Please note: this report was completed based on information VillageReach sent us in July to December 2012. VillageReach notes that owing to the dated information in this report, this report contains inaccuracies. VillageReach also notes that it is working on updating its plans and will provide information to its donors directly from its website.
Summary of project progress
In the first half of 2012, distributions through VillageReach's Mozambique Dedicated Logistics System (DLS) occurred regularly in the 4 provinces in which it is working (more).
We do not yet have the information necessary to report on the program's success in reducing the frequency of "stockouts," (instances when a health center's stock of a vaccine was used up completely) because we have received limited stockout data (more). We are not confident in the accuracy of the data we have seen (more).
VillageReach is in discussion with a potential funder that may support the extension of its work in Cabo Delgado and Niassa. The current budget includes funding for its work in the two provinces through March 2013, after which the scale of the program would be reduced to operating in Gaza and Maputo provinces (more). Based on its experience over the course of the scale-up, VillageReach is now less confident than it was at the start of the program that the provincial governments will maintain its program once it exits the country.1
Where we stand on VillageReach
In November 2011, we removed our #1 ranking from VillageReach because we did not believe that VillageReach had short-term room for more funding for its scale-up project in Mozambique. At that time, we estimated that VillageReach needed to raise an additional ~$1 million in "unsourced funds" (from new, not previously expected sources) to fund its activities in 2014-15.
In early 2012, VillageReach reported that it was substantially changing the scope of its project to deal with some of the challenges it had faced in its scale-up (our discussion of these changes is in our March 2012 update). Due to cost increases, the net result of these changes was a small increase in the total amount of "unsourced funding" needed to fully fund the project.2
Although we now believe that this project may have room for more funding -- i.e., were VillageReach to receive significant additional funding for this project it might extend the length of its work in Mozambique -- we are not planning to rank it among our top charities.
Table of Contents
Note on reliability of information in this report
One of the reports we received for this update on VillageReach's progress in Niassa province contained a chart that appears to have been copied from a report on Cabo Delgado province3 (VillageReach later sent us a corrected version of the report4 ). We received two charts of stockouts by vaccine in Cabo Delgado in the second half of 2011 (in different reports), and some of the data in the charts does not match. There have been a couple of past instances of data quality problems in reports VillageReach has sent us.5
Overview of scale-up progress
In the sections below we discuss progress in each of the four provinces that VillageReach is working in. In this section, we summarize across all four provinces.
Data available
| Province | Last month for which we have information on whether distributions occurred6 | Last month for which we have information on stockouts | When we expect next report |
|---|---|---|---|
| Cabo Delgado | September 2012 | September 20127 | Q2 20138 |
| Niassa | September 2012 | February 20129 | May 201310 |
| Gaza | September 2012 | June 201211 | January 201312 |
| Maputo | September 2012 | July 201213 | May 201314 |
Regularity of distributions
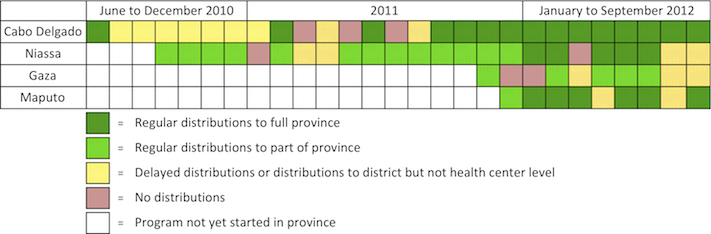
In recent months, the regularity of distributions in Cabo Delgado and Niassa provinces has improved. Distributions have started in Maputo province and part of Gaza province, where they occurred on or close to schedule in the first half of 2012 while experiencing some delays in July and August.
The following chart is our summary of the regularity of distributions of medical supplies in each province over the course of the project.15
Stockouts and quality monitoring
We continue to have limited data on stockouts. Stockouts appear to be fairly frequent in Cabo Delgado, Niassa, and Gaza, and less so in Maputo.
