Note: This page summarizes the rationale behind a GiveWell-recommended grant to Helen Keller Intl. Helen Keller Intl staff reviewed this page prior to publication.
In a nutshell
In April 2023, GiveWell recommended a $6 million grant to Helen Keller Intl for vitamin A supplementation (VAS) in Madagascar. Helen Keller is one of GiveWell's Top Charities.
With this grant, Helen Keller Intl will support campaigns to provide VAS in six regions in Madagascar every six months for four years. Vitamin A deficiency makes children susceptible to infectious disease, a major cause of child mortality. VAS is thought to reduce this susceptibility.
Published: June 2023
Table of Contents
Summary
Why we made this grant
- We think this grant is highly cost-effective. Our best guess is this grant is 13 times as cost-effective as cash transfers, which is above our current bar of 10x cash. Intuitively, this is because we think:
- Helen Keller’s activities lead to a large increase in uptake of VAS among children in areas Helen Keller works. Government-funded health systems are reaching roughly half of children with VAS and there is very little external funding available for VAS in these 6 regions to increase coverage above that level. Helen Keller will fund door-to-door campaigns, which in other locations have generally reached more than 80% of children.1
- VAS is relatively simple and cheap to deliver: All children ages six months to five years are given a few drops of a solution containing vitamin A by mouth.
- In areas with high child mortality, VAS reduces mortality by a modest but meaningful amount. We also believe there are substantial benefits beyond reductions in mortality.
A sketch of our cost-effectiveness analysis is below:
| Grant size | $6 million |
| Mortality benefits of the program | |
| Number of children under 5 covered | 4.9 million |
| Percent of children reached who would not have received VAS without the grant | 34% |
| Mortality rate among children who do not receive VAS | 0.79% |
| Reduction in mortality rate from VAS | 12% |
| Helen Keller cost per death averted (equals $6 million / [4.9 million x 34% x 0.8% x 12%]) | $4,000 |
| All actors cost per death averted (equals $10 million / [4.9 million x 34% x 0.8% x 12%]) | $6,300 |
| Moral weight for each death averted (we use moral weights to compare outcomes like deaths averted and increases in income) | 119 |
| Cost-effectiveness from mortality benefits only (times more cost-effective than providing unconditional cash transfers in the world’s poorest communities, “x cash”) (equals 120/$4,000/0.00335 units of value per dollar from cash transfers) |
9x cash |
| We also incorporate other benefits. In the final assessment, % of benefits from… | |
| … reducing child mortality | 44% |
| … avoiding short-term illness and the costs of treatment | 23% |
| … leveraging government resources | 14% |
| … other programs that are delivered alongside VAS (deworming, vaccines, etc.) | 10% |
| … improved child development (increased income in adulthood) | 9% |
| Overall cost-effectiveness (“x cash”) | approximately 12x cash |
You can see our full cost-effectiveness analysis for this grant here and a simple version here.2
Main reservations
- What is the child mortality rate? Record keeping on child deaths in the locations where GiveWell has supported VAS is not reliable. Our analysis uses estimates of child mortality from the Global Burden of Disease tool, which rely on a number of modeling assumptions.
- How much does VAS decrease child mortality in current contexts, and in Madagascar in particular? A meta-analysis of randomized controlled trials of VAS estimated a 24% reduction in child mortality. We guess that these studies overstated the impact of VAS by about a third at the time they were conducted. We also estimate vitamin A deficiency and infectious disease prevalence are less severe in Madagascar today than they were in the times and places where the studies were conducted. Overall, we estimate that VAS causes a 12% reduction in mortality in Madagascar today.
- How many of the children reached by this program would have received VAS without the program? Some children receive VAS without this program, through the routine health system. A recent survey estimated that 44% of children have been receiving VAS in the areas Helen Keller plans to support. We may over- or under-estimate cost-effectiveness if either (a) Helen Keller's support primarily leads to reaching children who would [not] have received VAS without their support, or (b) the additional children reached are systematically at lower [higher] risk of illness and death than those who are reached by the routine health system.
