partially exposed during childhood, as shown in Figure 2. I exploit this timing in two ways. First, in Section III, I compare the “born after” cohorts to the “already adult” cohorts by taking differences across these cohort groups. Second, in Section IV, I use the functional form of childhood exposure in estimation using data for all cohorts. (I discuss some alternative functional forms in Section IV.B.)These four factors (the external origin of the campaigns, the quick reduction of malaria that followed, the use of nonmalarious areas for comparison, and the differential incidence of eradication benefits across cohorts) combine to form the research design of the present study." Bleakley 2010, pp. 8-9.
“The resulting measures of pre-eradication malaria endemicity are strongly correlated with the sequelae and ecological determinants of malaria. Figure 3 plots the state-level child spleen rate against our map-based, state-level malaria index, constructed in the same way as the district-level index. In 1953–1954, just as the NMEP was starting its operations, the child spleen rate was strongly positively associated with the malaria index. By 1959–1960, as the eradication program was nearing completion, states converge to very low child spleen rates, so that states with high pre-eradication levels of malaria experienced the largest reductions in malaria over the eradication era. The district malaria index is also associated with known ecological determinants of malaria endemicity (precipitation, humidity, elevation, and temperature) in the expected directions (Web Appendix Table 4).” Cutler et al. 2010, p. 80.
- 266
“I reviewed the Bleakley study and mostly support its key findings: the campaigns to eradicate malaria from Brazil, Colombia, and Mexico, and perhaps the American South as well, were followed by accelerated income gains for people whose childhood exposure to the disease was reduced. The timing of these events is compatible with the theory that rolling back malaria increased prosperity.” Roodman, "Revisiting the evidence on malaria eradication in the Americas," 2017
- 267
The 36% incidence reduction in Bleakley is large, reflecting the malaria rate in the county with the highest incidence in the historical U.S. rather than average incidence. Bleakley's results are scaled to compare income changes in counties with the highest vs. lowest malaria incidence, so it makes sense to scale its results using the maximum incidence rate.
- 268
To set these values, we compared reference values including (i) historical malaria indicators from the Bleakley historical U.S. setting; (ii) historical malaria indicators from the Cutler historical India setting; and (iii) modern-day IHME incidence data by age groups for various regions of the world. We assume that the malaria rate for under-5 children is 2x the population rate. Reference values for this age ratio span 0.6-2.9:
- Historical data from the Cutler and Bleakley settings are imperfect but suggest that a high ratio makes sense.
- The ratio for modern-day sub-Saharan Africa (SSA) is 2.6.
- The malaria transmission patterns in Cutler/Bleakley settings are probably a little more moderate than in SSA, suggesting that it's about right to set the Cutler/Bleakley age ratio a little below the current value for SSA.
- We assume the malaria rate for children ages 5-14 is the same as the population rate. Reference values for this age range span 0.75 to 1.1, where the highest value is in sub-Saharan Africa, and similar to above, we use an input a little below SSA.
- 269
See this row in our supplementary analysis.
- 270
See these rows in our supplementary analysis.
- 271
See this section of the report. Our understanding (although we haven’t investigated this in depth) is that this is because nets reduce but don't eliminate malaria exposure. This implies many people will still be exposed to malaria (but may not develop a clinical case due to previous immunity). Nets also don't help post-incident case infections to clear any faster.
- 272
In modern studies, malaria prevalence is generally measured by collecting blood samples and testing them for malaria parasites using microscopy or diagnostic tests. It's unlikely that early and mid-20th century sources had access to such tests that would allow them to detect asymptomatic malaria parasitemia.
- 273This understanding is based on an unpublished conversation with a malaria expert.
- 274
Elsewhere in our analysis, we assume that malaria indirectly causes 0.75 deaths (e.g., by making people susceptible to other infectious diseases) for every direct malaria death.
If we assume that morbidity averted correlates with deaths averted, and roughly assume that half of indirect deaths come from complications immediately following malaria cases and are correlated with prevalence, this leaves us with a 20% share of morbidity from long-run malaria prevalence (50% x 0.75 / 1.75).
- 275
An incidence rate of >100% implies that there is more than one malaria case per child over the course of a calendar year.
- 276
See these rows in our cost-effectiveness analysis.
- 277
See our justification for the equivalent parameter in our deworming cost-effectiveness analysis here.
- 278
Bleakley 2010 evaluates long-term economic outcomes at ages 35-55, and Cutler et al. 2010 evaluates outcomes at ages 20-60.
- 279
See this section of our accompanying benchmarking spreadsheet. The benchmarks are based on extrapolating from our estimates in this section.
- 280
- Malaria incidence for all ages in the WHO African Region has fallen from 373 to 229 cases per 1,000 person years between 2000 and 2021. WHO, World Malaria Report 2022, Fig. 3.3 (a), p. 19.
- We adjust for the higher average malaria burden in children using the GBD 2019 estimate that children ages 0-14 have a malaria incidence rate that's 165% of the general population's. 14% x 1.65 ≅ 25%. This incidence rate is equivalent to 0.25 cases per person aged 0-14 per year.
- 281
- We assume that children can experience long-term income increases from averting malaria for 15 years in childhood. 15 years x 0.25 malaria cases averted per year x 0.6% income increase per case averted = 2.25% income increase.
- This is an upper bound for the income effect because (i) malaria incidence has been steadily decreasing since 2000, so decreases in childhood malaria incidence for working-age adults today lie somewhere in between the 2000 and 2021 incidence rates; and (ii) there's only been 15-20 years since malaria interventions greatly scaled up, so most working-age adults today have <15 years of childhood exposure to lower malaria burden.
- 282
The World Bank estimates that GDP per capita PPP in sub-Saharan Africa increased from $2,105 in 2000 to $4,070 in 2021. World Bank Open Data, GDP per capita, PPP - Sub-Saharan Africa
- 283
For example:
- Gallup & Sachs (2001) finds that a 10% reduction in a malaria index was associated with 0.3% higher growth → ~1.2% GDP per capita increase for a 40% reduction in Africa's malaria burden.
- Okorosobo et al. (2011) estimates "GDP penalties" from malaria ranging from 0.4% to 8.9% in Chad, Ghana, Nigeria, Uganda.
There are multiple caveats with this comparison:
- These macro papers report a wide range of estimates.
- This is non-causal cross-country evidence based on differences in malaria burden over space.
- We haven't dug into these papers and their evidence quality or done a thorough literature review for macro evidence.
- 284
See these rows in our cost-effectiveness analysis for each program:
- 285
This CDC fact sheet lists symptoms of uncomplicated and severe malaria episodes. Severe symptoms include fever, anemia, enlarged liver or spleen, kidney injury, and severe neurological symptoms associated with cerebral malaria.
