Summary
- We are aware of three organizations that estimate malaria mortality rates. All of them seem to agree that roughly 25% of all malaria mortality in sub-Saharan Africa occurs among individuals 5+ years old. (For simplicity, throughout this write up we refer to individuals 5 years old and over as "5-and-overs.")
- We believe that the mechanism by which bed nets would reduce malaria mortality among 5-and-overs is straightforward and plausible: bed nets would reduce malaria cases in this group, which would in turn reduce deaths. We checked this reasoning with three malaria researchers, and they agreed with this assessment.
- We are not aware of any randomized controlled trials (RCTs) that estimate the impact of bed nets on 5-and-over mortality. We have seen one RCT that finds that bed nets reduce 5-and-over malaria episodes. The malaria researchers we spoke to told us that they did not believe there was additional research we missed that directly addresses this question.
- Given the above, our best guess is that reducing malaria mortality among 5-and-overs is a meaningful impact of bed net distributions, but due to a lack of relevant evidence we are forced to make a variety of judgment calls when estimating the magnitude of this impact in our cost-effectiveness analysis (CEA) (see our CEA for more details).
Published: December 2017
Table of Contents
Malaria mortality rates among 5-and-overs
Our best guess based on the available data is that roughly 25% of all malaria mortality in sub-Saharan Africa occurs among individuals 5+ years old.
We are aware of three organizations or projects that estimate malaria mortality rates: the World Health Organization (WHO), the Global Burden of Disease (GBD) study (published by the Institute for Health Metrics and Evaluation (IHME)), and the Malaria Atlas Project (MAP).1
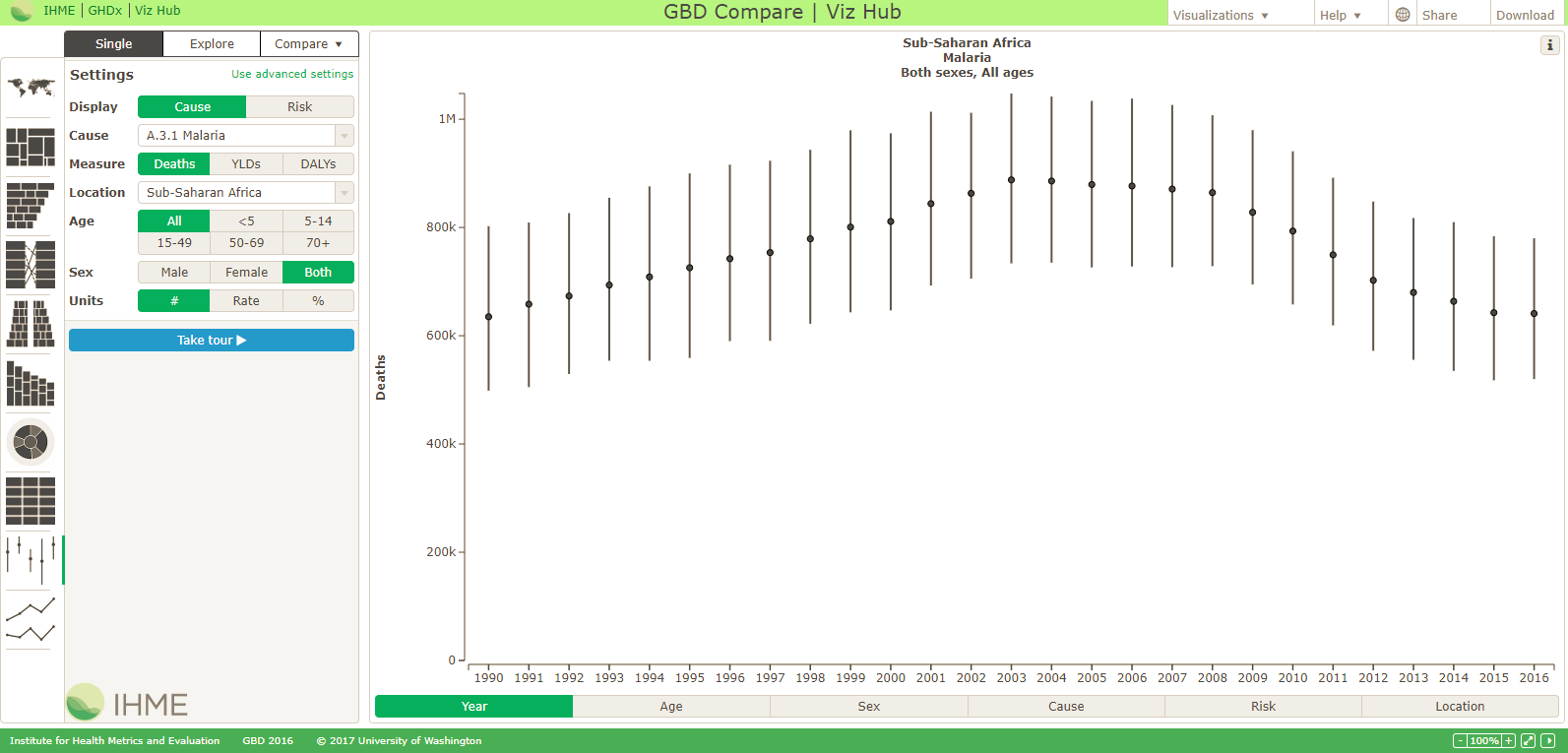
All three provide estimates of overall malaria mortality rates in sub-Saharan Africa. The WHO estimated that there were about 390,000 malaria deaths in the WHO African region in 2015 while MAP and GBD estimated about 630,000 malaria deaths in sub-Saharan Africa in a similar time period.2 We have not closely investigated what causes the variation in these mortality estimates, though it is worth noting that the confidence intervals for each group's estimates are wide and overlapping.