Funding for the grant
This grant was funded in April 2023 by the Rauch Family Foundation, on GiveWell's recommendation.
Planned activities and budget
Vitamin A deficiency is a major public health issue for preschool-aged children (aged 6 to 59 months) and can lead to visual impairment as well as increased risk of illness and mortality from common childhood infections.3 The World Health Organization (WHO) recommends that all preschool-aged children in areas where vitamin A deficiency is a public health problem receive vitamin A supplements two to three times per year.4 To distribute supplements, health workers cut open capsules containing vitamin A in solution and squeeze the contents of the capsules directly into children's mouths.5 For more information on vitamin A deficiency and supplementation, see here.
This $6 million grant will fund four years of vitamin A supplementation (VAS) in Madagascar, at a cost of about $1.5 million per year.6 The program will support VAS in six of the 23 regions in Madagascar.7 Activities will include:
- Providing technical support at the national level.
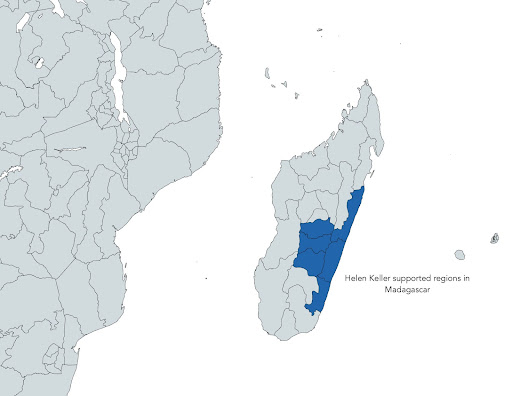
- Setting up initial support to six regions located in the center and eastern part of Madagascar. Helen Keller plans to start the program in 2 regions in 2023, add 2 more regions in the first half of 2024, and add the final 2 regions in the second half of 2024.8
- Supporting the strengthening of the health system in those regions to improve the management of the supply chain and information systems for VAS.
- Supporting routine delivery of VAS at the health facility level for populations living within five kilometers of health facilities and through community workers for all other children.
- Organizing catch-up events at the end of each semester to supplement children missed by routine delivery, which may be discontinued in some or all areas if strengthened routine delivery reaches a large proportion of targeted children.9
- Door-to-door coverage surveys to assess the success of campaigns and identify problems.10
The case for the grant
- Cost-effectiveness – We estimate that this grant will meet our bar for cost-effectiveness (more).
- Funding landscape – There has not been external support for VAS in most regions of Madagascar in recent years, which has resulted in moderately low VAS coverage. We would guess that that situation would persist without new external funding (more).
Cost-effectiveness
Based on our cost-effectiveness analysis of VAS in Madagascar, we estimate this grant will avert the deaths of approximately 1,590 children over four years, as well as have additional benefits for children's long-run incomes by protecting them from illness at a crucial developmental stage.11 We estimate that this program is 12 times as cost-effective as unconditional cash transfers to households living in some of the world's poorest communities,12 the benchmark we use to compare programs. We believe this program is in the range of cost-effectiveness of programs we expect to direct funding to as of early 2023, which are programs that are 10 or more times as cost-effective as cash transfers.
We discuss our model of Helen Keller's cost-effectiveness on this page. In considering this grant, we made the following updates to that model:
- Adjusted for double treatment: We adjust our cost-effectiveness estimates downwards to account for the possibility that children who are counted as reached by Helen Keller-supported VAS campaigns may have already received VAS from another source, and thus not benefit from the additional supplement. We estimate that 44% of targeted children in the six regions in question had access to VAS through routine health services prior to Helen Keller's entry to those regions, so we adjust our estimate of the effectiveness of this program downwards by 44%. This adjustment is based on data from the 2021 Demographic and Health Survey (DHS), and is higher than the existing VAS coverage rate we assume in other countries we support.13
- Estimated the cost per supplement based on other countries: We don't yet have data on the cost to deliver a round of VAS in Madagascar, because Helen Keller has not implemented a VAS program there before. We estimated that the cost would be equal to an average of other countries for which we do have data, which is $1.02 per child per supplementation round. See more information below in our "risks and reservations" section.
