We have published a more recent review of this organization. See our most recent report on the Sightsavers' deworming program.
Sightsavers' deworming program is one of our top-rated charities and we believe that it offers donors an outstanding opportunity to accomplish good with their donations.
More information: What is our evaluation process?
Published: November 2017
Summary
What do they do? Sightsavers (https://www.sightsavers.org/) is a large organization with multiple program areas that focuses on preventing avoidable blindness and supporting people with impaired vision. We have only reviewed Sightsavers' work to prevent and treat neglected tropical diseases (NTDs), and, more specifically, advocating for, funding, and monitoring programs that treat schistosomiasis and soil-transmitted helminthiasis (STH) ("deworming"); our recommendation is just for Sightsavers' work on deworming. (More)
Does it work? We believe that there is strong evidence that administration of deworming drugs reduces worm loads but weaker evidence on the causal relationship between reducing worm loads and improved life outcomes; we consider deworming a priority program given the possibility of strong benefits at low cost. Sightsavers has shared surveys for some of its past NTD programs that measure whether these programs have reached a large proportion of children targeted. These studies have generally found moderately positive results, but have some methodological limitations. We have seen very limited results from Sightsavers' deworming programs specifically. For GiveWell-supported programs, Sightsavers has told us it will conduct coverage surveys for each mass drug administration (MDA); we have reviewed one of those surveys to date. (More)
What do you get for your dollar? Our best guess is that deworming is generally highly cost-effective. We estimate that children are dewormed for a total of around $1.19 per child in Sightsavers-supported programs. This figure relies on several difficult-to-estimate inputs including how to account for (a) donated drugs and (b) in-kind contributions from governments with which Sightsavers works. Excluding drugs and government contributions, we estimate that Sightsavers' cost per treatment is $0.55. The number of lives significantly improved is a function of a number of difficult-to-estimate factors, which we discuss in detail in a separate report. (More)
Is there room for more funding? We believe that Sightsavers' deworming work is likely to be constrained by funding next year. Sightsavers has provided details of deworming programs that it could fund with additional funding of up to about $6.4 million in 2018 and 2019. Sightsavers appears to have limited prospects for funding these programs from other sources. We believe it is likely that Sightsavers could absorb funding beyond this amount to extend programs to 2020 and/or seek out additional opportunities to fund deworming programs. (More) December 2017 update: In November 2017, we recommended that Good Ventures give $2.5 million to Sightsavers' deworming program, reducing its room for more funding for 2018 and 2019 to about $3.9 million.
Sightsavers' deworming program is recommended because of:
- The strong track record and excellent cost-effectiveness of deworming. (More)
- Sightsavers' moderately strong process for assessing whether the MDA programs it supports are successfully reaching their intended recipients. (More)
- Standout transparency – it has shared significant, detailed information about its programs with us.
- Room for more funding – it can use additional funds to scale up its work on deworming.
Major open questions include:
- Sightsavers has a limited track record of implementing deworming programs. Deworming has not been a focus or major priority for Sightsavers, which may impact how well programs are carried out.
- The monitoring we have seen from Sightsavers is primarily from programs that do not treat for schistosomiasis or STH but which are implemented in similar fashion to deworming programs. This monitoring has some methodological limitations. While we expect monitoring from all programs that have been funded with donations due to GiveWell's recommendation ("GiveWell-directed" funding), we currently believe that Sightsavers has a fairly limited track record of producing the type of monitoring we find most useful for understanding program performance.
- Sightsavers is a large organization with significant unrestricted funding and fundraising capacity. (Sightsavers spends considerably more on fundraising than other charities we recommend—about 28% of overall funding and 48% of unrestricted funding, excluding gifts in kind.) It is possible that GiveWell-directed funds will cause Sightsavers to allocate less of its unrestricted funding or fundraising capacity to deworming than it otherwise would have. Sightsavers does not appear to have allocated large amounts of unrestricted funding to deworming in the past and told us that it has limited sources of restricted funding for deworming.
Table of Contents
- Summary
- Our review process
- A note about this review
-
What do they do?
- How does deworming fit in with Sightsavers' other activities?
- What types of deworming programs does Sightsavers support?
- How does Sightsavers select deworming programs to support?
- What role does Sightsavers play in supporting deworming programs?
- Descriptions of programs by country
- What is Sightsavers' staff structure?
- How has Sightsavers spent funds in the past?
-
Does it work?
- What is the independent evidence for the program?
- What is the likely impact per treatment in Sightsavers' programs compared with the independent studies on the impact of deworming?
- Are deworming pills delivered to and ingested by recipients?
- Are deworming programs operating as intended?
- What is the effect of Sightsavers' work on program outcomes?
- Are there any negative or offsetting impacts?
- What do you get for your dollar?
- Is there room for more funding?
- Sightsavers as an organization
- Sources
Our review process
We began considering Sightsavers as a potential top charity for its work on deworming in 2015. To date, we have:
- Had multiple conversations with Sightsavers staff.1
- Reviewed documents Sightsavers shared with us.
- Visited Sightsavers' country office in Ghana during one of our 2016 site visits. Sightsavers does not support a deworming program in Ghana, but we were able to have several conversations with Elizabeth Elhassan, Technical Director of NTDs, and Sunday Isiyaku, Country Director in Nigeria and Ghana, as well as other staff.
- Visited Sightsavers' country office in Guinea during one of our 2017 site visits. Sightsavers had recently supported a round of deworming in Guinea which was supported with GiveWell-directed funds. We met with several staff involved in the deworming program.