Aggregated data on stockouts by vaccine type across the four provinces indicates that stockouts of each vaccine were near the target of 10% or less of health centers in 2012 through September.16 We find it difficult to interpret this data because:
- We have not seen baseline stockout data from any province
- The program is at different stages in each province (for example, VillageReach started work in Cabo Delgado in June 2010 and in Maputo in December 2011)
- We would prefer to review disaggregated and raw data to determine whether the results are consistent across provinces
- We would also like to see data on "% of centers with at least one vaccine stockout," which was a key indicator in VillageReach's pilot project. This data was not included in the information VillageReach shared with us.
We asked VillageReach about the lack of the ‘at least one stockout’ chart in most of the evaluation reports we have seen, and it told us because of supply challenges with certain types of vaccines at higher distribution levels (national and provincial), the ‘at least one stockout’ chart fails to show improvements in stock levels for the vaccines that are available.17
VillageReach has conducted vaccine quality monitoring in each province, identified issues, and suggested improvements.
Cabo Delgado
Regularity of distributions
In our March 2012 update, we reported on VillageReach's summary of its one-year evaluation in Cabo Delgado (completed in September 2011), which found that distributions had been delayed or cancelled for a number of months due to lack of funds for the government's project activities. As a result of this finding, VillageReach decided to provide additional funding to cover costs incurred by the government. In its 18-month evaluation, which reports on progress since the one-year update, and is not yet public, VillageReach reports that distributions occurred regularly to most health units between September 2011 and February 2012.18 A later report indicates that distributions continued to occur regularly, with the exception of one month of distributions missed, through September 2012.19
Between November 2011 and June 2012, VillageReach shortened its scheduled involvement in Cabo Delgado. The June 2012 schedule indicates that VillageReach expected to transition from an implementation phase to a supervision phase in mid-2012 and then to an evaluation phase at the end of 2012.20 An earlier schedule, from November 2011, indicated that these transitions would take place six months later than that.21 In November 2012, VillageReach told us that it would extend its stay in the province until at least March 2013 (details below).
Stockouts and quality monitoring
VillageReach has provided stockout data from Cabo Delgado in two forms (this data is not yet public, and we are only able to provide general comments):
- The percentage of health centers with a stockout of at least one vaccine (for September to December 2011). VillageReach aims to reduce stockouts to under 5%; for the months since the regular distributions restarted for which we have seen data on this metric, the percentage of health centers with a stockout was consistently above this target.22
- Stockouts by vaccine (for July 2011 to September 2012). Supplies of two vaccines, the pentavalent vaccine and BCG, have been erratic, though seem to have improved since March 2012. Stockouts of the other three vaccines, polio, measles, and tetanus, remained fairly constant. VillageReach has met its target of 10% or less of health centers with a stockout of each of these three vaccines in most months since March 2012.23
We have requested data on stockouts since the start of the project, but have not yet received it. Stockouts were a key indicator tracked in VillageReach's pilot project.
In addition to vaccines, the distribution system has recently begun to deliver diagnostic tests to health centers. Stockouts of these diagnostic tests were fairly high in Cabo Delgado over the period July to December 2011.24
VillageReach's evaluation of the program's progress in Cabo Delgado (completed in February 2012) identifies concerns and provides suggestions on the quality of vaccination services.25 Problems noted include: a high percentage of refrigerators used to store vaccines have experienced problems, the supply of gas to power the refrigerators has been insufficient, and that data collection has not been standardized.26
VillageReach reports that refrigerator performance improved in 2012 and it consistently reached its target of 95% or more of health centers with functioning refrigerators through September 2012.27
Niassa
Regularity of distributions
VillageReach reports that between August 2010, when distributions began in part of the province, and March 2012, when its most recent monitoring report on the province was completed, regular distributions have occurred in all but four months.28 VillageReach also reports, however, that the interval between distributions averaged 58 days between July 2011 and February 2012 (the dates for which we've seen data).29 VillageReach told us this "is skewed by provinces experiencing infrequent distributions (e.g. multiple months)."30 Over the same period, VilllageReach reports that an average 33% of health centers were visited each month.31 A later report on the program as a whole notes that there have been "80% of distributions in past 12 months" in Niassa and "limited and/or no distributions in March, July, and August [of 2012] due to insufficient functioning vehicles available."32
In January 2012, distributions were expanded from 6 to all 16
districts in the province.33
VillageReach is currently supporting some of the government’s program costs, such as fuel and staff per diems (more on this issue in a previous update).34
Stockouts and quality monitoring
This data is not yet public, and we are only able to provide general comments.