- 286
This is because the people whose deaths were averted would be disproportionately low-earning.
- 287
- “P. falciparum is the most prevalent malaria parasite on the African continent. It is responsible for most malaria-related deaths globally. P. vivax is the dominant malaria parasite in most countries outside of sub-Saharan Africa.” WHO, "Malaria," 2023
- “For instance, in the absence of an offsetting fertility response, eradication of the more fatal P. falciparum in sub Saharan Africa is more likely to result in population growth. As a result, effects on cohorts exposed to eradication in childhood may differ in general equilibrium.” Cutler et al. 2010, p. 92.
- “However, the expected difference in the impact of malaria eradication for P. falciparum versus P. vivax is also theoretically ambiguous. It is uncertain, a priori, whether the larger mortality impact of P. falciparum eradication would tend to increase or decrease incentives to education because this depends both on the extent and magnitude of mortality selection from child and adult mortality. Reduced child mortality would tend to increase the magnitude of mortality selection and reduce years of schooling, in addition to raising population growth and potentially overwhelming school systems, lowering educational outcomes in general equilibrium. However, by extending the time over which returns to human-capital investments can be realized, averted adult mortality would tend to raise incentives for schooling.” Barofsky 2011, p. 20.
- 288
This is either because we think they would be challenging to model effectively, or because their likely effect is small enough that we do not expect explicit modeling to be worth the time investment required.
- 289
See this row in our cost-effectiveness analysis. This range includes DRC, Guinea, Nigeria (Global Fund and PMI states), Togo, and Uganda only (excluding Chad and South Sudan) for the reasons discussed in this section.
- 290
- Step one: Estimate the likely size of each effect (a rough subjective best guess).
- Step two: Evaluate each effect using three criteria, each assigned a score of up to 3:
- Can it be objectively justified (i.e., is there direct evidence for the effect)? (Where 0 is little evidence and 3 is strong direct evidence).
- How easy would it be to model? (Where 0 is impossible and 3 is simple).
- Consistency – is this effect included in our cost-effectiveness analysis for other programs? (Where 1 is no, 2 is partially and 3 is yes).
- Step three: Convert the total three criteria score out of 9 into a percentage (e.g., a total score of 5 converts to a percentage of 50%).
- Step four: Weight our estimate of each effect by this percentage to produce our overall adjustment (e.g., an effect size guess of 15% multiplied by a three criteria score of 60% = an adjustment of 9% (15% x 60% = 9%)).
We use the method described for all supplemental intervention-level adjustments in our cost-effectiveness analysis for ITNs, with the exception of:
- Our estimate of costs saved from averted malaria. We account for these savings using an explicit model, discussed in more detail here.
- The adjustment for marginal funding going to lower priority areas, which we estimate case-by-case for each country based on our understanding of how the National Malaria Program is likely to prioritize funding.
- 291
See this section of our cost-effectiveness analysis.
- 292
“Cerebral malaria is the most severe neurological complication of infection with Plasmodium falciparum. With over 575,000 cases annually, children in sub-Saharan Africa are the most affected. Surviving patients have an increased risk of neurological and cognitive deficits, behavioral difficulties and epilepsy making cerebral malaria a leading cause of childhood neuro-disability in the region. The pathogenesis of neuro-cognitive sequelae is poorly understood: coma develops through multiple mechanisms and there may be several mechanisms of brain injury.”
Idro et al. 2010, pp. 267-274. - 293
Rough calculations underlying our estimate are available here. These estimate the years lost to disability (YLDs) as a proportion of the overall malaria disease burden, measured in DALYs (disability-adjusted life years).
- 294
- “The best estimates of the causal contribution of malaria to anaemia in a particular setting come from randomized trials of malaria control interventions. A review of 29 community-based studies of insecticide-treated nets (ITNs), anti-malarial chemoprophylaxis, and insecticide residual spraying found that among children < 5 years exposed to between 1 and 2 years of malaria control, mean relative risk for a haemoglobin concentration < 11 g/dL was 0.73 (95% CI 0.64–0.81), and for a haemoglobin < 8 g/dL was 0.40 (95% CI 0.25–0.55) compared with the control groups not exposed to these malaria interventions.” White 2018, p. 371.
- The Pryce et al. meta-analysis we use to estimate the impact of ITNs on mortality also finds an effect of ITN distribution on hemoglobin levels (which determine anemia):
“Five trials reported the mean haemoglobin in ITN and no-nets arms. Pooled analysis of the trials showed that ITNs were associated with a mean difference of a 1.29 increase in percentage PCV (95% CI 0.42 to 2.16; 5 trials, 11,489 participants, Analysis 1.9).” Pryce et al. 2018, p. 16.
- 295
Note that reduced anemia is one of the proposed mechanisms for malaria income effects, which we model separately. This adjustment is intended to capture the shorter-term benefits of averted anemia separately from its possible role in income effects.
- 296
See this row in our cost-effectiveness analysis.
- 297
As of December 2023, these are AMF, Malaria Consortium, Helen Keller International (HKI), and New Incentives. See our "Top charities" page here.
- 298
Our model estimates a 14% upwards adjustment for ITNs (here), a 20% upwards adjustment for seasonal malaria chemoprevention (here) and a 21% upwards adjustment for vitamin A supplementation (here).
- 299
We use state-level data on malaria burden for Nigeria. See this section in our cost-effectiveness analysis.
- 300
See here for further discussion of our reasoning.
- 301
Discussed further in this section of the report.
- 302
From our 2019 report on insecticide resistance: "I did not find evidence that substantial mosquito insecticide resistance existed in the trials that underlie our estimate of ITN effectiveness (with the exception of one trial that carries little weight), however the majority of outcome weight is represented by two trials that I was unable to find resistance data on." GiveWell, Insecticide resistance adjustment analysis, 2019, p. 2.
- 303
We have decided not to explicitly model this impact because (i) we would have to make very uncertain assumptions about trials with missing information on insecticide resistance, and (ii) we believe insecticide resistance would probably have a small impact on overall cost-effectiveness. That is in part because adjusting for this variable would have opposite impacts on our estimate of ITN effectiveness and our insecticide resistance adjustment, partially canceling itself out.
- 304
See this row in our cost-effectiveness analysis. This range includes DRC, Guinea, Nigeria (Global Fund and PMI states), Togo, and Uganda only (excluding Chad and South Sudan) for the reasons discussed in this section.