- Adjusted for targeted areas with high mortality rates: We applied a 17% upward adjustment, because the districts within Madagascar where Helen Keller plans to work have higher mortality rates than the national average for children who are in the VAS-eligible age range (6-59 months old), according to the 2021 DHS.14 By prioritizing areas where children are more at risk than average, Helen Keller's VAS program can have a higher impact.
- Estimated vitamin A deficiency rates: Vitamin A deficiency (VAD) rates are a key input into our external validity adjustment for our cost-effectiveness analysis of VAS. The external validity parameter in the model seeks to capture differences in the characteristics of populations targeted by this grant relative to populations who participated in trials where the impact of VAS was estimated.15 Since there has not been a survey of vitamin A deficiency (VAD) rates in Madagascar since 2000, we created an estimate of our best-guess of Madagascar's VAD rate of 28%. Our estimate combines VAD estimates from the most recent vitamin A deficiency survey available (adjusted for estimated changes over time) with vitamin A deficiency estimates from the Institute for Health Metrics and Evaluation's Global Burden of Disease tool.16 This led to an external validity adjustment of 59%.
Funding landscape
In a scoping visit to Madagascar, Helen Keller learned that in recent years, there has been limited support for VAS in Madagascar from other partners. UNICEF supported the Madagascar Ministry of Health to pilot routine delivery of VAS in 2018,17 but currently does not have sufficient funding for VAS to cover campaigns.18 Nutrition International contributed to adding VAS to a measles campaign in 2022.19 We don't know of any other organizations currently focusing on delivering VAS campaigns in Madagascar.20 This information leads us to believe that there is room for Helen Keller to have additional impact on VAS in Madagascar.
We adjust our cost-effectiveness analysis for the likelihood that this grant funding will crowd out funding from other sources in the near-term. We think it's very unlikely that the government would increase its support for VAS in Helen Keller's absence to a level that is similar to what Helen Keller typically provides, so we estimate a very low probability (5%) that Helen Keller's funding would crowd out funding from the government. We also think there is a low probability (20%) that Helen Keller will crowd out funding from other philanthropic sources, because there has been limited external funding in Madagascar for VAS in recent years.
Risks and reservations
- Child mortality rates: Record keeping on child deaths in the locations where GiveWell has supported VAS can be unreliable.21 Our analysis uses estimates of child mortality from the Institute for Health Metrics and Evaluation's Global Burden of Disease tool; these estimates rely on a number of modeling assumptions.22 If baseline child mortality is actually lower than estimated, then VAS would avert fewer deaths than we estimate, whereas we could be underestimating the impact of this grant if child mortality is higher than estimated.
- Uncertainties about the impact of VAS in current contexts: Our current cost-effectiveness estimate relies heavily on a review of VAS studies, Imdad et al. 2017. The most heavily-weighted study in that analysis was done in 2013 and did not find a statistically significant effect on mortality.23 The five other studies that receive the most weight in the analysis are about 30 years old.24 Both these facts raise questions about the impact of VAS in current contexts. In our cost-effectiveness analysis, we have both (a) an internal validity adjustment which estimates that the meta-analysis finding is 26%25 overstated due to bias in how the studies were conducted, publication bias, etc., and (b) an external validity adjustment to adjust for differences between trial contexts and the contexts in which these VAS programs will be implemented (a 41% reduction in impact for Madagascar).26
- Which of the children who are reached by this program would have received VAS without the program? As mentioned above, a recent survey estimated that 44% of children have been receiving VAS in the areas Helen Keller plans to support, and we adjust for this in our model.27 We may over-estimate cost-effectiveness if either (a) Helen Keller's support primarily leads to reaching children who would have received VAS without their support, or (b) the additional children reached are systematically at lower risk of illness and death than those who are reached by the routine health system. If children would not have received VAS without support or these children are at higher risk than those reached by the routine health system, we may be underestimating cost-effectiveness.