VillageReach reports '% of health centers with at least one stockout,' for July 2011 to February 2012, in its 18-month evaluation report on Niassa. VillageReach reports that stockouts were consistently above the target of less than 5% of health centers with a stockout of any vaccine each month. VillageReach concludes, "The distributions are regular, but stock outs continue to be high."35 (Note that the first version of this chart we received was copied from the Cabo Delgado report. VillageReach sent us a corrected version when we noted this issue. More discussion of this issue above).
In its chart of 'stockouts by vaccine,' VillageReach reports that, for four of five vaccines, Niassa was close to its target of less than 10% of health centers experiencing a stockout. Stockouts of the fifth vaccine were more frequent.
VillageReach told us that between March and September 2012 the incidence of stockouts in Niassa was about 10% (we have not seen this data).36
The evaluation also identifies concerns and provides suggestions on the quality of vaccination services. Problems noted include: staff failing to monitor refrigerator temperatures and falsifying temperature data, damaged refrigerators, and poor waste management.37 As in Cabo Delgado, a fairly high percentage of refrigerators used to store vaccines are not functioning correctly.38
Gaza
Regularity of distributions
Distributions in Gaza started in November 2011, but did not occur in December 2011 or January 2012; VillageReach reports that there have been regular distributions to the southern part of the province in February to June 2012, with a distribution delay in March 2012.39 Distributions were delayed in July 2012 and only half of the southern part of the province received distributions in August.40 VillageReach has paid for some fuel and all per diems in the province since the start of distributions (more on this issue in a previous update).41
As of September 2012, there have been no distributions to the northern part of the province. VillageReach told us, “Currently there are no plans for expansion to the north because there are no funds for it… Reaching the remaining 27% of the health centers (in the north) has the same cost as reaching the 73% in the south because the north is geographically large with a very small population.”42
Stockouts and quality monitoring
VillageReach shared its 6-month evaluation of the program in Gaza with us; the report is not yet public. Like the most recent Cabo Delgado report, the 6-month Gaza evaluation identifies concerns and provides suggestions on the quality of vaccination services.43 As in Cabo Delgado, a high percentage of refrigerators used to store vaccines are not functioning correctly (and data is missing on refrigerator issues for four months between November 2011 and June 2012).44 Another funder plans to replace a number of health center refrigerators in Gaza (the timeline for this is not specified).45
The evaluation report does not contain a chart of the key stockout indicator used in VillageReach’s pilot project: '% of health centers with at least one vaccine stockout.' It does contain a chart on '% of stockouts by vaccine,' though data is missing for three of the eight months shown (two months in which there were no distributions and the month in which distributions were delayed).46
Baseline data collection
VillageReach is not planning to conduct its own baseline vaccination rate survey in Gaza. To evaluate progress on vaccination rates, it will rely on a 2010 survey conducted by the provincial government (which it told us it is not able to share), and the 2011 Demographic and Health Survey (DHS).47 According to the preliminary report on the 2011 DHS, 76.3% of children between the ages of 12 and 23 months have received all basic vaccinations and 89.0% have received the third DPT vaccination, a commonly used indicator of "vaccination coverage."48 We note that Gaza has fairly high baseline vaccination coverage; for comparison, the baseline rate of coverage for the third DPT vaccination for VillageReach's pilot project in Cabo Delgado was 68.9%.49
Completion of the baseline health center survey and cost study in Gaza has been delayed and the reports were, as of August 2012, expected in early November. VillageReach notes that these will not be public until after the endline studies.50
Maputo
Regularity of distributions
Distributions in Maputo province began in December 2011. VillageReach reports that distributions occurred regularly though September 2012,51 with the exception that in April, supplies were delivered to the district level in two districts rather than to the health centers.52
Stockouts and quality monitoring
We have not seen stockout data for the province. VillageReach noted as part of its monitoring visits to a sample of health centers, "Of the 16 health units visited in the last 3 months, none recorded stockouts of vaccines (except Nwamatibjana health center, which lacked BCG for 4 days due to weak coordination with SDMAS-vaccines provided by CISM)."53
As in other provinces, VillageReach visited health centers to monitor the program and suggest improvements. Issues identified include lack of information given to mothers at the time of vaccination, a staff person being unavailable to perform his duties, and some weak data quality.54
Baseline data collection
Completion of the baseline health center survey in Maputo has been delayed. As of September 2012, the report was expected in early November.55 VillageReach notes that this will not be public until after the endline survey.56
Room for more funding as of late 2012
VillageReach has reduced both its budget for the Mozambique project and its revenue projection. In September 2012, VillageReach told us it had a funding gap for 2013, but due to changes since that time, we do not have clear understanding of VillageReach's current funding gap.