- 305
We use a lower value of 5% for DRC and Nigeria, based on our understanding (discussed above) that these countries will extend the interval between campaigns in different states rather than focus on higher prevalence areas. We use a value of 0% for Chad, because our analysis in Chad uses a weighted average of subnational-level data on mortality rates and malaria prevalence and so this additional adjustment is not needed.
For more detail on our reasoning by country, see this entry in our CEA change log (for Nigeria and DRC). Our calculations for Chad are available here. - 306
“From 1995 onwards, coinciding with the results from the main African ITN trials, a vigorous debate arose about the possibility that the short-term mortality improvements observed in trials of 1–2 years' duration could be offset by increased mortality at older ages — a "delayed mortality" effect. The underlying hypothesis was that immunity to malaria would develop more slowly under reduced transmission, leading to a longer period of susceptibility. No direct evidence was available at the time either to support or to refute this hypothesis.”
Lengeler 2004b, p.84. - 307
A 2010 paper (Kilian et al. 2010, p. 2) claims that this question has been "answered, with a clear indication that even seven years after initial exposure of infants to ITN, no increased mortality could be observed" and cites three sources: Binka et al. 2002, Diallo et al. 2004, and Lindblade et al. 2004.
All of these appear to be follow-ups on the small-scale, high-quality studies that originally established the impact of ITNs on child mortality (see this section), and all conclude that reductions in child mortality were sustained in the several years after the initial study. These follow-ups account for three of the five studies that originally established an impact of ITNs on child mortality in Lengeler 2004a.We previously emailed the authors of all five studies to ask whether there have been any follow-ups beyond the latest we're aware of; in four of five cases, it's been confirmed that no more follow-ups were done, and in the fifth case we have not heard back. A more recent trial, Louis et al. 2012, measured mortality over a median follow-up time of about eight years in children individually randomized to either receive ITNs at birth or at 6 months of age. In line with the follow-ups, the study concluded that ITN protection in early infancy does not increase mortality later in life.
We attempted to vet the conclusions of one of the follow-ups (Binka et al. 2002), but we found the study difficult to interpret based on the information provided in the paper and our vet was inconclusive:- Binka et al. 2002 reported “no indication in any age group of increased mortality in the ITN group after the end of the randomized intervention.” (p. 597)
- The authors seem to have reached this conclusion based on judging the mortality rate differences in the follow-up period as minimal. “There was no indication in any group that the benefits of reducing malaria exposure for the 2- year period of the trial were lost during the subsequent follow-up period. In particular, in the age group 6-11 months of age at baseline, the cohort analysis found a significant protective efficacy during the 2-year period of the trial (confidence interval not overlapping with 0, see Table) but there was minimal difference between the control and ITN groups in mortality in this age group during the subsequent [5.5] years of follow-up (Table).” Binka et al. 2002, p. 597
- However, the mortality rate differences in the follow-up period do not strike us as small enough to demonstrate that mortality did not increase at older ages. Instead, the study seems to provide weak evidence of an increase in mortality at older ages.
- For children less than two years old at the start of the trial (the cohort in which mortality declined in the trial period), we calculate a difference in deaths per 1,000 people of -16.4 (95% CI: -28.4 to -4.6) over the trial period and 5.4 (95% CI: -4.6 to 15.3) over the follow-up period (these calculations probably underestimate the width of the confidence intervals, because we did not account for clustering). See our Calculations for Binka et al. 2002.
- It still seems possible that this increase did not offset earlier reductions in mortality by much, but we could not calculate a confidence interval for this offset from the information provided in the paper, so we do not know if the study had sufficient statistical power to reject the hypothesis with high confidence that delayed mortality offset earlier reductions in mortality by some non-negligible amount.
- Binka et al. 2002 reported “no indication in any age group of increased mortality in the ITN group after the end of the randomized intervention.” (p. 597)
- 308
WHO, Technical consultation on the malaria rebound phenomenon, 2022.
- 309
Discussed here in this report.
- 310
See our full report here. "The mosquito species distribution represented in our model does not perfectly reflect the species distribution in our areas of interest for ITN distributions. Since different species tend to exhibit different levels of pyrethroid resistance and different responses to the pyrethroid synergist PBO, this could lead to inaccuracy in our insecticide resistance adjustment." GiveWell, Insecticide resistance adjustment analysis, 2019, p. 2.
- 311
We have opted not to explicitly model this effect because we believe it would be complex to model and we are unsure how accurate the resulting model would be because we have little confidence in the representativeness of the data that underlie the apparent differences in insecticide resistance between species.
- 312
These may be distinct from its potential long-term economic benefits (which we would expect to operate via changes in child development).
- 313
Although the study found a large productivity effect (an increase in the average annual harvest value for a farmer by $76, about 15% of average annual harvest value at baseline), baseline imbalance between the treatment and control groups in the outcome of interest poses a major threat to the study’s validity. We are therefore hesitant to put any weight on this finding.
The study found that free ITNs increased the average annual harvest value by $76 (about 12% of the group’s average annual harvest value at baseline). Fink and Masiye 2015, Table 1, “Total harvest value 2009 (US$),” “Free nets”: 613.8. 76/613.8 = ~12%.
- Note that the paper’s abstract reports a 14.7% increase. Presumably, the 14.7% corresponds to the increase in harvest value as a proportion of the average annual harvest value in the group receiving free ITNs at endline, but we’re not sure. "The point estimates from our preferred specification suggest that the returns to bed nets in the study sample were large: on average, we find that access to free bed nets (three nets for a typical household) increased agricultural output by US$ 76, which corresponds to 14.7% of the average annual harvest value." Fink and Masiye 2015, p. 152.
Presumably, the 14.7% corresponds to the increase in harvest value as a proportion of the average annual harvest value in the group receiving free ITNs at endline, but we’re not sure. "The point estimates from our preferred specification suggest that the returns to bed nets in the study sample were large: on average, we find that access to free bed nets (three nets for a typical household) increased agricultural output by US$ 76, which corresponds to 14.7% of the average annual harvest value." Fink and Masiye 2015, p. 152.
Baseline imbalance between groups: “In order to facilitate a rapid distribution of bed nets, treatments were randomly assigned at the cluster level prior to the collection of baseline data in the experiment. The non-stratified cluster-level randomization resulted in a rather unbalanced sample, with treated farmers on average both larger and more productive than farmers in the control group. To address these imbalances, we focus on analyzing changes in production outcomes between the 2009 (pre- intervention) and the 2010 (post-intervention) farming seasons.” Fink and Masiye 2015, p. 152
- 314
"This cluster randomized trial evaluates the economic impact of a private sector malaria control program. In collaboration with 81,597 smallholder contract farmers in 1,507 clusters, I investigate whether the distribution of free insecticide-treated mosquito nets at the outset of malaria season increased cotton output sufficiently to be commercially viable for the implementing agribusiness. But despite large health effects in farming households, I do not detect any impact on deliveries to the agribusiness. I conclude that the independent and sustained distribution of free mosquito nets by Zambia’s cotton industry is unlikely to materialize without subsidies. The results can be partially reconciled with previous research on the labor decisions of smallholder farmers, and tend to side with the minority of the observational literature that questions the role of malaria as a central and immediate cause of poverty." Sedlmayr 2014, p. 1.