- Risks of bias in monitoring: Helen Keller commissions post-event coverage surveys for VAS campaigns.28
In reviewing coverage surveys for another recent grant, we came across two risks of bias that we have not have thoroughly understood in the past:
- Helen Keller does a survey for only one of the two rounds of VAS each year, and surveys are more frequently occurring during the non-rainy season.29 We think it's possible that coverage rates may be substantially lower in the rainy season, because distributions may be impeded by flooding or challenging road conditions.
- Various decision-makers for campaigns know whether or not a campaign will have a coverage survey, and may know which districts will be surveyed.30 Both of these facts could bias coverage results upwards.
We have brought up these concerns with Helen Keller. In response, Helen Keller has decided not to inform regional authorities in several countries about whether or not there will be a coverage survey in their region until after the campaign, and it may expand this practice to additional locations.31 We remain concerned that Helen Keller has typically conducted coverage surveys following one of the two VAS campaigns each year32 and decision-makers may be told or be able to predict which campaign will and will not have a coverage survey. We plan to continue to discuss mitigating these risks of bias. These concerns are incorporated into our cost-effectiveness analysis here.
- Uncertain costs in Madagascar: We recommended this grant based on rough estimates of costs in Madagascar. We could have funded Helen Keller to develop more detailed program plans and a budget ahead of recommending this grant, which would have resulted in a delay to implementation. We have worked with Helen Keller before to shift funds when actual costs fell above or below budgeted amounts, and think that Helen Keller's decision-making and prioritization was largely aligned with maximizing impact. This gives us confidence that should the budget be off, Helen Keller can course correct. There is a risk that costs will be much higher than anticipated and thus the cost-effectiveness of the program lower; at this point, Helen Keller does not expect Madagascar to be a significantly more challenging operating environment than Helen Keller's other VAS program geographies.
- Time-intensive to start a new program: Since Helen Keller doesn't currently work in Madagascar, it will need to set up a new office for this program and hire leadership staff for that office, which we expect will take its VAS program leadership a significant amount of time over the coming months. It's possible that it would be better for its leadership to focus on quality improvements to their current programs instead, such as testing ways to reduce costs or improving the rigor of coverage surveys.
Plans for follow up
- Annually, we will continue to receive narrative progress reports, coverage survey reports, and spending reports from Helen Keller.33
- We will also continue our monthly calls with Helen Keller to get informal updates.
- We will request annual room for more funding updates from Helen Keller, which we'll use, in combination with conversations, to understand more about how the funding landscape is changing.
- We will ask Helen Keller the following questions:
- Did Helen Keller's board and leadership approve opening an office in Madagascar?
- Have there been any unexpected challenges to opening an office and hiring employees?
- What has Helen Keller learned about the context in Madagascar that it didn't know before this grant decision?
- What VAS work is UNICEF supporting in Madagascar and how has that changed since Helen Keller's scoping visit in 2022? Are there any other new sources of funding for VAS in Madagascar?
Internal forecasts
| Confidence | Prediction | By time | Resolution |
|---|---|---|---|
| 75% | Helen Keller will establish a presence (at least one employee) in Madagascar within six months of approval of this grant | October 2023 | Yes |
| 85% | Helen Keller will establish a presence (at least one employee) in Madagascar within one year of approval of this grant | April 2024 | Yes |
| 65% | Helen Keller will expand its support beyond the initial 6 districts within three years of approval of this grant | April 2026 | - |
Our process
Our process for this grant decision relied heavily on our prior work on modeling the cost-effectiveness of VAS, and our monthly discussions with Helen Keller. For this particular grant, in order to determine the location of a new program, we had discussions with Helen Keller and Nutrition International in 2021 and 2022 about what locations might have (a) high cost-effectiveness, (b) reasonably high room for more funding, and (c) low risk of crowding out other funders. Helen Keller's VAS director and a regional director then visited Madagascar and had meetings with stakeholders in October 2022 and provided us with a scoping report. We created a cost-effectiveness model based on our standard VAS model and some updates for Madagascar (discussed above).