Expected expenses
Since our last update in March 2012, VillageReach has decreased its expected budget for the Mozambique project for FY2012-2015 by $1.41 million (from $4.04 million to $2.63 million). Changes include:57
- An overall decrease in core costs (costs of running the program at the central level within Mozambique) of $483,000, from $1.67 million to $1.18 million. VillageReach told us that this decrease will be largely achieved by reallocating staff time to contract projects (projects that VillageReach is hired to complete for other organizations) and projects funded by restricted grants from foundations, including both time spent searching for new funding sources and implementing funded projects.58
- Exiting from Cabo Delgado and Niassa provinces sooner than originally planned. This accounts for $395,000 of the budget decrease. VillageReach planned to leave Cabo Delgado and Niassa in mid to late 2013. In September 2012, it told us that it would leave the provinces early, by the end of 2012, in part due to lack of funding.59 In October 2012, VillageReach decided to extend its work in the two provinces until at least March 2013. It recently began discussions with a funder who is interested in funding VillageReach's work in these provinces and VillageReach has decided to postpone its exit until it can complete these discussions.60
- Decreases in expected costs in Gaza and Maputo, accounting for $315,000 of the budget decrease. The decrease in Gaza may be due to the decision not to extend the program into the northern part of the country (see above). We do not know the cause of the cost decreases in Maputo. VillageReach previously expected to exit the provinces in FY2014; it now expects to extend the programs into FY2015, but it has significantly reduced its budget for FY2014 in the provinces from $320,000 to $126,000.
- A reduction in the amount of “indirect” costs allocated to the program by $218,000, from $834,000 to $616,000. These are costs incurred at headquarters level. It is our impression that this change is primarily an accounting change in which general costs that were previously allocated to the Mozambique project are no longer allocated to it.61
Expected revenues
In September 2012, VillageReach projected revenues available for the Mozambique project of $325,000, $200,000 and $150,000 in each FY2013-2015. This includes unrestricted funding (56%) and funding from a foundation restricted to the Mozambique project (44%).62 In October 2012, VillageReach entered discussions with a potential new funder for the program.63
VillageReach's projection for future revenues available for the Mozambique project are lower than what we previously expected. In our previous projections, we assumed that VillageReach would receive $850,000 per year in 2013 and 2014 in unrestricted and Mozambique-restricted revenues, $410,000 of which would be used to fund operational costs that are not included in the Mozambique budget (estimates were provided by VillageReach at the start of the project), leaving $440,000 per year available to support the Mozambique project.64
In FY2012, VillageReach raised $960,000 in unrestricted funding and Mozambique-restricted funding,65 exceeding expectations by $110,000.
Assuming the same level of operational costs that we have in previous estimates, VillageReach's most recent projections would imply that it believes it will raise $735,000, $610,000, and $560,000 in unrestricted and Mozambique-restricted funds in the next three years, respectively.66 We are not confident in our understanding of why VillageReach’s total projected revenue for Mozambique (including both restricted and unrestricted funds) is now substantially lower than it was previously. Possibilities include:
- VillageReach's now expects its operational costs (not allocated to the Mozambique project) to be greater than $410,000 per year (the estimate they provided at the start of the project).
- VillageReach now has reason to believe that unrestricted and Mozambique-restricted revenues will be significantly lower in future years than they have been in the past.
- VillageReach now expects to allocate some unrestricted funding to projects other than the Mozambique project.