- 315
Our estimates are of household income lost directly or indirectly to malaria. This includes people needing to take more time off work as a result of malaria cases. See these rows in our cost of illness averted analysis for further details.
- 316
“Results: In aggregate, malaria infections, spleen rates, haemoglobin concentrations, and weight for height, did not differ significantly during the study period between villages with and without ITNs, with a weighted mean
difference of −2.6 P. falciparum episodes per 1,000 weeks at risk (95% Confidence Interval −7 to 1.8). In areas with a higher incidence of malaria there was some evidence ITN protective efficacy. The economic analysis indicated that, despite the uncertainty and variability in their protective efficacy in the different study sites, ITN could still be cost-effective, but not if they displaced funding for early diagnosis and effective treatment which is substantially more cost-effective.Conclusion: In Western Myanmar deployment of ITNs did not provide consistent protection against malaria in
children living in malaria endemic villages. Early diagnosis and effective treatment is a more cost effective malaria
control strategy than deployment of ITNs in this area where the main vector bites early in the evening, often before people are protected by an ITN.” Smithuis et al. 2013, p. 1. - 317
For a summary of fertility rates by country, see Our World in Data, "Fertility rate: children per woman, 2021"
- 318
"The impact of life-saving interventions on fertility and population growth varies by context, and is rarely greater than 1:1. In places where lifetime births/woman has been converging to 2 or lower, saving one child’s life should lead parents to avert a birth they would otherwise have. The impact of mortality drops on fertility will be nearly 1:1, so population growth will hardly change. In the increasingly exceptional locales where couples appear not to limit fertility much, such as Niger and Mali, the impact of saving a life on total births will be smaller, and may come about mainly through the biological channel of lactational amenorrhea. Here, mortality-drop fertility-drop ratios of 1:0.5 and 1:0.33 appear more plausible." Roodman 2014
- 319
- Egrot et al. 2014 conducted interviews about ITN-related fires in a district in Benin and conducted a literature search for ITN-related fires. The study found reports of bed net related fires in several countries, including some resulting in bodily harm or death.
- "Methods: This anthropological study is based on an inductive qualitative approach, including 91 semi-structured interviews conducted from July 2011 to March 2012 in a health district in Southern Benin.
Results: Fifty-six persons stated that bed nets can catch on fire but do not always refer to specific facts. However, 34 of the 56 people narrate specific events they heard or experienced. 39 accounts were geographically located and situated in time, with various details. In 27 situations, people were burned, for which 12 people reportedly died.
Discussion: The disparity between these results and the dearth of bibliographic documentation in the initial search prompted a more in-depth literature review: 16 contributions between 1994 and 2013 were found. Bed net fires were noted in 10 countries, but it is impossible to ascertain the frequency of such events. Moreover, bodily harm can be significant, and several cases of death attributed to bed net fires were noted." Egrot et al. 2014, p. 1.
- Kalanzi et al. 2014 examined admissions for bed net related burns to a national referral hospital in Kampala, Uganda. The study found 45 patients admitted to the burns unit with bed net related burns from 2008 to 2011. 15 of the 45 patients died.
“Methods: Data were collected from burns unit admission records at Mulago National Referral Hospital in Kampala, Uganda for the years 2008–2011 inclusive. Retrospective analyses on the characteristics of patients admitted with bed net related burns within this period were conducted.
Results: A total of 45 patients were admitted to the burns unit with bed net related burns during the study period. Most burns occurred among individuals who were 0–1 years old (33.3%) and 26–35 years old (24.2%) and the majority were male (71%). Bed net related burns at Mulago Hospital are severe, as evidenced by the fact that 15 of 45 patients died (crude mortality rate = 33%) and that 26 patients (57.8%) had total body surface area burn percentages that were greater than 20%. The average length of stay in hospital for patients with bed net related burns was 30.4 days." Kalanzi et al. 2014, p. 495. - Egrot et al. 2014 conducted interviews about ITN-related fires in a district in Benin and conducted a literature search for ITN-related fires. The study found reports of bed net related fires in several countries, including some resulting in bodily harm or death.
- 320
“Manufacturers’ delivery data show that, between 2004 and 2021, more than 2.5 billion ITNs were supplied globally, of which 2.2 billion (87%) were supplied to sub-Saharan Africa.” WHO, World Malaria Report 2022, p. 64.
- 321
The ITN distribution programs we have supported conduct monitoring surveys to determine whether recipients use nets as intended. Our largest grantee to date, Against Malaria Foundation, has generally found moderate-to-high usage rates (in the 60 to 80% range, depending on the country and length of time since the campaign). These results are broadly in line with evidence from other surveys; for more detail on the wider evidence on ITN usage, see our response to the New York Times article. For more detail about the usage monitoring data we have seen from distributions that GiveWell has funded, see our page on Against Malaria Foundation’s program.
- 322
We would expect fewer people to use nets if they needed to pay for them than if they were free. Because some portion of the protection provided by nets is a community-level effect from the overall number of mosquitoes in the environment being lower (see this section of the report), this could undermine their protective effect for a whole community (not just the individuals who don’t purchase them). We also note that the largest benefits of using ITNs accrue to children, who do not generally have the opportunity to decide for themselves whether or not to purchase nets. For more details on this topic, see this 2012 blog post.
- 323
The specific types of involvement we have seen have varied between different campaigns. For more details by campaign, see our Against Malaria Foundation supplementary information page. As an example, 22 senior district health staff were employed as Field Supervisors in Kasaï-Occidental Province in DRC as part of a 2014 distribution supported by Against Malaria Foundation.
"i) Field Supervisors (FSs)
22 FSs were selected from permanent and senior health staff in Tshikapa Health District.
ii) Community Health Workers (CHWs) – data collectors
Each of the 22 FSs had the responsibility of recruiting, in each HA they were designated, enough CHWs to gather household data and hang nets. Two primary recruitment criteria were literacy and familiarity with using a mobile phone. The number of CHWs recruited depended on the size of the HA and the number of households to be visited. The aim was to recruit enough CHWs to carry out the entire registration and hang‐up, once it commenced, in a five day period. Between 20 and 40 CHWs were recruited by each FS for a total of 4,000 CHWs across the 8 HZs (8 HZs x 20 HAs x 25 CHWs per HA = 4,000 CHWs)." AMF and IMA World Health, LLIN Distribution Report: West Kasai, Democratic Republic of Congo, p. 13.