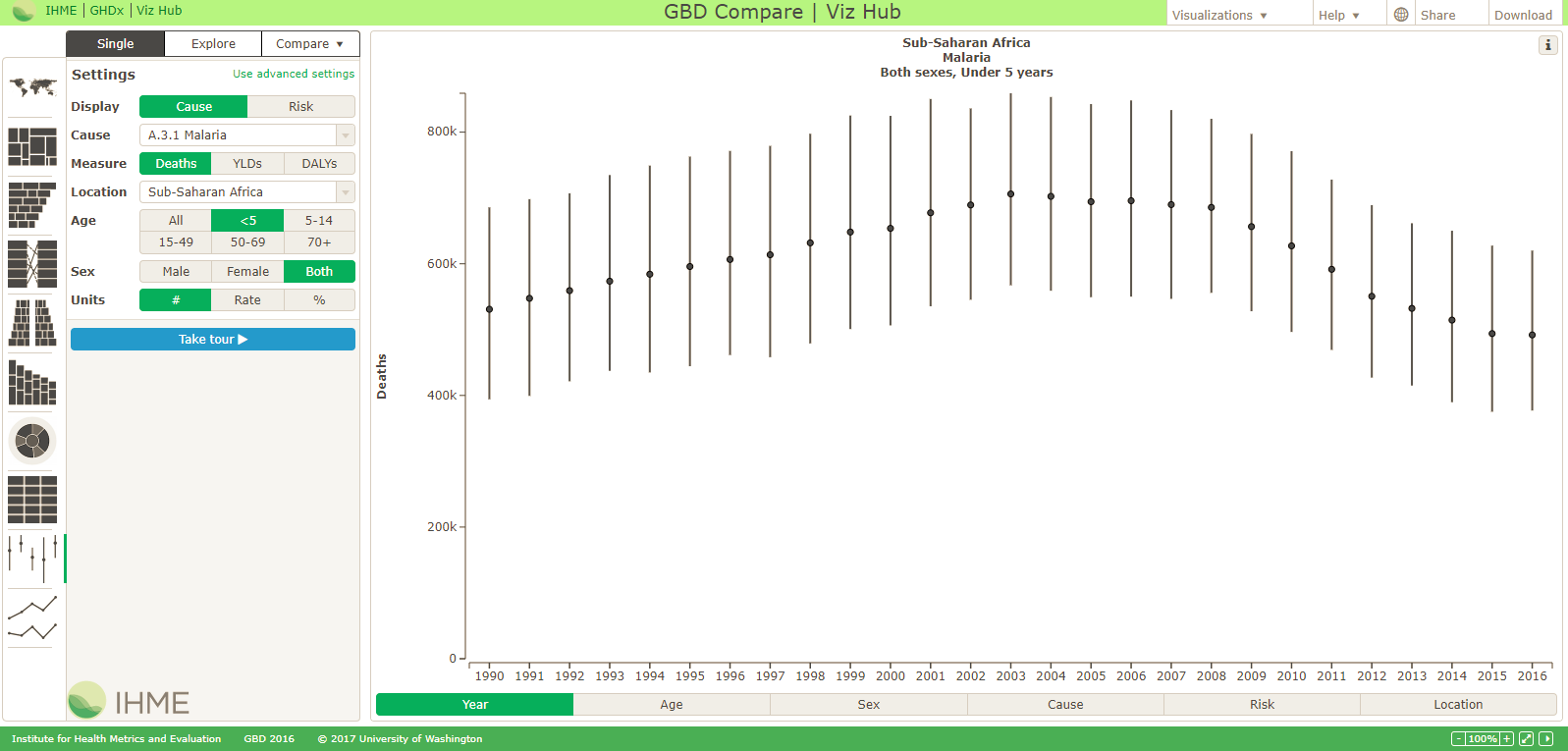
Regarding what portion of malaria deaths occur in children under 5 years old in sub-Saharan Africa, it appears that all three groups have similar estimates as of 2015-2016: that about 73-77% of malaria deaths in sub-Saharan Africa occur in children under 5 years old.3 Therefore, about 25% of deaths are estimated to occur in 5-and-overs (see previous footnote for details). Since these estimates are all fairly similar to each other, we have not deeply investigated the underlying methods used to generate them.