Our best guess about what did occur, based on conversations with VillageReach, is that #3 the primary explanation: it intended to start up the project with unrestricted funds and to raise restricted grants from foundations to continue and expand the project. It has found that foundations are not as interested as expected in supporting the project, and VillageReach has decided that it is not wise to continue putting all of its unrestricted funding into a project that is unlikely to result in future revenue growth.
A possible alternative use of unrestricted funds is support for a project in Malawi, announced in September 2012, for which VillageReach needs to raise about $500,000 to supplement a foundation grant of about $1.5 million.67
For full data on how our view of VillageReach's funding gap has changed over time, see this spreadsheet.
Funding gap
We do not have a current estimate of VillageReach's funding gap. In September 2012, VillageReach estimated that it had a funding gap for the Mozambique project of $552,000, including a funding gap of $228,000 in FY2013 (which ends in September 2013).68 Since September 2012, it has extended its work in Cabo Delgado and Niassa by three months, increasing the budget by about $145,000,69 and entered into discussions with a potential funder about further extending its work in these provinces.70 We understand that there is no guarantee of support from this funder. We have elected not to fully investigate VillageReach's funding gap and cannot provide a specific estimate at this time.
Summary of our funding gap estimates over time
For details of how our funding gap estimates have changed over time, see this spreadsheet.
Sources
- Beale, John. VillageReach Director of Strategic Development. Email to GiveWell, August 30, 2012.
- Beale, John. VillageReach Director of Strategic Development. Email to GiveWell, September 18, 2012.
- Beale, John. VillageReach Director of Strategic Development. Email to GiveWell, November 6, 2012.
- Beale, John. VillageReach Director of Strategic Development. Email to GiveWell, November 26, 2012.
- Beale, John. VillageReach Director of Strategic Development. Email to GiveWell, December 19, 2012.
- Beale, John. VillageReach Director of Strategic Development. Phone conversation with GiveWell, September 12, 2012.
- GiveWell. Changes in VillageReach budget (November 2011 to October 2012).
- GiveWell. Changes in expected Mozambique costs and revenues over time (XLS).
- GiveWell. Summary of regularity of distributions (XLS).
- Mozambique National Institute of Statistics. Demographic and health survey (2011; preliminary report) (PDF).
- VillageReach. Funding requirements for VillageReach Mozambique DLS program (September 2012). VillageReach asked us to keep this document confidential.
- VillageReach. Health system strengthening in Mozambique: Update (November 2011) (PDF).
- VillageReach. Health system strengthening in Mozambique: Update (June 2012) (PDF).
- VillageReach. Health system strengthening in Mozambique: Update (October 2012) (PDF).
- VillageReach. Mozambique budget with GiveWell additions (November 2011, updated February 2012) (XLS).
- VillageReach. Mozambique Dedicated Logistics System performance report: All provinces (January to September 2012). VillageReach asked us to keep this document confidential.
- VillageReach. Mozambique Dedicated Logistics System performance report: Cabo Delgado (July to December 2012). VillageReach asked us to keep this document confidential.
- VillageReach. Mozambique Dedicated Logistics System performance report: Cabo Delgado (January to September 2012). VillageReach asked us to keep this document confidential.
- VillageReach. Mozambique evaluation schedule (September 2012). VillageReach asked us to keep this document confidential.
- VillageReach. Support to PAV – 18-month evaluation: Cabo Delgado. VillageReach asked us to keep this document confidential.
- VillageReach. Support to PAV – 6-month evaluation: Gaza. VillageReach asked us to keep this document confidential.
- VillageReach. Support to PAV – 6-month evaluation: Maputo (August 2012). VillageReach asked us to keep this document confidential.
- VillageReach. Support to PAV – 18-month evaluation: Niassa (April 2012). VillageReach asked us to keep this document confidential.
- VillageReach. Tentative schedule for VillageReach evaluation activities (January 2012) (PDF).
- VillageReach. The Barr Foundation and VillageReach announce new program to improve supply chain for essential medicines (PDF).
- 1
"VillageReach initially envisioned that DPS authorities in each province would effectively take over responsibility for the operation of the DLS after a period of one or two years… We are now less confident of seeing this phase realized in each of the provinces, owing primarily to the significant funding challenges, insufficient transportation available, and overloaded human resources we have seen the government experiencing." VillageReach, "Health System Strengthening in Mozambique: Update (October 2012)," Pgs 19-20.