- 324
See this section for more details.
- 325
“Core interventions for malaria vector control are applicable for all populations at risk of malaria in most epidemiological and ecological settings, namely: i) deployment of insecticide-treated nets (ITNs) that are prequalified by WHO, which in many settings are long-lasting insecticidal nets (LLINs); and ii) indoor residual spraying (IRS) with a product prequalified by WHO. Once high coverage with one core intervention has been achieved, supplementary interventions – namely the deployment of chemical or biological larvicides – can be used in addition to the core interventions in specific settings and circumstances.” WHO, Guidelines for Malaria Vector Control, 2019, p. xiv.
- 326
See this row of our cost-effectiveness analysis.
- 327
See this section of our cost-effectiveness analysis.
- 328
Note: our concerns also mean that we use the data from AMF’s monitoring in a relatively limited way as inputs into our cost-effectiveness analysis, and rely instead on other sources of information to evaluate net durability and usage. See this section of our report on AMF for further details.
- 329
Factors accounted for elsewhere:
- We consider whether goods are purchased but do not reach recipients. We do not adjust for this factor here because it is accounted for separately in our cost per net analysis. See this section of the report for more details.
- We consider "double treatment," i.e., whether people will not benefit from campaigns because they receive nets from other sources. We discuss how we account for this factor here.
- 330
See this row in our cost-effectiveness analysis. This range includes DRC, Guinea, Nigeria (Global Fund and PMI states), Togo, and Uganda only (excluding Chad and South Sudan) for the reasons discussed in this section.
- 331
We estimate that each $ donated to GiveDirectly’s direct cash transfer program generates 0.00335 units of value. 0.005 / 0.0035 = ~1.5.
- 332
We estimate that each $ donated to GiveDirectly’s direct cash transfer program generates 0.00335 units of value. 0.015 / 0.0035 = ~4.5.
- 333
See this row in our cost-effectiveness analysis. When rounded, this figure appears as 0%.
- 334
We estimate that each dollar spent by a domestic government in a malaria-endemic country generates 0.005 units of value, compared to 0.077 for AMF’s spending in Uganda. 0.005 / 0.077 = ~6%. For details of how we estimate this, see this section.
- 335
- We estimate that each $ spent by the Ugandan government generates 0.005 units of value if used for other activities.
- In total, we think the Ugandan government spends ~$47,000 in in-kind resources for every $1 million spent by AMF.
- This implies that shifting these resources away from other activities results in 236 units of value being lost. (~47,000 x 0.005) = 236.
See this row in our cost-effectiveness analysis.
- 336
See this row in our cost-effectiveness analysis.
- 337
142 / 76,545 = ~0.2%. See this row in our cost-effectiveness analysis.
- 338
See this row in our cost-effectiveness analysis. Our funging adjustments ranged from roughly -15% to -40% depending on the country. This range includes DRC, Guinea, Nigeria (Global Fund and PMI states), Togo, and Uganda only (excluding Chad and South Sudan) for the reasons discussed in this section.
- 339
We revisit these probabilities for each grant we make. For Uganda, we most recently estimated these probabilities as part of a 2021 grant (for campaigns taking place in Uganda in 2023). See our grant page here.
- 340
In this scenario, we do not think that AMF’s funding is causing more nets to be delivered, if other funders would have replaced its spending in any case.
- 341
This is based on an analysis of the value of the Global Fund’s spending. We estimate that the Global Fund’s spending on other activities generates 0.015 of value per $, compared to 0.077 units of value per $ for AMF’s spending in Uganda. 0.015 / 0.077 = ~19%. See this section for how we generate these estimates.
- 342
- We estimate that each $ spent by the Global Fund generates 0.015 units of value if used for other activities and AMF generates 0.077 units of value per $ spent on nets in Uganda.
- Per $1m, the Global Fund replacing AMF’s spending in Uganda would generate 92,846 units of value on nets ($1m x 0.077) and lose 15,433 units of value ($1m x 0.015) that would have been spent on other programs. 76,545 - 15,433 = 61,112.
See this row in our cost-effectiveness analysis.
- 343
See this row in our cost-effectiveness analysis.
- 344
24,445 / 76,545 = ~32%. See this row in our cost-effectiveness analysis.
- 345
The Global Fund pays for some of the distribution costs in the AMF-supported campaigns we have seen, and we incorporate these costs into our cost per net analysis (more discussion here).
We exclude these costs from our leverage and funging adjustments, because we think that AMF providing funding for a given campaign does not lead to the Global Fund contributing more funding to that campaign:
- In the campaigns we have seen, AMF covers the cost of purchasing nets and other partners cover most of the distribution costs.
- The way this process works is that AMF negotiates with the Global Fund and the country’s national malaria program to reallocate funding following AMF’s contribution. AMF uses its funds to purchase nets, and the Global Fund reallocates funding it would have spent on purchasing nets to distributing the nets that AMF purchases. The amount of funding that the Global Fund contributes is the same overall, but allocated differently between net purchase and distribution costs. See this section of our separate review of AMF for further details.
We do not have permission from the Global Fund to publish the proportion of costs it covers for AMF-supported campaigns (more here). For the purposes of our cost-effectiveness analysis, we therefore present AMF as covering all “upstream” costs for each campaign (96% of total costs in most locations, with in-kind government contributions accounting for the rest). See this row in our cost-effectiveness analysis. This is purely a presentational point, and does not affect our bottom line.
- 346
We currently estimate that there is a 20% to 60% chance that other funders would replace GiveWell's funding for net campaigns in our absence depending on the country. See this row in our cost-effectiveness analysis. This range includes DRC, Guinea, Nigeria (Global Fund and PMI states), Togo, and Uganda only (excluding Chad and South Sudan) for the reasons discussed in this section.
- 347
See this section of our cost-effectiveness analysis. Note: we also thought there was no chance that the Ugandan government would fund the campaign itself (Scenario 1). This was because all the ITN campaigns we have seen have been funded by external donors rather than domestic governments, and we think it is very unlikely that the Uganda government would fund the ITN campaign without external support.
- 348
See the WHO, World malaria report 2022, Annex 4 - C. Funding for malaria control for a summary of the level of support provided by different donors for malaria control in malaria endemic countries between 2019 and 2021.
- 349
See this row in our analysis of the Global Fund’s malaria funding.