As of 2011, there were larger differences in the estimates of 5-and-over malaria mortality between GBD and the WHO; we do not know what led the estimates to converge.4
Connection between bed net coverage and malaria mortality in 5-and-overs
Our best guess is that reducing malaria mortality among 5-and-overs is a meaningful impact of bed net distributions. The mechanism by which bed nets would reduce malaria mortality among 5-and-overs is straightforward and plausible, and the only relevant empirical evidence we are aware of (one RCT that studied the impact of bed nets on adult malaria case rates) is consistent with this theory. However, we must make a variety of judgment calls to estimate the magnitude of this impact in our CEA for the Against Malaria Foundation (AMF).
Mechanism
We believe that the mechanism by which bed nets would reduce 5-and-over malaria mortality is straightforward: bed nets likely reduce malaria cases in 5-and-overs which likely reduces malaria deaths. The malaria researchers that we spoke to agreed that bed nets likely had some effect on 5-and-over malaria mortality due to the plausibility of this mechanism.5
Relevant evidence
We are not aware of any RCTs that estimate the impact of bed nets on 5-and-over mortality. We have seen one RCT that finds that bed nets reduce 5-and-over malaria episodes. The malaria researchers we spoke to told us that they did not believe there was additional research we missed that directly addresses this question.6
The only relevant RCT that we have seen on this topic (Kamol-Ratanakul and Prasittisuk 1992) found that insecticide-treated bed nets reduced malaria episodes in adults by roughly 30-40% relative to a control group that received untreated nets, which was a statistically significant result.7 However, there are a number of limitations in applying this study to AMF's work, including:
- The study sample size was fairly small (261 total subjects), which may increase the potential for error.
- The bed nets were distributed in eastern Thailand to a population of migrant workers prior to 1992; effects of bed nets in that context may be different from effects of universal distributions in sub-Saharan Africa today.
- The study compared insecticide-treated nets against untreated nets, which may underestimate the impact of receiving a bed net from an AMF distribution (where the counterfactual may be not receiving a net at all).
The malaria researchers that we spoke to told us that this topic is not well studied. It may be impractical and expensive to collect large enough sample sizes to detect a statistically significant effect of nets on 5-and-over mortality, among other challenges.8
Other factors that could affect cost-effectiveness analysis
A few factors which may lead to a lower protective efficacy for 5-and-overs than exists for children under 5 are:
- Older individuals may go to sleep later in the day than young children. As a result, adults may be less likely to be under bed nets during the hours when mosquitoes are most likely to bite.9
- Older individuals likely have had more exposure to malaria in the past, so would be expected to have greater immunity and hence lower case fatality rates.10 However, even if 5-and-overs face a lower absolute risk of acquiring symptomatic malaria, we do not know of any reasons why the relative risk reduction (i.e., the percentage reduction in malaria cases due to bed net coverage) would be lower in 5-and-overs due to different immunity levels.
- Older individuals may be less likely than young children to sleep under bed nets they receive. Perhaps adults know they are less likely to acquire malaria so have less of an incentive to sleep under nets.11
We have not investigated the extent to which the above factors would lead to lower protective efficacy among 5-and-overs.
See the following footnote for additional details on how we incorporate 5-and-over malaria mortality into our CEA.12
Process
To inform our estimate of malaria mortality rates among 5-and-overs, we:
- Reviewed mortality estimates from three organizations or projects (discussed above): the World Health Organization, Global Burden of Disease study, and Malaria Atlas Project.
- Spoke with three individuals from the above organizations to better understand the general methodology behind their mortality estimates for 5-and-overs. We did not receive permission to publish notes from these conversations.
To better understand the connection between bed net coverage and malaria mortality in 5-and-overs, we:
- Spoke with three malaria researchers about this topic and published conversation notes:
- Conducted a review of relevant literature. To identify relevant literature, we:
- Reviewed RCTs of bed net distributions (e.g., RCTs cited in our intervention report on bed nets) to see whether any of them recorded effects on adult case rates or adult mortality rates.
- Ran a large number of Google Scholar searches with queries using different combinations of the following keywords: "malaria," "insecticide treated nets," "adults," "case rates," "age 5 and over."
- Asked malaria researchers whether they were aware of literature discussing the relationship between bed net coverage and 5-and-over malaria mortality or case rates.
Sources
{kind=link}
{kind=link}
- 1
See:
- 2
- Overall estimates of malaria mortality in sub-Saharan Africa (or WHO African region) in 2015 or 2016 by organization:
- WHO:
- Total malaria deaths (2015, WHO African region): about 394,000
- Malaria deaths among children under 5 (2015, WHO African region): about 292,000
- Malaria deaths among people 5 and over (2015, WHO African region): about 102,000
- Source: Table 6.4, Pg. 43, WHO, World Malaria Report 2016 provides estimates of the number of malaria deaths, including in children under 5 years old, by region of the world for 2015. Estimated total deaths in WHO African Region: 394,000 (95% CI: 230,000 to 549,000). Estimated deaths <5 years in African region: 292,000 (95% CI: 171,000 to 408,000). So, the estimated % of deaths in children <5 years old in the African region is about 74% (292,000 / 394,000 = about 74.11%). See Pg. 43, WHO, World Malaria Report 2016
.