A note about this review
Sightsavers became a top charity in 2016. In 2017, as expected, we learned relatively little about the performance of Sightsavers deworming programs, because programs funded with GiveWell-directed funds were in their early stages. For most of our other top charities, we have spent several years reviewing and engaging with the charity's work. We feel that we know somewhat less about Sightsavers than two of our other three top charities that support deworming, the Schistosomiasis Control Initiative and Deworm the World Initiative and slightly less than the third, the END Fund.
What do they do?
Sightsavers focuses on preventing avoidable blindness and improving the lives of those who have visual impairments.2 Sightsavers' work on NTDs accounts for roughly half of its overall program expenditure budget.3 In this review, we evaluate the deworming programs in Sightsavers' neglected tropical diseases (NTDs) portfolio, focusing in particular on the types of programs on which Sightsavers has spent and committed the funding it received due to GiveWell's top charity recommendation starting in November 2016. We refer to that funding as "GiveWell-directed funds."
Sightsavers is primarily focused on adding deworming components to the community-based NTD programs that it already supports in Africa.4 Consistent with this focus, in 2017 Sightsavers used GiveWell-directed funds to add deworming MDAs to integrated NTD programs in the Democratic Republic of the Congo (DRC), Guinea, Guinea-Bissau, and in four Nigerian states; to support research related to deworming in Cameroon; and to initiate an integrated NTD program in Benue state, Nigeria.5 Our review focuses on these projects and to a lesser degree on Sightsavers' previous work on deworming.
The deworming programs that Sightsavers supports conduct MDAs which aim to treat the entire population of children within districts or implementation units that meet the World Health Organization (WHO)-defined minimum prevalence thresholds for MDA with deworming pills.6 In some high prevalence settings, Sightsavers supports adult treatments; Sightsavers notes that this is in line with WHO recommendations and is at the request of governments.7 Sightsavers provides both technical assistance and funding to governments and other implementing partners in the deworming programs it supports (more).
Below, we discuss:
- How deworming fits in with Sightsavers' other activities
- The types of deworming programs Sightsavers supports
- How Sightsavers selects programs to support
- Sightsavers' role in supporting deworming programs
- The status of Sightsavers' deworming work by country
- A breakdown of Sightsavers' recent spending
How does deworming fit in with Sightsavers' other activities?
Background
Sightsavers was founded in 1950 to treat eye conditions in developing countries.8 It continues to focus on eliminating avoidable blindness and supporting people with visual impairments and disabilities in low- and middle-income countries;9 this focus led to its work on integrated NTD programs, particularly programs targeting those NTDs that cause blindness (onchocerciasis and trachoma).10
Sightsavers began its work on deworming programs in 2011 as part of its integrated NTD programs.11 It currently supports deworming programs in six countries in Africa.12
Sightsavers' integrated NTD programs
Sightsavers began to work on NTD programs in the 1950s.13 It is our understanding that Sightsavers' integrated NTD program is focused on diseases that can be treated via MDAs, primarily onchocerciasis (which can cause blindness), trachoma (which can also cause blindness), lymphatic filariasis, schistosomiasis, and STH.14
Sightsavers has told us that most NTD-focused organizations (including Sightsavers) are prioritizing treating onchocerciasis, trachoma, and lymphatic filariasis, because these diseases have been targeted for elimination in the next decade.15 Schistosomiasis and STH (both of which are treated by deworming programs) are not as highly prioritized because elimination of these diseases is not expected soon.16 Sightsavers has used GiveWell-directed funds to add deworming components to the NTD programs that it already supports and to initiate a new integrated NTD program in Benue state, Nigeria; it is not interested in starting new programs that only support deworming.17
What types of deworming programs does Sightsavers support?
There are several different ways to implement mass drug administrations (MDAs). In a community-based MDA, a trained volunteer community drug distributor (CDD) travels from household to household distributing treatments over a period of several days or weeks, or distributes treatments from a fixed location in the community.18 In school-based MDAs, teachers are trained to provide treatments to children during normal school hours.19
In many deworming MDAs that Sightsavers supports, it supports a combination of school-based and community-based MDAs. Sightsavers told us that programs are planned to avoid children being treated in both their schools and communities. In some cases, school- and community-based MDAs do not overlap geographically. In locations where school enrollment is low, both methods may be used in the same area and children may be marked in some way (such as on a fingernail) or asked during community-based treatment if they already received treatment.20
Note that two of the other three top charities GiveWell recommends that support deworming programs (the Schistosomiasis Control Initiative and Deworm the World Initiative) primarily support school-based MDA programs. More about Sightsavers' views on the advantages and disadvantages of various types of MDAs can be found in our 2016 site visit notes.
How does Sightsavers select deworming programs to support?
Before supporting a new deworming program, Sightsavers told us that it considers:21
- The prevalence and intensity of schistosomiasis and STH in the area in which the program would occur.22
- The availability of funding for the deworming component. Sightsavers prefers to use restricted funding for deworming components because its unrestricted funding is in high demand by its other programs.
- The feasibility of the program given Sightsavers' partners' capacity and resources.
- The feasibility of the program given Sightsavers' capacity.
We have not yet asked Sightsavers for concrete examples of how it has applied the above criteria to determine whether or not to support a new deworming program.
What role does Sightsavers play in supporting deworming programs?