- 350
The Global Fund’s malaria allocation for Uganda increased from $188,322,878 in the 2018-2020 cycle to $263,024,950 in the 2021-2023 cycle, an increase of 33%. Its allocation to Uganda’s LLIN campaign increased from $76,946,542 to $84,231,291 over the same period, an increase of 9%. GiveWell, Tracking of Global Fund spending in countries receiving funding from AMF, 2021.
- 351
The malaria programs include indoor residual spraying, routine LLIN distribution systems, integrated community case management, and other smaller programs. GiveWell, Tracking of Global Fund spending in countries receiving funding from AMF, 2021.
- 352
Our understanding is that the largest external funders of malaria in both countries are the Global Fund and PMI. See WHO, World malaria report 2022, Annex 4 - C. Funding for malaria control for a summary of the level of support provided by different donors for malaria control in malaria endemic countries between 2019 and 2021. In that period, Uganda was granted a total of approximately $300 million by PMI and the Global Fund while Nigeria was granted a total of approximately $580 million. The difference in population (which we use here as a rough proxy for funding need, since both countries have high malaria rates) was much larger—Nigeria has around five times the population of Uganda.
In the more recent Global Fund 2021-2023 grant period, Uganda received $260m in malaria grant funding compared to $418m for Nigeria. See our summary of the Global Fund’s country malaria allocations here.
Population comparisons are rough and based on figures from Google queries "population of [country]"
- 353
In the 2018-2020 cycle, the Global Fund malaria’s allocation for Togo was $31,939,623. In the 2021-2023 cycle, the allocation is $34,172,674. GiveWell, Tracking of Global Fund spending in countries receiving funding from AMF, 2021.
Note: we subsequently learned that much of this increased funding was earmarked for health systems strengthening projects, rather than programs specific to malaria. However, our best guess was that the Togolese government may have chosen to allocate less to health systems strengthening and more to the LLIN campaign if Against Malaria Foundation did not have a history of supporting LLIN campaigns in Togo.
GiveWell, Tracking of Global Fund spending in countries receiving funding from AMF, 2021, Sheet: "Togo 2021-2023," "Re Global Fund 2021-2023" section, "HSS" line. - 354
See this row in our cost-effectiveness analysis.
- 355
See this row in our cost-effectiveness analysis.
- 356
0.005 / 0.077 = ~6%, or ~1/15.
- 357
See this row in our supplementary analysis.
- 358
Health
- We use data from the Uganda National Health Expenditure Accounts in 2013-14 (available here) as a proxy for how domestic governments in malaria-endemic countries allocate their health spending. In that year, approximately 30% of the health spending was allocated to HIV/AIDS, 20% to malaria, and the rest to other programs (see this column in our accompanying spreadsheet).
- We roughly guess the dollar value required to save a life for eight of the largest categories of spending (e.g., we guess $30,000 of spending on HIV/AIDS programs is required to save one life (here), compared to $10,000 for malaria, here). As a simplifying assumption, we divide each category of spending into spending intended to save adult lives (e.g., HIV/AIDS), or spending intended to save under-five lives (e.g., malaria) (see this column in our accompanying spreadsheet). This allows us to calculate the weighted average cost required to save one child’s life ($12,254) and one adult life ($30,000).
- Finally, we translate these figures into standardized units of value using GiveWell’s moral weights for the value of averting a child death (116 units) and adult death (73 units). We also use our estimates of the proportion of spending allocated to programs intended to save adult lives (55%) and under-five lives (45%). This results in an overall weighted average of 0.0056 units of value per $ spent on health programs by domestic governments. See this row for our calculations.
Education
- As with health, we use data from Uganda as a proxy for how domestic governments in malaria-endemic countries allocate their education spending. Specifically, we rely on World Bank 2014 data that 7% of Uganda’s GDP in 2014 went towards primary education, 3% went towards secondary education and 2% went towards tertiary education (here). We then rescale these figures, resulting in estimates that 59% of education spending in Uganda goes towards primary education, 25% towards secondary education and 16% towards tertiary education (here).
- As a simplifying assumption, we assume that the primary benefit of education spending is that it increases long-run income and consumption. We benchmark our estimates to our estimates of the impact of GiveDirectly’s unconditional cash transfer program (which we think also increases income and consumption). Specifically, we roughly guess that primary education spending is 100% as valuable as GiveDirectly’s program, secondary education is 70% as valuable and tertiary education is 50% as valuable (here).
- We take a weighted average of these values, using the % of government spending on each category of education as weights. This results in an overall estimate of 0.0028 units of value per $ spent on education programs by domestic governments. See this row for our calculations.
Social security
We use a similar approach to estimating the value of social security spending as education spending. Specifically:- We use data from Uganda as a proxy for how domestic governments in malaria-endemic countries allocate their social security spending. We use World Bank 2014 estimates that social security spending accounted for 0.62% of Uganda’s GDP (here). Within this, 0.29% of GDP is in-kind spending, 0.1% is social pension spending, 0.1% is conditional cash transfers, and 0.05% is other cash transfers (here).
- We roughly guess the value generated by each of these four largest categories of social security spending, excluding the smaller categories. As with education spending, we use the simplifying assumption that the primary benefit of social security spending is that it increases income and consumption. Benchmarking to GiveDirectly’s cash transfer program, we guess that cash transfers generate 100% of the value of GiveDirectly’s program and in-kind and social pension spending each generate 70% of the value (here).
- We take a weighted average of these values, using the percentage of government spending on each category of social security spending as the weights (re-scaled to ignore smaller categories). This results in an overall estimate of 0.0026 units of value per $ spent on social security programs by domestic governments. See this row for our calculations.
- 359
See this row in our cost-effectiveness analysis. Note: although we focus on the Global Fund in our analysis, we also factor in the possibility that PMI might replace AMF’s funding for ITN campaigns if GiveWell did not provide it. This means our analysis relies on the assumption that the counterfactual value of PMI’s spending is the same as the counterfactual value of the Global Fund’s spending.
- 360
0.015 / 0.077 = ~19%, or ~⅕.
- 361
HIV (calculated on this sheet)
- As a simplifying assumption, we assume that all Global Fund spending on HIV will be used for antiretroviral therapy (ART). This is because our understanding is that this is the dominant focus of the Global Fund’s HIV programming.
- We estimate that spending on ART is 1.4x as cost-effective as direct cash transfers. This is based on the following estimates (drawn from published literature):
- ART costs $540 per person to deliver per year.
- Treating someone with HIV with ART extends their remaining life expectancy by 18 years, on average (from 9 to 27 years).