For internal review, a Senior Researcher and a Senior Program Associate gave feedback on the plan for investigating the grant, and a Senior Program Associate gave feedback prior to final grant approval by a Senior Program Officer.
Sources
- 1
See Results section of GiveWell, Helen Keller Intl's Vitamin A Supplementation Program, 2023.
- 2
Simple version uses slightly different calculations and therefore generates a slightly different cost-effectiveness result.
- 3
"Vitamin A deficiency is a major public health problem affecting an estimated 190 million preschool-age children, mostly from the World Health Organization (WHO) regions of Africa and South-East Asia (1). Infants and children have increased vitamin A requirements to promote rapid growth and to help combat infections. Inadequate intakes of vitamin A at this age could lead to vitamin A deficiency, which, when severe, may cause visual impairment (night blindness) or increase the risk of illness and mortality from childhood infections such as measles and those causing diarrhoea (2)." World Health Organization, "Guideline: Vitamin A supplementation in infants and children 6-59 months of age," 2011, p. 2.
- 4
- In settings where vitamin A deficiency is a public health problem, vitamin A supplementation is recommended in infants and children 6–59 months of age as a public health intervention to reduce child morbidity and mortality (strong recommendation). The quality of the available evidence for all-cause mortality was high, whereas for all other critical outcomes it was moderate to very low. The quality of the available evidence for outcomes in human immunodeficiency virus (HIV)- positive children was moderate for all-cause mortality." World Health Organization, "Guideline: Vitamin A supplementation in infants and children 6-59 months of age," 2011, p. 1.
- One dose of 100,000 IU of vitamin A is recommended for infants aged 6 to 11 months of age, and a 200,000 IU dose of vitamin A is recommended for children 12 to 59 months of age every four to six months. Table 1, World Health Organization, "Guideline: Vitamin A supplementation in infants and children 6-59 months of age," 2011, p. 5.
- WHO defines vitamin A deficiency to be of mild public health importance when rates of vitamin A deficiency (defined as a measure of serum or plasma retinol <0.70 µmol/l) among preschool-aged children or pregnant women are between 2% and 10%, moderate public health importance when rates of vitamin A deficiency among preschool-aged children or pregnant women are between 10% and 20%, and severe public health importance when rates of vitamin A deficiency among preschool-aged children or pregnant women are greater than or equal to 20%. World Health Organization, "Global prevalence of vitamin A deficiency in populations at risk," WHO Global Database on Vitamin A Deficiency, 2009, p. 8, Table 5.
- 5
- "For distribution sites visited by an independent HKI supervisor, 86% met the criteria for minimum quality threshold for service delivery defined as 1) health worker used scissors to cut the capsule 2) health worker asked the age of the child 3) health worker squeezed the drops into the child’s mouth 4) health worker used the correct dose of VAS and 5) were there no stock-outs of VAC." HKI VAS project year 1 report 2014 (unpublished).
- Table 1: Suggested vitamin A supplementation scheme for infants children 6–59 months of age, Row 'Route of administration': "Oral liquid, oil-based preparation of retinyl palmitate or retinyl acetate, An oil-based vitamin A solution can be delivered using soft gelatin capsules, as a single-dose dispenser or a graduated spoon (20)." World Health Organization, "Global prevalence of vitamin A deficiency in populations at risk," WHO Global Database on Vitamin A Deficiency, 2009, p. 5, Table 1.
- 6
Estimated cost of $1.5 million per year is from David Doledec, Program Director, Vitamin A Supplementation, Helen Keller Intl, email to GiveWell, January 9, 2023 (unpublished).
- 7
The regions are: Vakinankaratra, Atsinanana, Amoron'i Mania, Haute Matsiatra, Vatovavy and Atsimo-Atsinanana. Helen Keller, Madagascar VAS scoping report, October 2022, Annex: proposed target regions and populations, p. 5.