- 2
In our August 2011 update on VillageReach, we estimated that VillageReach had a funding gap of $965,000. This estimate included an assumption that VillageReach would receive $850,000 in each FY2012-2015 and have $410,000 worth of costs that were both (a) not included in the Mozambique project budget; and (b) funded with unrestricted funds. In our March 2012 update on VillageReach, we estimated that VillageReach had a funding gap of $1.435 million. This funding gap estimate included the same assumptions about annual unrestricted revenues and annual non-Mozambique project costs. However, because VillageReach had revised its project plan to end the project in FY2014 instead of FY2015, of this increase, $440,000 ($850,000 less in revenues minus $410,000 less in costs) was due to the project ending in FY2014 instead of FY2015. If we exclude the change due to the length of the project plan (which in practically may have little effect on the funding VillageReach is able to allocate to the project), the overall funding gap increased by about $30,000 ($965,000 in the earlier estimate and $1.435 million minus $440,000, or about $995,000 in the later estimate).
- 3
The version of Niassa 18-month evaluation that we received from VillageReach in November contained two stockout charts: one of health centers with 'at least one vaccine stockout' (Pg 18) and one of health centers with a stockout of each type of vaccine. The two charts are not consistent with one another (e.g. in one month there were more centers reported to have experienced a stockout of a particular vaccine than centers with at least one vaccine stockout). When we asked VillageReach about this, it told us, "The discrepancy in Niassa data reflects a delay in all of the data being inputted into vrMIS, in the first case, after which an update was made" (John Beale, email to GiveWell, November 26, 2012). We later realized that the chart for 'at least one vaccine stockout' was identical to the one in the Cabo Delgado 18-month evaluation report. We believe this was copied from the Cabo Delgado report.
- 4
"I have attached a corrected version of the Niassa 18-month report, with an updated slide 18. In the previous version of the presentation deck, the slide was indeed copied from the Cabo Delgado report - apparently during the translation process - and wasn't picked up during final editing." John Beale, email to GiveWell, December 19, 2012.
- 5
- 6VillageReach, "Health system strengthening in Mozambique: Update (October 2012)."
- 7VillageReach, "Mozambique Dedicated Logistics System Performance Report: Cabo Delgado (January to September 2012)."
- 8Comments on update attached to John Beale, email to GiveWell, November 26, 2012.
- 9VillageReach, "Support to PAV – 18-Month Evaluation: Niassa (April 2012)," Pg 19.
- 10Reports are expected every 6 months (VillageReach, "Tentative schedule for VillageReach evaluation activities (January 2012).") We received the most recent report in November 2012.
- 11VillageReach, "Support to PAV – 6-Month Evaluation: Gaza." pg 12
- 12VillageReach, "Tentative schedule for VillageReach evaluation activities (January 2012)."
- 13VillageReach, "Support to PAV – 6-Month Evaluation: Maputo (August 2012)," Pg 11.
- 14Reports are expected every 6 months (VillageReach, "Tentative schedule for VillageReach evaluation activities (January 2012)."). We received the most recent report in November 2012.
- 15
GiveWell, "Summary of Regularity of Distributions."
- 16
VillageReach, "Mozambique Dedicated Logistics System Performance Report: All Provinces (January to September 2012)."
- 17
“Reporting stock outs by vaccine type is more actionable data for the audience of this evaluation. Note that in the pilot project when we selected this indicator, the upstream supply of vaccines was fine but now there are problems with the upstream supply. That meant that it was a good indicator of the DLS [VillageReach’s project] performance. However, now that indicator is not a good indicator of DLS performance, but looking by vaccine type is a better indicator because we can mentally take out those vaccines with upstream supply problems.” John Beale, email to GiveWell, September 18, 2012.
- 18
Table indicates that there were "distribution[s] to the health unit level with VillageReach support," in each September 2011 through February 2012. VillageReach, "Support to PAV – 18-Month Evaluation: Cabo Delgado," Pg 5.
- 19
"92% distributions for past 12 months. One month was missed due to an accumulation of several months with delays in accessing funding." VillageReach, "Health System Strengthening in Mozambique: Update (October 2012)," Pg 19.