The deworming programs that Sightsavers supports are implemented by the governments or partners it works with.23 Sightsavers primarily provides technical assistance to governments and implementing partners and in some cases it also provides financial support. More details on Sightsavers' role in specific programs below.
What technical assistance does Sightsavers provide?
The assistance Sightsavers provides in each country varies depending on what its implementing partner needs. Sightsavers' role on deworming projects has included the following:
- Advocacy. Sightsavers meets with government representatives to encourage them to implement additional NTD programs.24
- Developing national plans. Sightsavers assists country governments and partner non-governmental organizations (NGOs) in developing national integrated plans for addressing NTDs.25
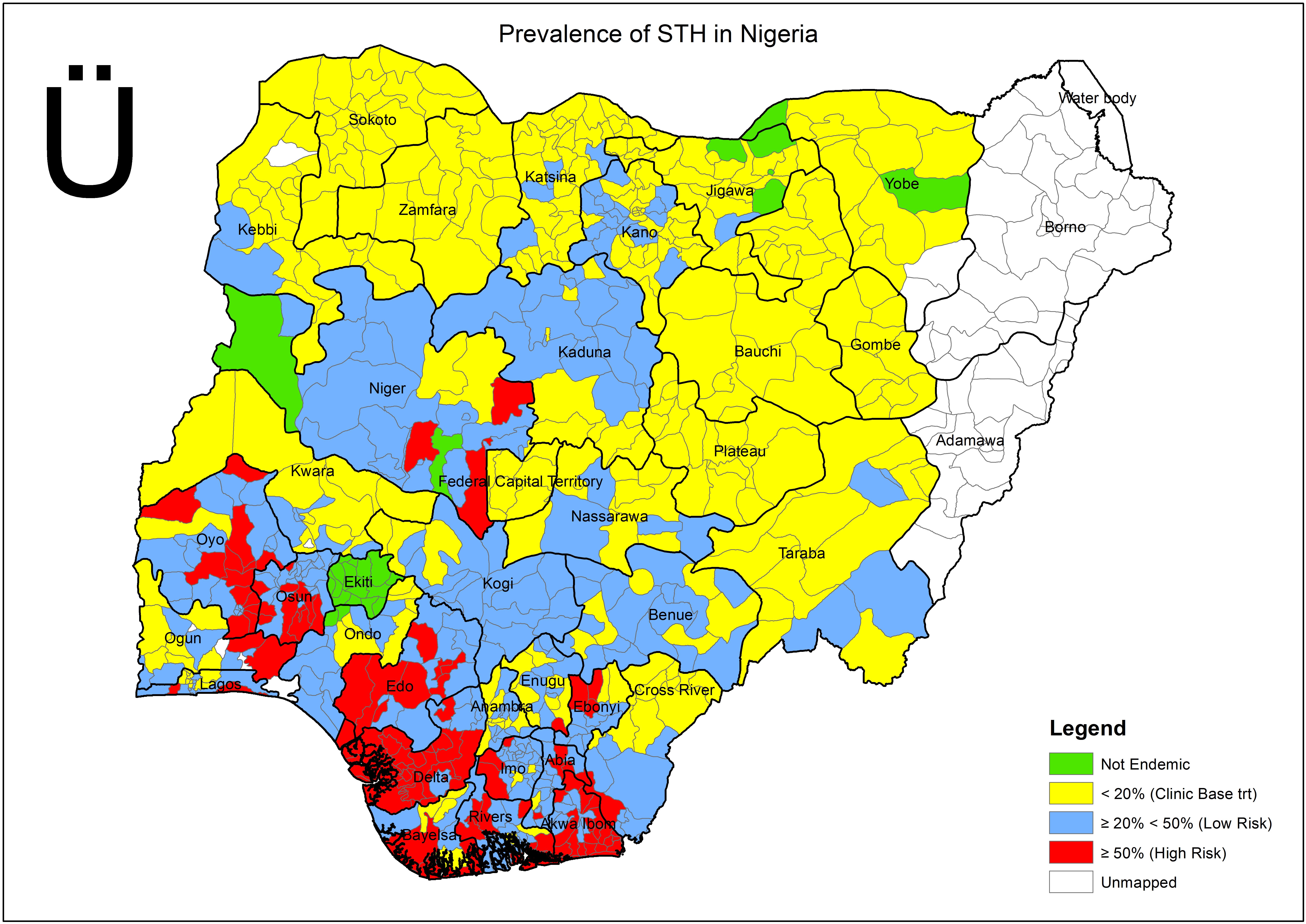
- Prevalence surveys. Sightsavers has led several projects designed to assess the prevalence of NTDs in a specified area. For example, Sightsavers led the Global Trachoma Mapping Project and mapped the prevalence of STH and schistosomiasis in several states in Nigeria.26
- Trainings. Sightsavers helps plan and develop trainings for those who will implement the MDA and supports trainings on how to use health management information systems and national NTD databases.27
- Drug logistics. Sightsavers provides support in some locations for drug logistics, such as storage.28
- Community sensitization. Sightsavers helps with efforts to create awareness within communities about when an MDA will occur and why it is important.29
- Monitoring and reports. We have focused on Sightsavers' coverage surveys, but Sightsavers has also told us about additional monitoring activities it has conducted (see footnote).30
Sightsavers told us that it aims to periodically conduct coverage surveys on all of its MDA programs,31
and that it plans to conduct coverage surveys for deworming MDA projects supported by GiveWell-directed funds annually.32
A coverage survey involves sending representatives to treatment areas to survey community members about whether they received and ingested a treatment. We discuss the methodology and results from some coverage surveys we have seen below.