- We also use GiveWell’s standard discount rate of 4% to discount the costs of ART over time also, the standard GiveWell moral weight for averting one year of life lived with disease/disability (YLD) (2.3), and a -20% adjustment to account for lost effectiveness due to possibility of poor program implementation.
This produces an overall estimate that each $ spent on ART is 1.1x as cost-effective as direct cash transfers. See these columns for our calculations and this column for references from the secondary literature.
Tuberculosis (calculated on this sheet)
- As a simplifying assumption, we assume that all Global Fund spending on TB will be used for TB screen-and-treat programs.
- We estimate the cost-effectiveness of screen-and-treat based on GiveWell’s separate analysis of IRD Global’s TB screen-and-treat program. Our analysis includes the following key estimates:
- It costs $8 to treat one person with screen-and-treat.
- The health burden of tuberculosis is 84% as high in areas supported by the Global Fund as it is in areas supported by IRD Global’s program.
- Screen-and-treat has a 0.12% probability of averting a death.
- The additional benefits of averted morbidity from TB are 4% as high as the benefits from averted mortality.
- We use a moral weight of 60 for the value of averting one person’s death with screen-and-treat. This is lower than GiveWell’s standard value of 70 for averting the death of an adult, because the age profile of people who die from TB is older and GiveWell’s moral weights assign higher values to averting deaths at younger ages.
- As with HIV, we use a -20% adjustment to account for lost effectiveness due to possibility of poor program implementation.
This produces an overall estimate that each dollar spent on screen-and-treat is 3.2x as cost-effective as direct cash transfers. See these columns for our calculations and this column for references from the secondary literature.
- 362
The programs and their cost-effectiveness estimates are (see here):
- Malaria vector control: LLINs (campaign): 9.7x as cost-effective as direct cash transfers
- Malaria vector control: LLINs (continuous): 5.6x as cost-effective
- Malaria vector control: Indoor residual spraying (IRS): 3.2x as cost-effective
- Malaria vector control: Other: 0.5x as cost-effective
- Malaria case management (CM): 2.5x as cost-effective
- Malaria specific prevention interventions (prophylaxis): 13.6x as cost-effective
- Malaria (other): 0.5x as cost-effective
We estimate the value of each program in a separate sheet in this spreadsheet.
- 363
We use data from the Global Fund’s Unfunded Quality Demand (UQD) register to estimate how reallocated funding in the Global Fund’s portfolio is most likely to be used. The UQD register contains funding for programs that national governments would ideally like to deliver, but cannot because they do not have sufficient funding from their Global Fund grant. These programs may subsequently be funded through savings from other programs, reallocation of funding in the Global Fund’s wider portfolio, or private sector contributions.
We use data on the proportion of different malaria programs were funded from the UQD register between 2017 and 2019, and what proportion of these programs were funded by either savings from savings on other malaria programming ("grant savings") or reallocated funding within the Global Fund’s wider portfolio ("portfolio optimization").
- 364
See our discussion above on our uncertainty about malaria mortality estimates from the Global Burden of Disease project.
- 365
In 2019, we learned from researchers working on the Global Burden of Disease project that its 2019 model for estimating mortality rates takes into account the expected impact of ITN distributions on mortality.
Alexandra Walker, Engagement Officer, IHME, email to GiveWell, July 21, 2021 (unpublished). - 366
The studies we looked at are:
- Bhatt et al. 2015
- Kleinschmidt et al. 2018
- Dolan et al. 2019
- Jakubowski et al. 2017
- Afoakwah et al. 2015
- Kamau et al. 2017
Each of these studies evaluated the impact of nets on malaria, except Jakubowski et al. 2017, which is an evaluation of the President’s Malaria Initative’s impact on malaria. We included it in our analysis even though it does not focus solely on nets because we expect that a large portion of PMI’s funding goes towards nets.
- 367
WHO estimates that the proportion of households in sub-Saharan Africa with access to at least one ITN rose from 5% in 2000 to 68% in 2021. We haven’t vetted this estimate, but this is consistent with our expectations that net coverage rose dramatically in this period as mass campaigns scaled up. WHO, World malaria report 2022, p. 66.
- 368
Data available at Malaria Atlas Project, ITN use 2010-2020.
- 369
GiveWell, analysis of ITNs and child mortality trends, September 2023, unpublished.
- 370
“Core interventions for malaria vector control are applicable for all populations at risk of malaria in most epidemiological and ecological settings, namely: i) deployment of insecticide-treated nets (ITNs) that are prequalified by WHO, which in many settings are long-lasting insecticidal nets (LLINs); and ii) indoor residual spraying (IRS) with a product prequalified by WHO. Once high coverage with one core intervention has been achieved, supplementary interventions – namely the deployment of chemical or biological larvicides – can be used in addition to the core interventions in specific settings and circumstances.” WHO, Guidelines for Malaria Vector Control, 2019, p. xiv.
- 371
WHO, World malaria report 2022, p. xxv, "Distribution and coverage of malaria prevention" section.
- 372
We’re not sure why this is. Anecdotally, two factors we’ve heard that may be driving this are:
- Nets are widely seen as an effective malaria prevention tool. There was a significant global advocacy effort to encourage high coverage of nets, and national malaria programs and malaria stakeholders are broadly agreed on their importance for malaria control.
- There is strong community demand for nets, since they are visible compared to other malaria control tools. Communities have also been receiving them for a long time, and developed an expectation of continued supply.
- 373
“GiveWell is not wrong in asserting that ITNs are an excellent investment. However, there are many factors that should be taken into consideration when allocating funding for their procurement, and some of your assumptions used to calculate cost-effectiveness may need updating. Decisions should be tailored to specific settings and products since there is great variability in usage patterns, durability, entomological factors and the relative effectiveness of different types of ITNs.” David McGuire, “Review of GiveWell LLIN report,” 2023 (unpublished).
- 374
“Historically I believe that funders have relied too much on the so-called experts in North America and Europe (like myself) without sufficiently consulting with those in Africa tasked to make it all work. Many of these managers are frustrated by the fact that donors are prioritizing nets over other VC tools rather than allowing them to tailor their VC strategies for optimal impact based on what they think will work best within their specific transmission and socio-cultural settings. Malaria managers are enthusiastic about ITNs, especially new dual-AI nets, but they are also quite vocal about the challenges with uptake and attrition and the need for complementary interventions.”