- GBD:
- Total malaria deaths (2016, sub-Saharan Africa): about 641,000
- Malaria deaths among children under 5 (2016, sub-Saharan Africa): about 492,000
- Malaria deaths among people 5 and over (2016, sub-Saharan Africa): about 149,000
- Source: See GBD-Compare tool figures: GBD-Compare, overall malaria mortality estimate, sub-Saharan Africa, 2016 and GBD-Compare, under-5 year old malaria mortality estimate, sub-Saharan Africa, 2016. This implies that about 77% of malaria deaths were in children under 5 years old (492,000 / 641,000 = about 76.76%).
- MAP:
- Total malaria deaths (2015, sub-Saharan Africa): about 631,000
- Malaria deaths among children under 5 (2015, sub-Saharan Africa): about 464,000
- Malaria deaths among people 5 and over (2015, sub-Saharan Africa): about 167,000
- Source:
- "Across sub-Saharan Africa during the past 15 years, we estimated that there was an overall decrease of 57% (95% uncertainty interval, 46 to 65) in the rate of malaria deaths, from 12.5 (95% uncertainty interval, 8.3 to 17.0) per 10,000 population in 2000 to 5.4 (95% uncertainty interval, 3.4 to 7.9) in 2015. This led to an overall decrease of 37% (95% uncertainty interval, 36 to 39) in the number of malaria deaths annually, from 1,007,000 (95% uncertainty interval, 666,000 to 1,376,000) to 631,000 (95% uncertainty interval, 394,000 to 914,000). The share of malaria deaths among children younger than 5 years of age ranged from more than 80% at a rate of death of more than 25 per 10,000 to less than 40% at rates below 1 per 10,000. Areas with high malaria mortality (>10 per 10,000) and low coverage (<50%) of insecticide-treated bed nets and antimalarial drugs included much of Nigeria, Angola, and Cameroon and parts of the Central African Republic, Congo, Guinea, and Equatorial Guinea." Pg. 2435, Gething et al. 2016
- "As transmission declined between 2000 and 2015, the share of annual malaria deaths in children 4 years of age or younger and in those 5 to 14 years of age decreased (from 78.7% to 73.5% and from 6.7% to 4.8%, respectively), and the share in persons 15 years of age or older increased (from 14.6% to 21.7%). An expanded set of mapped estimates according to age group and year is provided in Figs. S2 and S3 in the Supplementary Appendix." Pg. 2442, Gething et al. 2016
- WHO:
- Historically (e.g. in 2011), the GBD study (published by IHME) estimated about 8x more malaria mortality among those over age five in Africa than the WHO did (see below). As of the 2015-2016 estimates, it appears that GBD estimated about 149,000 malaria deaths among people 5-and-over as compared to the roughly 102,000 deaths estimated by WHO (see above), a much smaller discrepancy. We do not know what led to this convergence, though it appears both that WHO's estimate has roughly doubled (from about 55,000 deaths to about 102,000 deaths) while GBD's estimate fell by about 3x (from about 435,000 deaths to about 149,000 deaths).
- "4. How do the IHME findings published in February 2012 compare to the findings of WHO's World Malaria Report 2011?
The IHME study entitled "Global malaria mortality between 1980 and 2010: a systematic analysis" published in the Lancet on 3 February 2012 raised many questions about the differences between malaria burden estimates. The IHME study estimates 1.24 million annual deaths from malaria (range: 0.93 million - 1.69 million) while WHO's point estimate is 655 000 for 2010 (range: 537 000 to 907 000). In most settings and ages, the two studies' uncertainty intervals overlap and there are many similarities between the trends. The total number of malaria deaths is seen as falling consistently - in both studies - after prevention and control interventions were scaled up after 2004.
According to both methods, about 90% of malaria deaths occur in Africa. The most important difference between the estimates is regarding deaths in those over five years of age in Africa. According to IHME, malaria killed an estimated 435 000 people in this age group in 2010; while according to WHO it killed 55 000.
In this context, it is worth recalling the significant body of scientific evidence and consensus about the development of partial immunity to malaria in stably endemic areas, which has demonstrated that children over five years of age and adults are substantially protected against severe disease and death. Moreover, carefully conducted prospective hospital-based studies in a variety of settings suggest that the proportion of older adults dying from malaria is lower than would be expected from the IHME estimates." WHO, "Q&A on malaria mortality estimation," February 2012
- For further discussion of historical differences in methodology between WHO and IHME, see this blog post: Victoria Fan and Felix Lam, "Malaria Estimate Sausages by WHO and IHME," February 2012
- "4. How do the IHME findings published in February 2012 compare to the findings of WHO's World Malaria Report 2011?
- Note that the figures we cite from the World Malaria Report 2016, Gething et al. 2016, and the Global Burden of Disease 2017 may not be exactly comparable:
- The World Malaria Report 2016 and Gething et al. 2016 estimate the number of malaria deaths from 2015, while GBD 2017 estimates the number of malaria deaths from 2016.