Sightsavers has described other types of monitoring that it conducts; we are not sure if Sightsavers regularly supports additional monitoring for its deworming programs.33 For example, it told us that it conducted impact assessments in Nigeria in 201634 (which we understand to mean measurements of worm prevalence and/or intensity before a program and after one or more rounds of MDA35 ); we have requested the results from this study but have not yet received them.36
What financial assistance does Sightsavers provide?
Sightsavers supports MDA programs financially when necessary.37 Historically, it has paid for expenses like planning meetings, monitoring and evaluation, vehicles, computers, education materials, sensitization activities, and supervision activities.38 Sightsavers supports its partners' salary costs on some projects, where appropriate for operational reasons and where this has been built into the project and approved by the donor.39 When providing financial support, Sightsavers told us that it asks implementing partners to provide detailed, activity-based budgets;40 we have not yet seen budgets at this level of detail (more).
Descriptions of programs by country
In this section we describe the projects on which Sightsavers has spent or committed GiveWell-directed funds. Information about other Sightsavers projects with deworming components is available here.
Nigeria
Nigeria is one of Sightsavers' largest country programs and the first where it implemented deworming; Sightsavers has worked there on various programs for over 40 years and on deworming programs since 2011.41
Sightsavers has used GiveWell-directed funds to support two projects in Nigeria; it has so far committed funds for 2017-2018:42
- In Kebbi, Kogi, Kwara and Sokoto states, Sightsavers treats children aged 5 to 15 years through a combination of yearly school- and community-based MDAs, using community-based MDAs to target out-of-school children.43 GiveWell-directed funds support schistosomiasis treatments in 34 local government areas (LGAs) and combined schistosomiasis and STH treatments in 17 LGAs, including one LGA where Sightsavers will also target adults consistent with WHO protocols.44 A grant from the Schistosomiasis Control Initiative (another GiveWell top charity) funded deworming work in an additional 28 LGAs across these 4 states in 2017.45
- In Benue state, Sightsavers conducts annual school-based MDAs for schistosomiasis and STH; in some areas, GiveWell-directed funds also support community-based MDAs for lymphatic filariasis and onchocerciasis.46
In addition to GiveWell-directed funds, these projects are funded by the UK government's UK Aid Match and Sightsavers' unrestricted funds (details in footnote).47 Our understanding is that lymphatic filariasis and onchocerciasis work in Kebbi, Kogi, Kwara and Sokoto states was fully funded before GiveWell recommended Sightsavers and therefore GiveWell-directed funds support the deworming components of Sightsavers programs in these states.48 In Benue state, Sightsavers did not have funding for other NTD work and GiveWell-directed funds therefore support all of the NTD treatments.49
In each of the programs that GiveWell-directed funds support, Sightsavers partners with the Nigerian government, which implements the programs, while Sightsavers provides technical assistance, monitoring, financial management support, and donations of items such as vehicles.50 In addition, Sightsavers helps to coordinate the government's national and state NTD teams and assists these teams in developing their strategies.51 In Benue state, Sightsavers is also collaborating with UNICEF on water, sanitation and hygiene (WASH) activities.52
We note that Sightsavers also has funding from the UK government to support an integrated NTD program that includes treatments for STH and schistosomiasis in five other states in Northern Nigeria, in partnership with CBM, Helen Keller International, and MITOSATH.53
Guinea-Bissau
Sightsavers' past NTD work in Guinea-Bissau has focused on eliminating trachoma, onchocerciasis, and lymphatic filariasis.54 It has used GiveWell-directed funds to add deworming to its Guinea-Bissau NTD programming, to date committing funding for 2017-2018.55 Its other NTD work is ongoing, funded by UK Aid Match (lymphatic filariasis and onchocerciasis) and its unrestricted funds (trachoma).56
Following the completion of the schistosomiasis (SCH) and STH surveys in late 2017, Sightsavers told us that it will support SCH and STH MDAs in all districts in Guinea-Bissau reaching WHO-defined minimum prevalence thresholds for MDA.57 Sightsavers partners with the Ministries of Health and Education which will execute the MDAs, the first of which is planned for November/December 2017.58 Sightsavers provides technical support (for example, it trains the health workers who will supervise the MDA campaign), financial support, and programme monitoring.59 It also assists the government with the MDA planning process and advocates to the government for increased government ownership of the project.60
In 2017, Sightsavers also plans to support a mapping survey of STH and schistosomiasis prevalence in all provinces except the Bijagos archipelago (where the London School of Hygiene and Tropical Medicine is supporting STH and schistosomiasis prevalence mapping).61 We note that Sightsavers expects the new data to update its treatment targets, which are based on a prevalence survey conducted in 2005 (the most recent prevalence survey in Guinea-Bissau) and are therefore out of date.62
Cameroon
Sightsavers has worked on NTD programs in Cameroon since 1996 and school-based deworming programs since 2011.63 Sightsavers' partners include the Ministry of Public Health, Helen Keller International, and other NGOs. USAID funds most of its deworming work.64
Sightsavers has committed GiveWell-directed funds to a three-year project in Cameroon to (1) conduct a survey to measure prevalence and intensity of STH and schistosomiasis in 15 of 16 health districts in the regions where Sightsavers supports deworming65 and (2) develop strategies to deploy in areas where prevalence has remained high after five rounds of MDA. Sightsavers expects that the strategy will focus on training adults (health workers, teachers, etc.) on how to encourage better hygiene behaviors among children.66 More details about the study are available at Sightsavers, GiveWell Project Document Cameroon.