- 20
VillageReach, "Health System Strengthening in Mozambique: Update (June 2012)," Pg 9.
- 21
VillageReach, "Health System Strengthening in Mozambique: Update (November 2011)," Pg 10.
- 22
VillageReach, "Support to PAV – 18-Month Evaluation: Cabo Delgado," Pg 16.
- 23
VillageReach, "Mozambique Dedicated Logistics System Performance Report: Cabo Delgado (July to December 2012)."
VillageReach, "Mozambique Dedicated Logistics System Performance Report: Cabo Delgado (January to September 2012)."
- 24
VillageReach, "Support to PAV – 18-Month Evaluation: Cabo Delgado," Pg 21.
- 25
For the evaluation, VillageReach staff visited 8 health centers and rated on quality of vaccine distribution, refrigeration control, syringe disposal, injection safety, data collection & management, equipment management, waste management, and sanitation & hygiene. VillageReach, "Support to PAV – 18-Month Evaluation: Cabo Delgado," Pg 7.
Also noted, "BCG and Measles vaccination sessions were conducted only 1 or 2 times per week (Monday and/or Friday) in all the health posts visited due to fears of wastage and reduced quantities of these vaccine. For births that occur in or out of the maternity ward, infants are not receiving vaccinations unless at least 9 infants show up for vaccination. Some mothers who travelled more than 15 km for vaccination were told to return home without vaccination because the day they gave birth or because the day of their visit was outside the 'instituted' days for vaccination." VillageReach, "Support to PAV – 18-Month Evaluation: Cabo Delgado," Pg 8.
- 26
VillageReach, "Support to PAV – 18-Month Evaluation: Cabo Delgado," Pg 10, Pg 13.
- 27
VillageReach, "Mozambique Dedicated Logistics System Performance Report: Cabo Delgado (January to September 2012)." Pg 2
- 28
VillageReach, "Support to PAV – 18-Month Evaluation: Niassa (April 2012)," Pg 6.
- 29
VillageReach, "Support to PAV – 18-Month Evaluation: Niassa (April 2012)," Pg 21.
- 30
John Beale, email to GiveWell, December 19, 2012.
- 31
VillageReach, "Support to PAV – 18-Month Evaluation: Niassa (April 2012)," Pg 17.
- 32
VillageReach, "Health System Strengthening in Mozambique: Update (October 2012)," Pg 19.
- 33
"Niassa: January 2012 – expansion of distributions to all 16 districts; 92% distributions for 12 months." VillageReach, “Health System Strengthening in Mozambique: Update (June 2012),” Pg 18.
Previous situation described in an earlier update. - 34
John Beale, phone conversation with GiveWell, September 12, 2012.
- 35
VillageReach, "Support to PAV – 18-Month Evaluation: Niassa (April 2012)," Pg 18.
- 36
Comments on update attached to John Beale, email to GiveWell, November 26, 2012.
- 37
VillageReach, "Support to PAV – 18-Month Evaluation: Niassa (April 2012)," Pgs 8-9.
- 38
VillageReach, "Support to PAV – 18-Month Evaluation: Niassa (April 2012)," Pg 20.
- 39
VillageReach, "Support to PAV – 6-Month Evaluation: Gaza," Pg 5.
- 40
VillageReach, "Health System Strengthening in Mozambique: Update (October 2012)," Pg 19.
- 41
"VillageReach covered fuel and per diem costs for vaccine distribution to the health unit level from November 2011 to June 2012." VillageReach, "Support to PAV – 6-Month Evaluation: Gaza," Pg 3.
VillageReach clarified that it had paid for some fuel and all per diems. John Beale, email to GiveWell, November 26, 2012. - 42
John Beale, email to GiveWell, September 18, 2012.
- 43
For the evaluation, VillageReach staff visited 11 health centers and rated each health center on quality of vaccine distribution, refrigeration control, syringe disposal, data collection & management, equipment management, waste management, and sanitation & hygiene.
VillageReach, "Support to PAV – 6-Month Evaluation: Gaza," Pg 7.
- 44
VillageReach, "Support to PAV – 6-Month Evaluation: Gaza," Pg 13.