- The World Malaria Report 2016 reports total deaths in the "WHO African region," which may include different countries than the "Sub-Saharan Africa" category reported in the GBD and Gething et al. 2016. It appears that the countries included in each regional definition are similar enough for our purposes. See definitions for these regions at the following links: WHO, "WHO regional offices" and Wikipedia, "Sub-Saharan Africa".
- Overall estimates of malaria mortality in sub-Saharan Africa (or WHO African region) in 2015 or 2016 by organization:
- 3
- Overall estimates of malaria mortality in sub-Saharan Africa (or WHO African region) in 2015 or 2016 by organization:
- WHO:
- Total malaria deaths (2015, WHO African region): about 394,000
- Malaria deaths among children under 5 (2015, WHO African region): about 292,000
- Malaria deaths among people 5 and over (2015, WHO African region): about 102,000
- Source: Table 6.4, Pg. 43, World Malaria Report 2016 provides estimates of the number of malaria deaths, including in children under 5 years old, by region of the world for 2015. Estimated total deaths in WHO African Region: 394,000 (95% CI: 230,000 to 549,000). Estimated deaths <5 years in African region: 292,000 (95% CI: 171,000 to 408,000). So, the estimated % of deaths in children <5 years old in the African region is about 74% (292,000 / 394,000 = about 74.11%). See Pg. 43, WHO, World Malaria Report 2016.
- GBD:
- Total malaria deaths (2016, sub-Saharan Africa): about 641,000
- Malaria deaths among children under 5 (2016, sub-Saharan Africa): about 492,000
- Malaria deaths among people 5 and over (2016, sub-Saharan Africa): about 149,000
- Source: See GBD-Compare tool figures: http://ihmeuw.org/478u and http://ihmeuw.org/478v. This implies that about 77% of malaria deaths were in children under 5 years old (492,000 / 641,000 = about 76.76%).
- MAP:
- Total malaria deaths (2015, sub-Saharan Africa): about 631,000
- Malaria deaths among children under 5 (2015, sub-Saharan Africa): about 464,000
- Malaria deaths among people 5 and over (2015, sub-Saharan Africa): about 167,000
- Source:
- "Across sub-Saharan Africa during the past 15 years, we estimated that there was an overall decrease of 57% (95% uncertainty interval, 46 to 65) in the rate of malaria deaths, from 12.5 (95% uncertainty interval, 8.3 to 17.0) per 10,000 population in 2000 to 5.4 (95% uncertainty interval, 3.4 to 7.9) in 2015. This led to an overall decrease of 37% (95% uncertainty interval, 36 to 39) in the number of malaria deaths annually, from 1,007,000 (95% uncertainty interval, 666,000 to 1,376,000) to 631,000 (95% uncertainty interval, 394,000 to 914,000). The share of malaria deaths among children younger than 5 years of age ranged from more than 80% at a rate of death of more than 25 per 10,000 to less than 40% at rates below 1 per 10,000. Areas with high malaria mortality (>10 per 10,000) and low coverage (<50%) of insecticide-treated bed nets and antimalarial drugs included much of Nigeria, Angola, and Cameroon and parts of the Central African Republic, Congo, Guinea, and Equatorial Guinea." Pg. 2435, Gething et al. 2016
- "As transmission declined between 2000 and 2015, the share of annual malaria deaths in children 4 years of age or younger and in those 5 to 14 years of age decreased (from 78.7% to 73.5% and from 6.7% to 4.8%, respectively), and the share in persons 15 years of age or older increased (from 14.6% to 21.7%). An expanded set of mapped estimates according to age group and year is provided in Figs. S2 and S3 in the Supplementary Appendix." Pg. 2442, Gething et al. 2016
- WHO:
- Historically (e.g. in 2011), the GBD study (published by IHME) estimated about 8x more malaria mortality among those over age five in Africa than the WHO did (see below). As of the 2015-2016 estimates, it appears that GBD estimated about 149,000 malaria deaths among people 5 and over as compared to the roughly 102,000 deaths estimated by WHO (see above).
- "4. How do the IHME findings published in February 2012 compare to the findings of WHO's World Malaria Report 2011?
The IHME study entitled "Global malaria mortality between 1980 and 2010: a systematic analysis" published in the Lancet on 3 February 2012 raised many questions about the differences between malaria burden estimates. The IHME study estimates 1.24 million annual deaths from malaria (range: 0.93 million - 1.69 million) while WHO's point estimate is 655 000 for 2010 (range: 537 000 to 907 000). In most settings and ages, the two studies' uncertainty intervals overlap and there are many similarities between the trends. The total number of malaria deaths is seen as falling consistently - in both studies - after prevention and control interventions were scaled up after 2004.
According to both methods, about 90% of malaria deaths occur in Africa. The most important difference between the estimates is regarding deaths in those over five years of age in Africa. According to IHME, malaria killed an estimated 435 000 people in this age group in 2010; while according to WHO it killed 55 000.