Guinea
Sightsavers has worked on NTDs in Guinea since 1993, focusing on onchocerciasis, trachoma and lymphatic filariasis.67 Using GiveWell-directed funds, Sightsavers has committed funding to provide deworming treatments in three health districts for 2017-2018; deworming in other districts in Guinea is largely supported by Helen Keller International.68
Sightsavers' deworming work targets school-aged children between 5 and 15 years using school-based and community based MDAs.69 Sightsavers provides logistical support and technical, financial, and human resources to the program.70 It also works with the government and other implementing partners to incorporate deworming work into the national NTD plan.71
Democratic Republic of the Congo
Sightsavers has supported NTD programs in DRC since 2011.72 Sightsavers works in three provinces; its partner in those provinces is the United Front Against Riverblindness (UFAR).73 In 2015, Sightsavers partnered with the Schistosomiasis Control Initiative (SCI) to support the distribution of deworming treatments in the Lubutu territory in Maniema province. Sightsavers continued this support in 2016, but we understand that work has now ceased.74
Sightsavers has allocated GiveWell-directed funds to add deworming components to its NTD programming in Ituri Nord, Ituri Province, in the northeastern region of the DRC; it has committed funds for 2017 and 2018 so far.75 The program will target school-aged children between 5 and 15 years through yearly school-based and community-based MDAs;76 the first MDA is planned for October/November 2017.77
Sightsavers and UFAR support the DRC's Ministry of Health in implementing the program by procuring drugs, providing logistical support and communication materials, providing technical assistance, monitoring and supervising the program, and funding the distribution.78
What is Sightsavers' staff structure?
Sightsavers' work on NTDs is spread across three main departments: finance and planning, NTDs, and policy and program strategy, which includes research.79 These departments work closely with regional office teams in Sub-Saharan Africa on the strategic planning and implementation of NTD projects in each country.80
As of 2016, Sightsavers employed a West Africa regional director, an East and Central Africa regional director, and 11 country directors for 20 country offices in Africa.81 Some country directors supervise multiple countries.82 There are also some countries for which Sightsavers does not have any permanent on-the-ground staff and instead works fully through partners.83 Some country offices include monitoring and evaluation (M&E) staff, and recently Sightsavers has been adding NTD Managers to its country teams.84 Additionally, Sightsavers has technical advisors who travel country to country, disseminating information on best practices for MDAs and monitoring and providing regular remote assistance.85 In 2017, Sightsavers used GiveWell-directed funds to recruit new program officers, for example, in Guinea-Bissau.86
Within country offices, the standard staff are:87
- Country director. Country directors oversee the program managers. They also oversee the finance and support teams.
- Program managers. Program managers oversee the program officers and work with the finance and support teams.
- Program officers. Program officers do a large portion of Sightsavers' work in the field and spend much of their time on monitoring activities. They visit implementing partners to check that activities are proceeding according to schedule and visit communities to observe whether or not work is being carried out as expected. They also train partners' staff on program delivery.
- Finance and support team. Usually 1 to 4 people, this team provides the financial and operational support for Sightsavers' activities in the country. The finance team helps to design budgets for programs and regularly monitors partner expenditures to ensure that funds are being spent in accordance with budgets.88
How has Sightsavers spent funds in the past?
We have seen very high-level summaries of Sightsavers spending between 2014 and 2016.89 The vast majority of this spending was funded by in-kind gifts from other organizations, which are mostly drug donations.90 Excluding in-kind gifts, a rough characterization of Sightsavers' spending between 2014 and 2016 is that approximately 90% of funding was split roughly equally between fundraising, eye care programs, and NTD programs.91 This spreadsheet shows our breakdown of Sightsavers' 2014-2016 spending (in USD).92
Spending on NTD and deworming programs
From 2014-2016, Sightsavers spent around $50 million in unrestricted funding each year.93 In 2014, 2015, and 2016, Sightsavers spent, respectively, 7%, 9%, and 6% of its unrestricted funding on NTD programs.94 Most of the funding for NTD programs was from restricted funding sources; 18%, 14% and 8% of NTD programs were funded by unrestricted funds in 2014, 2015, and 2016, respectively.95
We do not know what portion of Sightsavers' spending supported deworming programs alone: although Sightsavers has shared its 2014, 2015, and 2016 spending and its 2017 projected spending by NTD program with us, deworming components are not separated out from the other programs.96 Sightsavers' 2017 projections and 2016 spending indicate that about 34% of total NTD funding is allocated to integrated programs for onchocerciasis, lymphatic filariasis, schistosomiasis, and STH, with the remainder spent on trachoma.97 Projects Sightsavers has allocated GiveWell-directed funds to comprise about 5% of projected 2017 spending on NTD programs.98
Sightsavers has shared budgets for its projected spending of GiveWell-directed funds received between when we added Sightsavers to our list of top charities in November 2016 to when it set its budget for the year around May 2017, totaling $3 million (see this spreadsheet). Below, we present a breakdown of projected spending by category and country.