- 8
David Doledec, Program Director, Vitamin A Supplementation, email from Helen Keller Intl, April 18, 2023 (unpublished)
- 9
"We recommend that Helen Keller focuses on the following in Madagascar:
- Provide technical support at the national level to develop policies, guides, and tools to support a sustainable delivery system for VAS
- Set up initial support to 6 regions located in the center and eastern part of Madagascar (see map), targeting around 1.5 million children for the 6 regions proposed
- Support the strengthening of the health system in regions to improve the management of the supply chain and information system for VAS
- Support routine delivery of VAS at the health facility level for populations living within 5 kilometers of these facilities and through community workers for all other children.
- Organize catch-up events at the end of each semester to supplement children missed by routine delivery, until routine delivery can reach all targeted children." Helen Keller, Madagascar VAS scoping report, October 2022, Annex: proposed target regions and populations, p. 5.
- 10
- Helen Keller plans to start the program in two regions in 2023 and do coverage surveys in those regions, add two more regions in the first half of 2024 and do coverage surveys there, then add the final two regions in the second half of 2024 and do coverage surveys there. David Doledec, Program Director, Vitamin A Supplementation, email from Helen Keller Intl, April 18, 2023 (unpublished).
- Based on what Helen Keller has told us in the past, it will then switch to random sampling of regions to monitor coverage.
- See our most recent review of Helen Keller's coverage surveys here.
- 11
- "Reducing exposure to malaria during childhood may have an effect on long-term productivity and earnings. We include these possible benefits in our cost-effectiveness analyses for seasonal malaria chemoprevention and mass distribution of long-lasting-insecticide-treated nets. In 2018, we reviewed research on whether vitamin A supplementation may also lead to long-term effects on productivity and earnings by reducing incidence of various infectious diseases, and decided to also include a developmental effects parameter for vitamin A supplementation in our cost-effectiveness analyses." GiveWell, "Vitamin A supplementation," 2018
- See our estimate of development effects in this section of our cost-effectiveness analysis here.
- 12
Note that a) our cost-effectiveness analyses are simplified models that are highly uncertain, and b) our cost-effectiveness threshold for directing funding to particular programs changes periodically. See GiveWell’s Cost-Effectiveness Analyses webpage for more information about how we use cost-effectiveness estimates in our grantmaking.
- 13
See those other countries' rates here.
- 14
See calculations here.
- 15
More information about this parameter in the cell note here.
- 16
See these calculations here.
- 17
"As campaigns were phasing out, UNICEF and the Ministry of Health conducted a pilot study in 2018 to evaluate how routine delivery for VAS could be organized using health facilities and community actors." Helen Keller, Madagascar VAS scoping report, October 2022. p. 2.
- 18
"UNICEF lacks funding for VAS , and the Covid-19 crisis seems to have shifted focus from VAS to other activities. Throughout 2020 and 2021, no significant VAS activities took place in the country. A measles campaign was organized in May 2022 to which VAS was added, but despite financial contribution from Nutrition International, coverage did not increase beyond 65%. There is no visibility on future campaigns, and although UNICEF has some funds they can use for VAS, these are not specific to VAS and insufficient to support campaigns." Helen Keller, Madagascar VAS scoping report, October 2022, p. 2
- 19
"A measles campaign was organized in May 2022 to which VAS was added, but despite financial contribution from Nutrition International, coverage did not increase beyond 65%." Helen Keller, Madagascar VAS scoping report, October 2022, p. 2.
- 20
USAID and the World Bank have large-scale community health programs in Madagascar that include nutrition among other services, but have no specific VAS focus: "USAID (ACCESS and IMPACT) and the World Bank (PARN) have ongoing large-scale community health programs which cover the majority of Madagascar’s regions. Nutrition is among the services provided. However, there is no specific attention to the delivery of VAS, supply chain, and information system management." Helen Keller, Madagascar VAS scoping report, October 2022, p. 3.