Also noted, "In almost all the districts, there is insufficient control of the PAV refrigerator temperature, with greater problems on weekends and holidays. There is a tendency to corrupt/invalidate the temperature records." VillageReach, "Support to PAV – 6-Month Evaluation: Gaza," Pg 10.
- 45
“It was learned that most health units are going to be given new refrigerators distributed by the Energy Fund (FUNAE).” VillageReach, "Support to PAV – 6-Month Evaluation: Gaza," Pg 13.
- 46
VillageReach, "Support to PAV – 6-Month Evaluation: Gaza," Pg 12.
- 47
John Beale, email to GiveWell, August 30, 2012.
- 48
Mozambique National Institute of Statistics, "Demographic and Health Survey (2011; preliminary report)," Pg 14.
- 49
See our review of VillageReach, chart "Figure 2-3: Coverage across Time and Location: DTP 3 (3 doses of DTP)."
- 50
John Beale, email to GiveWell, August 30, 2012.
- 51
VillageReach, "Health System Strengthening in Mozambique: Update (October 2012)," Pg 19.
- 52
VillageReach, "Support to PAV – 6-Month Evaluation: Maputo (August 2012)," Pg 5.
- 53
VillageReach, "Support to PAV – 6-Month Evaluation: Maputo (August 2012)," Pg 11.
- 54
VillageReach, "Support to PAV – 6-Month Evaluation: Maputo (August 2012)," Pgs 14 and 19.
- 55
VillageReach, “Mozambique Evaluation Schedule (September 2012).”
- 56
John Beale, email to GiveWell, August 30, 2012.
- 57
GiveWell, "Changes in VillageReach Budget (November 2011 to October 2012)." Data in this document is from:
VillageReach, "Health System Strengthening in Mozambique: Update (November 2011)," Pg 13.
VillageReach, "Health System Strengthening in Mozambique: Update (October 2012)," Pg 12. - 58
John Beale, phone conversation with GiveWell, September 12, 2012.
- 59
John Beale, phone conversation with GiveWell, September 12, 2012.
- 60
"As for the potential new funder for the Mozambique, the updated budget in the narrative reflects the status of discussions with them to date. The funder has expressed interest in seeing us remain active in all four provinces (not closing down Cabo Delgado and Niassa), but we do not expect to have a signed agreement before early next year. We have therefore decided to maintain the program for all provinces using our own resources, as we have been to date. As a result the updated budget shows additional expense that we will incur for core costs, Cabo Delgado and Niassa through the end of March 2013." John Beale, email to GiveWell, November 6, 2012.
- 61
John Beale, phone conversation with GiveWell, September 12, 2012.
- 62
VillageReach, “Funding Requirements for VillageReach Mozambique DLS Program (September 2012).”
- 63
"As for the potential new funder for the Mozambique, the updated budget in the narrative reflects the status of discussions with them to date. The funder has expressed interest in seeing us remain active in all four provinces (not closing down Cabo Delgado and Niassa), but we do not expect to have a signed agreement before early next year." John Beale, email to GiveWell, November 6, 2012.
- 64
VillageReach, "Mozambique Budget with GiveWell Additions (November 2011, Updated February 2012)." See Cells E17, F17, E11, and F11.
- 65
VillageReach, “Funding Requirements for VillageReach Mozambique DLS Program (September 2012),” Sheet VillageReach 2012.
- 66
Adding $410,000 to each $325,000, $200,000 and $150,000, VillageReach's projected revenues available for the Mozambique project in each FY2013-2015.
- 67
"The Barr Foundation will provide approximately 75% of the financial support for
the $2 million initiative. VillageReach is seeking additional funders to join the project." VillageReach, "The Barr Foundation and VillageReach Announce New Program to Improve Supply Chain for Essential Medicines." - 68
VillageReach, "Funding Requirements for VillageReach Mozambique DLS Program (September 2012)," Sheet Moz DLS.
- 69
Total budget as of June 2012: $4,063,674. VillageReach, "Health System Strengthening in Mozambique: Update (June 2012)," Pg 12
Total budget as of October 2012: $4,208,640. VillageReach, "Health system strengthening in Mozambique: Update (October 2012)," Pg 12.
- 70
John Beale, email to GiveWell, November 6, 2012.