Sightsavers projected spending using GiveWell-directed funds (2017-2019)99
| Spending category | % of projected spending |
|---|---|
| Capital expenditure | 2% |
| Project activities | 48% |
| Staff costs | 9% |
| Administration costs | 2% |
| Monitoring, evaluation and lesson learning | 19% |
| Program management | 13% |
| Overheads | 8% |
| Country | % of projected spending |
|---|---|
| Nigeria | 38% |
| Guinea-Bissau | 32% |
| Cameroon | 13% |
| Guinea | 12% |
| DRC | 5% |
Spending on fundraising
Sightsavers spent 27-29% of its total spending (excluding in-kind contributions), which was 45-51% of its unrestricted funding, on fundraising activities in 2014, 2015 and 2016.100 While we typically do not put too much weight on an organization's spending breakdown (for reasons explained in this blog post), this seems higher than we've seen from other top charities—though we recognize that there can be significant variation in how organizations categorize costs. When we asked Sightsavers about its high fundraising costs, it noted that it aims to use less than one third of its total annual budget on fundraising and that this is consistent with industry standards.101 Sightsavers also highlighted that when the value of in-kind gifts are included, Sightsavers’ fundraising costs are under 10%.102
Does it work?
We believe that there is strong evidence that administration of deworming drugs reduces worm loads but weaker evidence on the causal relationship between reducing worm loads and improved life outcomes, such as increased income and consumption. We consider deworming a priority program given the possibility of strong benefits at low cost.
To evaluate Sightsavers' track record at executing programs, we have primarily considered results from coverage surveys of past programs. The coverage surveys we have seen from Sightsavers are generally of moderate quality, and are primarily from programs that are delivered using fairly similar methods to deworming but which focused on NTDs other than schistosomiasis or STH. We have seen one coverage survey from an MDA funded by GiveWell-directed funds and expect to see more such surveys in future years.
In this section, we also discuss how the disease burden in the areas where Sightsavers works compares to that of the places where the independent studies that form the evidence base for the impact of deworming were conducted. While Sightsavers' programs generally target areas that require mass treatment according to WHO guidelines, the disease burden in areas where Sightsavers works is on average lower than in the studies mentioned below, so our expectation is that the average impact per child treated is lower in Sightsavers areas. We adjust our cost-effectiveness analysis accordingly.
What is the independent evidence for the program?
Sightsavers supports MDAs to treat communities for NTDs, including schistosomiasis and STH. While we do not have a strong view on the evidence behind and cost-effectiveness of integrated NTD programs, we have reviewed the independent evidence for deworming programs, which we discuss extensively in our intervention report on deworming. In short, we believe that there is strong evidence that administration of the drugs reduces worm loads but weaker evidence on the causal relationship between reducing worm loads and improved life outcomes; we consider deworming a priority program given the small possibility of strong benefits at a very low cost.
We do not know how similar the areas where Sightsavers works are to the places where the key studies on improved life outcomes from deworming took place. It is possible that Sightsavers works in locations where the type and severity of worm infections are significantly different (more in the next section).
What is the likely impact per treatment in Sightsavers' programs compared with the independent studies on the impact of deworming?
In general, mass deworming programs treat everyone in a targeted demographic, regardless of whether each individual is infected (more). Because of this, the benefits (and therefore the cost-effectiveness) of a program are highly dependent on the baseline prevalence of worm infections.
In this section, we discuss how the disease burden in the areas where Sightsavers works compares to the places where the independent studies that form the evidence base for the impact of deworming were conducted. While it is our understanding that Sightsavers programs generally target areas that require mass treatment according to WHO guidelines,103 the disease burden in areas where Sightsavers works is on average lower than in the study areas, so our expectation is that the impact per child treated is lower in the areas where Sightsavers works. We adjust our cost-effectiveness estimate (more below) accordingly.
In this spreadsheet, we compare the prevalence of the places in which Sightsavers currently supports a program to the prevalence from the studies providing the best evidence for the benefits of deworming. Note that we used a number of approximations to arrive at an estimate that could be used in our cost-effectiveness analysis.
Key pieces of evidence that we discuss in our report on deworming (Miguel and Kremer 2004, Baird et al. 2012, and Croke 2014) are from deworming experiments conducted in Kenya and Uganda in the late 1990s and early 2000s. Prior to receiving deworming treatment, the participants in those studies had relatively high rates of moderate-to-heavy infections of schistosomes or hookworm.104
Are deworming pills delivered to and ingested by recipients?
We believe there is moderately strong evidence that pills have been delivered to and ingested by a large proportion of targeted recipients in Sightsavers-supported programs in the past. The evidence we have seen is from Sightsavers-supported NTD MDA programs, two of which included deworming—including one coverage survey for an MDA supported by GiveWell-directed funds in Guinea. We believe Sightsavers' track record in implementing MDAs is moderately strong because implementation and monitoring for deworming programs is fairly similar to other NTD MDAs.
The evidence we have focused on includes:
- Coverage surveys: We believe the coverage surveys Sightsavers has shared with us provide the best evidence of its impact. While they have some methodological limitations, they indicate that Sightsavers is reaching a moderately high proportion of targeted recipients.
- Impact assessments: We have seen impact assessments of several of Sightsavers' trachoma and onchocerciasis programs; the assessments have significant methodological limitations and have not substantially shifted our view on Sightsavers' ability to support deworming programs. Sightsavers told us that it also conducted an impact assessment of its deworming work in Sokoto state, Nigeria in 2016;105 we have not received the results from Sightsavers.106
Details follow.