In this context, it is worth recalling the significant body of scientific evidence and consensus about the development of partial immunity to malaria in stably endemic areas, which has demonstrated that children over five years of age and adults are substantially protected against severe disease and death. Moreover, carefully conducted prospective hospital-based studies in a variety of settings suggest that the proportion of older adults dying from malaria is lower than would be expected from the IHME estimates." WHO, "Q&A on malaria mortality estimation," February 2012
- For further discussion of historical differences in methodology between WHO and IHME, see this blog post: Victoria Fan and Felix Lam, "Malaria Estimate Sausages by WHO and IHME," February 2012
- "4. How do the IHME findings published in February 2012 compare to the findings of WHO's World Malaria Report 2011?
- Note that the figures we cite from the World Malaria Report 2016, Gething et al. 2016, and the Global Burden of Disease 2017 may not be exactly comparable:
- The World Malaria Report 2016 and Gething et al. 2016 estimate the number of malaria deaths from 2015, while GBD 2017 estimates the number of malaria deaths from 2016.
- The World Malaria Report 2016 reports total deaths in the "WHO African region," which may include different countries than the "Sub-Saharan Africa" category reported in the GBD and Gething et al. 2016.
- Though, MAP notes that it estimates that the age profile of malaria mortality can differ substantially by region within sub-Saharan Africa.
- "Across sub-Saharan Africa during the past 15 years, we estimated that there was an overall decrease of 57% (95% uncertainty interval, 46 to 65) in the rate of malaria deaths, from 12.5 (95% uncertainty interval, 8.3 to 17.0) per 10,000 population in 2000 to 5.4 (95% uncertainty interval, 3.4 to 7.9) in 2015. This led to an overall decrease of 37% (95% uncertainty interval, 36 to 39) in the number of malaria deaths annually, from 1,007,000 (95% uncertainty interval, 666,000 to 1,376,000) to 631,000 (95% uncertainty interval, 394,000 to 914,000). The share of malaria deaths among children younger than 5 years of age ranged from more than 80% at a rate of death of more than 25 per 10,000 to less than 40% at rates below 1 per 10,000. Areas with high malaria mortality (>10 per 10,000) and low coverage (<50%) of insecticide-treated bed nets and antimalarial drugs included much of Nigeria, Angola, and Cameroon and parts of the Central African Republic, Congo, Guinea, and Equatorial Guinea." Pg. 2435, Gething et al. 2016
- "A comparison among age groups highlights the markedly higher vulnerability to death from malaria among children younger than 5 years of age, and this risk is reflected in both the highest rates and highest numbers of deaths across the continent in this age group. However, the share of estimated malaria deaths between children younger than 5 years of age and those 5 years of age or older varies considerably according to geographic region (Fig. 4A). This variation highlights the use of these estimates for informing malaria control and treatment strategies that are tailored to the demographic structure of local malaria burdens. Such efforts will become increasingly important as the malaria burden is further reduced and shifts from children toward adults (Fig. 4B)." Pgs. 2441-2442, Gething et al. 2016
- Overall estimates of malaria mortality in sub-Saharan Africa (or WHO African region) in 2015 or 2016 by organization:
- 4
Historically (e.g. in 2011), the GBD study (published by IHME) estimated about 8x more malaria mortality among those over age five in Africa than the WHO did (see below). As of the 2015-2016 estimates, it appears that GBD estimated about 149,000 malaria deaths among people 5 and over as compared to the roughly 102,000 deaths estimated by WHO (see above).
- "4. How do the IHME findings published in February 2012 compare to the findings of WHO's World Malaria Report 2011?
The IHME study entitled "Global malaria mortality between 1980 and 2010: a systematic analysis" published in the Lancet on 3 February 2012 raised many questions about the differences between malaria burden estimates. The IHME study estimates 1.24 million annual deaths from malaria (range: 0.93 million - 1.69 million) while WHO's point estimate is 655 000 for 2010 (range: 537 000 to 907 000). In most settings and ages, the two studies' uncertainty intervals overlap and there are many similarities between the trends. The total number of malaria deaths is seen as falling consistently - in both studies - after prevention and control interventions were scaled up after 2004.
According to both methods, about 90% of malaria deaths occur in Africa. The most important difference between the estimates is regarding deaths in those over five years of age in Africa. According to IHME, malaria killed an estimated 435 000 people in this age group in 2010; while according to WHO it killed 55 000.
In this context, it is worth recalling the significant body of scientific evidence and consensus about the development of partial immunity to malaria in stably endemic areas, which has demonstrated that children over five years of age and adults are substantially protected against severe disease and death. Moreover, carefully conducted prospective hospital-based studies in a variety of settings suggest that the proportion of older adults dying from malaria is lower than would be expected from the IHME estimates." WHO, "Q&A on malaria mortality estimation," February 2012
- For further discussion of historical differences in methodology between WHO and IHME, see this blog post: Victoria Fan and Felix Lam, "Malaria Estimate Sausages by WHO and IHME," February 2012
- "4. How do the IHME findings published in February 2012 compare to the findings of WHO's World Malaria Report 2011?