“GiveWell would also be wise to consider future investment in other vector control tools that are currently available or under development in settings where they may be more appropriate, preferred by NMCPs/users, or provide significant additional impact when layered on top of ITNs. For example, there are many countries, particularly in East and Southern Africa where there is a strong preference for and long history of IRS…
NMPs, including Uganda's NMCD, have expressed concerns for many years about the potential impact of reducing IRS coverage in high transmission areas. This is based on very bad experiences they have had in Uganda when donors have withdrawn IRS funding. More broadly, data generated under the NgenIRS project showed spikes in malaria incidence when IRS was removed from areas where nets are deployed.” David McGuire, “Review of GiveWell LLIN report,” 2023 (unpublished). - 375
“Historically I believe that funders have relied too much on the so-called experts in North America and Europe (like myself) without sufficiently consulting with those in Africa tasked to make it all work. Many of these managers are frustrated by the fact that donors are prioritizing nets over other VC tools rather than allowing them to tailor their VC strategies for optimal impact based on what they think will work best within their specific transmission and socio-cultural settings.” David McGuire, “Review of GiveWell LLIN report,” 2023 (unpublished).
- 376
“It is noteworthy that no country that has successfully eliminated malaria has done so with nets. Nets are an effective control tool in medium to high-transmission areas, but as countries progress towards elimination they must rely more on surveillance, case management, focal IRS, larviciding, etc. And, as malaria rates come down, cost-effectiveness becomes a less useful metric since nothing meets traditional cost-effectiveness thresholds in low transmission settings.” David McGuire, “Review of GiveWell LLIN report,” 2023 (unpublished).
- 377
“With between 200-300 million ITNs being distributed each year, countries and their donor and implementing partners should also consider the environmental impact of accumulating plastic waste. There are pilot efforts underway to minimize the amount of plastic packaging and to implement recovery and recycling of ITNs. However, looking ahead it would be preferable to deploy VC tools that would help enable more significant reduction of plastic waste and easier and more environmentally friendly disposal.” David McGuire, “Review of GiveWell LLIN report,” 2023 (unpublished).
- 378
“Furthermore, to maximize the ability of donors to procure as many nets as possible, there has been a move to standardize the size, shape and color of ITNs. This makes perfect economic sense, but research has shown great variability in user preferences and, therefore, this one-size-fits-all approach may be a contributing factor to reduced uptake of ITNs. For example, many people prefer conical nets since they are much easier to hang and tie up during the day, and in some predominantly Muslim communities there is an aversion to white nets because of their resemblance to traditional funeral shrouds.” David McGuire, “Review of GiveWell LLIN report,” 2023 (unpublished).
- 379
“This tool is designed to help National Malaria Control Programs explore the most cost effective option of deploying current World Health Organisation (WHO) recommended mosquito net and IRS products for malaria control.
In this tool, a project is a collection of regions and a region is defined as a management unit - this could be an administration unit, province or village. For each region defined in the tool, there is a set of outputs summarising the impact and cost effectiveness of intervention packages.
IRS is very focal and usually completed in a smaller region of a larger province or district. The model assumes that IRS is applied at random to the population so it is more appropriate to create separate IRS regions and non-IRS regions for this assessment and adjust population size accordingly.” Imperial College London, Malaria Intervention Tool (MINT) - 380
“The Lives Saved Tool is a mathematical modeling tool which allows users to estimate the impact of coverage change on mortality in low and middle income countries.” The Lives Saved Tool (LiST), "Home"
- 381
Examples of backwards-looking analysis and data we’ve incorporated into our cost-effectiveness analysis:
- Data on the number of ITNs delivered in previous campaigns from AMF’s distribution data. We use this as part of our cost per net analysis (more).
- Estimates of Global Fund distribution costs in previous campaigns, based on data shared by the Global Fund. We also use this in our cost per net analysis (more).
- Estimates of the gap between campaigns at the province level in DRC between 2021 and 2023 with and without support from AMF. We used this analysis to update our adjustment for moving distributions closer together (more).
- 382
Examples of backwards-looking analysis we’ve not yet prioritized:
- Analysis of what happened in cases we declined to fund nets (i.e., did another funder fill the gap). This could inform our adjustment to account for other actors’ spending.
- An analysis of what countries AMF has allocated funding to using non-GiveWell funds, and how much. This affects our analysis because we think that one impact of GiveWell funding for AMF may be to divert AMF’s other funding away from GiveWell-supported programs into non-GiveWell supported programs, some of which GiveWell might estimate to be less cost-effective.
- An analysis of data on the number of households registered in AMF-supported campaigns. We discuss the campaign registration process in detail in our separate report on AMF here.
- Reviewing data on the price paid by AMF to purchase nets for previous campaigns. We have previously focused on using forward-looking projections for net costs in our cost per net analysis (more).
- 383
“The World Health Organization (WHO) has recommended a new vaccine, R21/Matrix-M, for the prevention of malaria in children. The recommendation follows advice from the WHO: Strategic Advisory Group of Experts on Immunization (SAGE) and the Malaria Policy Advisory Group (MPAG) and was endorsed by the WHO Director-General following its regular biannual meeting held on 25-29 September.
WHO also issued recommendations on the advice of SAGE for new vaccines for dengue and meningitis, along with immunization schedule and product recommendations for COVID-19. WHO also issued key immunization programmatic recommendations on polio, IA2030 and recovering the immunization programme.The R21 vaccine is the second malaria vaccine recommended by WHO, following the RTS,S/AS01 vaccine, which received a WHO recommendation in 2021. Both vaccines are shown to be safe and effective in preventing malaria in children and, when implemented broadly, are expected to have high public health impact. Malaria, a mosquito-borne disease, places a particularly high burden on children in the African Region, where nearly half a million children die from the disease each year.” WHO, "WHO recommends R21/Matrix-M vaccine for malaria prevention in updated advice on immunization," 2023
- 384
“Stephensi breeds in water and thrives in congested cities, where unreliable piped-water systems often force people to store water around their homes, and poor trash collection provides ample spots (such as old bottle caps) for mosquitoes to lay eggs. The species is poised to descend on what public health experts describe as a largely malaria-naive human population: Most urban dwellers don’t have immunity from repeated prior exposure and may fall much sicker.” Nolen, "An Invasive Mosquito Threatens Catastrophe in Africa," 2023
- 385
“As more and more people are protected by nets or sprays at home, mosquitoes have begun to bite more outdoors and in the daytime, instead of indoors and at night, the historic pattern of the malaria vector species in Africa.” Nolen, "Mosquitoes Are a Growing Public Health Threat, Reversing Years of Progress," 2023
- 386
“There appears to be a significant shift in malaria burden in Uganda and elsewhere from children <5 to school-age children. Not only are there increased cases of severe malaria among this older group, but they also represent one of the largest parasite reservoirs within communities, so this must be taken into account when deciding how to deploy nets and other malaria interventions layered on top of them.” David McGuire, “Review of GiveWell LLIN report,” 2023 (unpublished).