Coverage surveys
Sightsavers hires external consultants to conduct house-to-house coverage surveys of a sample of a population targeted for an MDA program, in order to estimate the proportion of the population targeted that actually received treatment.107 We have heard conflicting reports about how often Sightsavers conducts coverage surveys across its NTD portfolio, but our impression is that it does not have a regular schedule; it tends to only conduct coverage surveys after the first round of MDA or if it suspects there are issues with the program (e.g., because reports of coverage seem implausibly high or low).108 Sightsavers plans to conduct coverage surveys for deworming MDA projects supported by GiveWell-directed funds annually.109
Sightsavers has shared reports on its coverage surveys from Benin (2015), Togo (2015), Burkina Faso (2015), Côte d'Ivoire (2015), Cameroon (2015-16), South Sudan (2015), Nigeria (2014 and 2015), Malawi (2015) and Guinea (2017);110 however, we only have permission to share results from five of these surveys.
We summarize the methodologies of the publicly available coverage surveys we have seen from Sightsavers in this spreadsheet ("Methods" sheet). We note some limitations to the survey methodologies that impact our confidence in their accuracy and representativeness of treatment coverage in Sightsavers' MDA programs:
- Selection of geographic areas: Sightsavers' coverage surveys are implemented within specified geographic areas (e.g., districts, regions, or local government areas). It appears that geographic areas are often selected purposefully rather than randomly. For example, in the 2017 coverage survey in Guinea—the first coverage survey of an MDA that was funded with GiveWell-directed funds—the N'Zérékoré health district was chosen from three districts where MDAs occurred based on time constraints and ease of logistics.111 The 2015 coverage surveys in Benin and Togo do not specify why Abomey and Sotouboua districts were chosen for the survey.112 Details on the selection of geographic areas for all Sightsavers' coverage surveys are available in this spreadsheet, "Methods" sheet.
- Length of time between MDA and survey: For some of Sightsavers' coverage surveys, respondents are asked to recall taking drugs up to six months prior, which may have an impact on the accuracy of the responses; for some other surveys, the amount of time between the MDA and survey is not clear.113 Sightsavers told us that it aims to conduct all coverage surveys within 1-2 months of the MDA and that it does not believe recall bias is a serious concern.114
- Unclear data quality control processes: There is no mention in the coverage survey results of any re-surveying of households to check the accuracy of the data collected and, although several reports mention data quality verification, specifics are not given.115
Additionally, we note some limitations specific to certain surveys:
- There appear to be inconsistencies in the praziquantel coverage data from the 2014 coverage survey in Nigeria and in the report from the 2015 coverage survey in Malawi.116
- For the 2014 coverage survey in Nigeria, it appears that distribution of drugs for schistosomiasis was not yet fully completed at the time of the survey, so the surveys may underestimate coverage for the schistosomiasis part of the MDAs.117
For the results of these coverage surveys, see this spreadsheet, "Results" sheet.
Notes on these results:
- Coverage rates found in these surveys vary widely: from 40% coverage for ivermectin and albendazole in Benin from the 2015 survey, to 88% coverage for ivermectin and albendazole in the Northwest region of Cameroon from the 2015-16 survey.118 Sightsavers' 2017 Guinea coverage survey found a 58% coverage rate for praziquantel and albendazole. We place particular weight on these results because this survey is the only available coverage survey of an MDA that was funded with GiveWell-directed funds.119
- We do not believe the coverage surveys we have seen are representative of all of Sightsavers' NTD programs because we do not believe we have seen all of the coverage surveys Sightsavers has completed (or completed in a specific time frame)120 and because it is not clear how Sightsavers selects MDAs for surveys.
- For some areas with low coverage rates, the primary explanation given is that community distributors may not have been visiting all households.121 According to Sightsavers, the relatively low coverage rates found in Guinea in 2017 may have been affected by the timing of the survey, as children may have been traveling for the holidays.122
Impact assessments
We have reviewed three studies Sightsavers shared that reported on the impact of MDAs on the prevalence of onchocerciasis or of trachoma. The studies suggest that past treatment programs have been successful, but the studies have a number of limitations, particularly because it is unclear whether these programs are representative of Sightsavers' work and whether changes can be attributed, at least in part, to Sightsavers' work.
- A 2008 impact assessment of long-term (1991-2008) treatment of onchocerciasis in Kaduna, Nigeria:123 Baseline data from 1987 indicated a median onchocerciasis prevalence of 52%. In 2008, after 15-17 years of treatment, onchocerciasis prevalence had dropped to 0% in all surveyed communities (none of the 3,703 individuals screened were infected).124 Limitations of the study include: (1) the difficulty of attributing the change to Sightsavers' work given the possibility that other concurrent work or improvements during the long interval between baseline and follow up may have impacted onchocerciasis prevalence, (2) selection of study areas based on criteria that may be correlated with larger changes in prevalence, and (3) a high non-participation rate among targeted respondents.125
- A 2015 impact assessment of long-term (1993-2015) treatment of onchocerciasis in fifteen villages in three districts of Uganda:126 District-level onchocerciasis prevalence ranged from 0.8% to 5.5% at the time of the assessment.127 The authors noted that baseline prevalence data (from 2007) was available for only two of the fifteen villages,128 but they did not provide the baseline data from the two villages in the report. The study concluded that the MDAs performed well.129 Other limitations of the study are discussed in this footnote.130
- An impact assessment on three rounds of trachoma treatment (2009-2012) in three regions of Guinea-Bissau:131 Sightsavers has told us that it has run a trachoma program in Guinea-Bissau since 2011; we are uncertain about the details of Sightsavers' trachoma support in these three regions, and about the role other organizations play in this program.132 This study concluded that after three years of MDA, trachoma prevalence in children 1-9 years of age was below 5% in all three regions, indicating that further treatment was not needed.133 The study did not include baseline data (or state how much prevalence dropped). However, Sightsavers has elsewhere reported what may be comparable 2005 baseline data for these three regions, which suggests that trachoma prevalence decreased from 20-30% to 1-5% in these regions.134
Sightsavers also shared documents on impact assessments of an onchocerciasis control program in Kwara and Kogi states in Nigeria and another onchocerciasis control program in Kibaale District Uganda.135 We have not reviewed these documents in depth. A quick review led us to believe that they would not affect our views on Sightsavers' deworming programs.