- 5
- "Although there is not substantial empirical evidence, it is reasonable to expect that ITNs will avert some adult mortality. Nets will likely be less effective at averting adult deaths in high transmission areas, since adults in high transmission areas typically have high levels of malaria immunity....GiveWell proposed using the estimated impact of ITNs on malaria case rates in adults as a rough proxy for declines in adult malaria mortality. Dr. Kleinschmidt said that if one needs to estimate declines in adult malaria mortality, this approach does not seem unreasonable in many settings. Following an ITN distribution, immunity levels in adults would not be expected to change substantially in the short-term. If health service quality is unchanged following a distribution, it is probably reasonable to expect that observed reductions in adult mortality may, at least in part, be attributable to the impact of ITNs on case rates." GiveWell's non-verbatim summary of a conversation with Immo Kleinschmidt on May 25, 2017
- "GiveWell: The theoretical mechanism by which ITNs could reduce adult malaria mortality seems quite simple, and very similar to that for children: they sleep under nets, so they get bitten less, so they get less malaria, so they are less likely to die from malaria. Does this sound right, or are there factors that limit the comparison with children, such as different sleeping patterns?
Dr. Churcher: That sounds roughly correct, though the link between getting malaria and dying from it will depend heavily on their level of immunity and therefore vary from place to place. We investigated mosquito biting times and the times people are under a bed net, and generally did not find large differences between adults and children, though it did vary substantially from site to site. Bed net usage rates among adults are quite good overall; they mostly share a sleeping place with young children. Again, there is very little research out there and quite a lot of variability. For example, one study found the lowest usage is often among teenagers as, unlike young children, adolescents often don’t share sleeping spaces with their parents." GiveWell's non-verbatim summary of a conversation with Thomas Churcher and Hilary Ranson on May 31, 2017
- 6
- "Malaria mortality in adults has not been closely studied via empirical research. This is likely because adult malaria mortality is difficult to measure in resource-poor settings. Adults in these settings may die of malaria without entering health systems. Post-mortems will not always be performed to determine causes of death." GiveWell's non-verbatim summary of a conversation with Immo Kleinschmidt on May 25, 2017
- "GiveWell: We have been unable to find much empirical research [on] the impact of ITNs on adult malaria mortality. Is there substantial research that we have not seen, and why do you think we have not been able to find more research?
Dr. Churcher: It is true that there are not many clear estimates on these issues. This is largely because the complex nature of immunity makes impacts on adult malaria mortality very hard to estimate. Young children will have fairly similar responses to an anti-malaria intervention because they have not yet developed immunity. Adults are much more variable: in high transmission areas almost all have considerable immunity, which reduces the chance that a case of malaria will result in death. Therefore though ITNs would prevent cases in adults it might limit the impact of ITNs on adult case fatality. In comparison, in low transmission settings the case fatality rate would be higher due to lower immunity, so ITNs may be more effective at reducing the number of deaths. Due to the cost and difficulty of conducting trials, it would be very challenging to obtain good quality data." GiveWell's non-verbatim summary of a conversation with Thomas Churcher and Hilary Ranson on May 31, 2017
- 7
- "A randomized, double-blind, field trial was carried out to compare the effectiveness of permethrin-treated bed nets with that of untreated nets as a method of malaria control for migrant workers in eastern Thailand. The study was conducted using 261 subjects in eastern rural areas that are known to be highly endemic for multidrug-resistant Plasmodium falciparum infection. One hundred twenty-six subjects used treated nets, while 135 used untreated nets. During the 35 weeks of observation, 23 subjects using treated nets and 33 workers using untreated nets developed 28 and 51 episodes of malaria, respectively (P = 0.029). The reduction in risk per subject due to treated nets was 0.06. The residual effects of permethrin were tested using a World Health Organization standard bioassay. Anti-mosquito activity was found to be present in the nets for more than 16 months. We conclude that because of the failure of the development of safe, effective, long-lasting prophylactic agents, integrating the use of impregnated nets with large-scale primary health care programs may be a partially effective method for controlling malaria in eastern Thailand." Abstract, Kamol-Ratanakul and Prasittisuk 1992
- There were about 135 migrant workers in the control group (received untreated nets) and about 126 migrant workers in the treatment group (received insecticide-treated nets). Among these workers, about 33 in the control group acquired malaria while about 23 in the treatment group acquired malaria. The total number of malaria episodes in the control group were 51, compared with the treatment group's 28. The number of malaria episodes per 1,000 person-weeks in the control group were 10.79, compared with the treatment group's 6.35. See Table 2, Pg. 307, Kamol-Ratanakul and Prasittisuk 1992.
- We are uncertain which outcome estimate is most appropriate to use as a headline estimate. The risk reduction based on malaria episodes per 1,000 person-weeks was about 41% (1-(6.35/10.79) = .411). The risk reduction based on number of people who acquired malaria was about 30% (1-(23/33) = .303).
- The mean age of the migrant workers in this study was about 21-23 years old. See Table 1, Pg. 306, Kamol-Ratanakul and Prasittisuk 1992.
- 8
- "Malaria mortality in adults has not been closely studied via empirical research. This is likely because adult malaria mortality is difficult to measure in resource-poor settings. Adults in these settings may die of malaria without entering health systems. Post-mortems will not always be performed to determine causes of death.