- 21
For example, the Institute for Health Metrics and Evaluation explains that mortality data can be flawed: "This last piece – the underlying cause of death – is what GBD researchers use to produce mortality statistics. Understanding the underlying cause of death in a population allows public health officials to develop interventions that target the root cause.But picking out the underlying cause of death can be difficult. Many countries in the world do not have functioning vital registration systems, and even for those countries who do, there are often high levels of misclassification and vague reporting of causes of death on death certificates." Institute for Health Metrics and Evaluation, Determining causes of death: How we reclassify miscoded deaths," 2018.
- 22
- GBD's mortality estimates for Madagascar model mortality based on many sources, such as Demographic and Health Surveys, Malaria indicator surveys, and Vital Registration Death Data. Institute for Health Metrics and Evaluation, Global Burden of Disease Study 2019 (GBD 2019) Data Input Sources Tool.
- "GBD researchers use models to determine the relationship between the known data points that we have, and then estimate the range of possible values (researchers call this the “uncertainty interval”).... GBD models now consider thousands of data sources and millions of data points to produce measures of death and disability for hundreds of diseases and risks in countries around the world. Incorporating this many sources, and producing this many results, would not be possible without models." Institute for Health Metrics and Evaluation, "The power of models", 2018.
- 23
The DEVTA 2013 study received approximately 62% of the weight in the analysis in Imdad et al. 2017, Figure 3, p. 17.
- The weight of each study in the analysis can be seen in Imdad et al. 2017, Figure 3, p. 17.
- The Deworming and Enhanced Vitamin A (DEVTA) was a large VAS trial in India, with results published in 2013. The results of DEVTA were published in Awasthi et al. 2013, which estimates that VAS reduced child mortality by 4% and cannot rule out the possibility that VAS did not affect child mortality at all (the 95% confidence interval ranged from a 3% increase in child mortality to an 11% decrease).
- 24
- The five studies are: Ross et al. 1993, West et al. 1991, Herrera et al. 1992, Daulaire et al. 1992, and Sommer et al. 1986. For more details on these studies, see our page on VAS here.
- The weight of each study in the analysis can be seen in Imdad et al. 2017, Figure 3, p. 17.
- 25
- The calculations behind this figure can be found here. We estimate an adjustment of 74%, meaning the original value is 26% higher than we think it should be (100-26=74). The confidence we have in the point estimate for VAS from the meta-analysis is meaningfully but not hugely lower than for malaria nets or seasonal malaria chemoprevention, two other top charity programs. This is in part because we are more unsure about what causes of death VAS averts. We also note that the majority of the randomized controlled trials included in the meta-analysis we rely on for our estimate of the relative risk of all cause mortality for children aged 6- to 59-months participating in VAS programs took place in the 1980s and 1990s. Our rough guess is that RCTs that took place several decades ago generally have more methodological limitations than more recent trials.
- See publication dates of trials included in "Analysis 1.1. Comparison 1 Vitamin A versus Control, Outcome 1 All-cause mortality at longest follow-up" in Imdad et al. 2017, p. 90.
- 26
See this adjustment here. It is a 59% adjustment, which means it is reducing the impact by 41% (100-41=59).
- 27
- This data is from Institut National de la Statistique (INSTAT) Antananarivo, Madagascar, Enquête Démographique et de Santé à Madagascar (EDSMD-V) 2021, 2022, Tableau 11.9, p. 238.
- See the adjustment here in our cost-effectiveness analysis.
- 28
See this spreadsheet for details on post-event coverage surveys for VAS campaigns.
- 29
Helen Keller Intl, conversation with GiveWell, September 6, 2022 (unpublished).
- 30
Helen Keller Intl, conversation with GiveWell, September 6, 2022 (unpublished).
- 31
Helen Keller Intl, email to GiveWell, January 9, 2023 (unpublished).
- 32
Most campaigns generally have coverage surveys after only one round of VAS, though in some years surveys were conducted for both rounds for some countries. See this spreadsheet, sheet "Comprehensiveness (2018-22)," column "Have we seen a coverage survey?"
- 33For recent examples, see Helen Keller Intl, Annual narrative report, April 2022, Helen Keller Intl, Annual coverage report, April 2022, and Helen Keller Intl, Expenditure report, April 2022.