...Dr. Kleinschmidt believes that there has not been academic interest in modeling the impact of ITNs on adult malaria mortality because it is fraught with difficulties. He believes it is possible to make a crude estimate, but he thinks it would be very difficult to precisely measure ITNs' impact on adult mortality." GiveWell's non-verbatim summary of a conversation with Immo Kleinschmidt on May 25, 2017 - "GiveWell: We have been unable to find much empirical research the impact of ITNs on adult malaria mortality. Is there substantial research that we have not seen, and why do you think we have not been able to find more research?
Dr. Churcher: It is true that there are not many clear estimates on these issues. This is largely because the complex nature of immunity makes impacts on adult malaria mortality very hard to estimate. Young children will have fairly similar responses to an anti-malaria intervention because they have not yet developed immunity. Adults are much more variable: in high transmission areas almost all have considerable immunity, which reduces the chance that a case of malaria will result in death. Therefore though ITNs would prevent cases in adults it might limit the impact of ITNs on adult case fatality. In comparison, in low transmission settings the case fatality rate would be higher due to lower immunity, so ITNs may be more effective at reducing the number of deaths. Due to the cost and difficulty of conducting trials, it would be very challenging to obtain good quality data." GiveWell's non-verbatim summary of a conversation with Thomas Churcher and Hilary Ranson on May 31, 2017
- "Malaria mortality in adults has not been closely studied via empirical research. This is likely because adult malaria mortality is difficult to measure in resource-poor settings. Adults in these settings may die of malaria without entering health systems. Post-mortems will not always be performed to determine causes of death.
- 9
"GiveWell: The theoretical mechanism by which ITNs could reduce adult malaria mortality seems quite simple, and very similar to that for children: they sleep under nets, so they get bitten less, so they get less malaria, so they are less likely to die from malaria. Does this sound right, or are there factors that limit the comparison with children, such as different sleeping patterns?
Dr. Churcher: That sounds roughly correct, though the link between getting malaria and dying from it will depend heavily on their level of immunity and therefore vary from place to place. We investigated mosquito biting times and the times people are under a bed net, and generally did not find large differences between adults and children, though it did vary substantially from site to site. Bed net usage rates among adults are quite good overall; they mostly share a sleeping place with young children. Again, there is very little research out there and quite a lot of variability. For example, one study found the lowest usage is often among teenagers as, unlike young children, adolescents often don’t share sleeping spaces with their parents." GiveWell's non-verbatim summary of a conversation with Thomas Churcher and Hilary Ranson on May 31, 2017
- 10“[I]n high transmission areas almost all [adults] have considerable immunity, which reduces the chance that a case of malaria will result in death. Therefore though ITNs would prevent cases in adults it might limit the impact of ITNs on adult case fatality. In comparison, in low transmission settings the case fatality rate would be higher due to lower immunity, so ITNs may be more effective at reducing the number of deaths." GiveWell's non-verbatim summary of a conversation with Thomas Churcher and Hilary Ranson on May 31, 2017
- 11
"GiveWell: The theoretical mechanism by which ITNs could reduce adult malaria mortality seems quite simple, and very similar to that for children: they sleep under nets, so they get bitten less, so they get less malaria, so they are less likely to die from malaria. Does this sound right, or are there factors that limit the comparison with children, such as different sleeping patterns?
Dr. Churcher: That sounds roughly correct, though the link between getting malaria and dying from it will depend heavily on their level of immunity and therefore vary from place to place. We investigated mosquito biting times and the times people are under a bed net, and generally did not find large differences between adults and children, though it did vary substantially from site to site. Bed net usage rates among adults are quite good overall; they mostly share a sleeping place with young children. Again, there is very little research out there and quite a lot of variability. For example, one study found the lowest usage is often among teenagers as, unlike young children, adolescents often don’t share sleeping spaces with their parents." GiveWell's non-verbatim summary of a conversation with Thomas Churcher and Hilary Ranson on May 31, 2017
- 12
In our cost-effectiveness analysis of the Against Malaria Foundation (AMF) (see most recent CEA on this page), we estimate the number of adult deaths averted with the following process:
- We estimate the malaria burden in countries where AMF works using mortality estimates from the Global Burden of Disease Project.
- Using those estimates, we calculate the expected number of 5 and over malaria deaths for every under-5 malaria death.
- We multiply the number from the step above by (a) the number of under-5 deaths averted according to our model (which is based on the results of a meta-analysis of net distributions and adjusted for a variety of factors) and (b) an adjustment factor accounting for the previously discussed reasons why bed nets may not be as effective at reducing the relative risk of malaria mortality for individuals 5 and over as they are at reducing the relative risk of under-5 malaria mortality.
In this calculation, the key factor is the ratio of 5-and-over malaria deaths relative to under-5 malaria deaths (rather than the raw number of adult malaria deaths).
For further details on how we incorporate 5-and-over malaria mortality into our CEA, see the "Nets" sheet in the most recent CEA on this page and search for "Deaths averted — individuals 5+ years old."