We have not seen impact assessments of Sightsavers' schistosomiasis or STH programs specifically.136 Sightsavers told us that it completed an impact assessment of its deworming work in Sokoto state, Nigeria. We have not received the results.137
Are deworming programs operating as intended?
We do not have a good understanding of how often activities in Sightsavers-supported programs operate as Sightsavers intends and have not prioritized this question.
Sightsavers told us that its program supervisors conduct monitoring visits to check that program activities at national and local levels are being implemented as intended ("routine monitoring").138 Sightsavers has shared two of these routine monitoring reports covering programs in Nigeria in 2016 (one from a trip to Kebbi state, and another from a trip to Kogi state), as well as templates for quarterly and annual monitoring reports.139
The program supervisor conducting routine monitoring in Kogi State found that issues identified in the last monitoring visit had been addressed, the targeted number of teachers were trained on time, and program expenditures were on track to stay on budget.140
In Kebbi State, the program supervisor reported observing community drug distributors entering data and using dose poles; the report did not state whether or not community drug distributors were performing these activities appropriately.141
We have not seen other routine monitoring reports from Sightsavers, and are uncertain how often routine monitoring visits occur.142 Sightsavers has also told us that it has developed a Quality Standard Assessment Tool (QSAT) to assess (using checklists) whether programs are generally operating as intended.143 Sightsavers intends the QSAT reports to supplement the routine monitoring reports it has shared with us.144
What is the effect of Sightsavers' work on program outcomes?
Sightsavers may be having an impact in the following ways:
- It may increase the likelihood that a government implements a deworming program by advocating for deworming programs, by offering to provide technical assistance, and/or by funding implementation.
- It may improve the quality of a deworming program (leading to more children dewormed effectively or improved cost-effectiveness).
We have not yet asked Sightsavers for its guess as to what would have happened in the locations where it supports deworming programs if it had not provided support, so we have limited evidence on which to judge how Sightsavers affects programs. Sightsavers operates a program similar to the programs that Deworm the World Initiative and the Schistosomiasis Control Initiative operate, and much of our confidence that Sightsavers' technical assistance causes additional children to receive deworming treatments comes from what we have learned about those two organizations' models.
We would guess that Sightsavers increases the likelihood that (national and subnational) governments implement deworming, particularly when it pays for the majority of financial program costs.
We are uncertain about whether or not Sightsavers' assistance increases the quality of the programs it supports.
Are there any negative or offsetting impacts?
We discuss several possible considerations but do not see significant concerns.
Administering deworming drugs seems to be a relatively straightforward program.145 However, there are potential issues that could reduce the effectiveness of some treatments, such as:
- Drug quality: For example, if drugs are not stored properly they may lose effectiveness or expire.
- Dosage: If the incorrect dosage is given, the drugs may not have the intended effect and/or children may experience additional side effects.
- Replacement of government funding: We have limited information about whether governments would pay for the parts of the program paid for by Sightsavers in its absence. We also have little information about what governments would use deworming funds for if they did not choose to implement deworming programs.
- Diversion of skilled labor: Drug distribution occurs only once or twice per year and is conducted by volunteers in communities or teachers in schools. Given the limited time and skill demands of mass drug distribution, we are not highly concerned about distorted incentives for skilled professionals. Planning for the program can take senior government staff time; we are not sure what these staff would spend their time on in the absence of deworming programs, but suspect that they would support other education or health initiatives.
- Adverse effects and unintended consequences of taking deworming drugs: Our understanding is that expected side effects are minimal and there is little reason to be concerned that drug resistance is currently a major issue (more information from our report on deworming). We are somewhat more concerned about potential side effects during integrated NTD programs, since multiple drugs are taken within a short time period, but it is our understanding that organizations follow protocols to space out the treatments to sufficiently avoid adverse effects.
- Popular discontent: We have heard a couple of accounts of discontent in response to mass drug administration campaigns supported by the Schistosomiasis Control Initiative, including one case that led to riots.146 Additionally, during deworming activities supported by Evidence Action's Deworm the World Initiative in Ogun State, Nigeria in December 2017, rumors of students collapsing after receiving deworming pills reportedly generated panic that led some parents to take their children out of school; Ogun State government denied that any students collapsed.147 While the accounts we have heard are from programs supported by the Schistosomiasis Control Initiative and Evidence Action's Deworm the World Initiative, we think it is possible that other deworming programs could cause similar discontent.
What do you get for your dollar?
We estimate that on average the total cost of a schistosomiasis and/or STH treatment delivered in Sightsavers-supported programs is $1.19. Excluding the cost of drugs (which are often donated) and in-kind government contributions to the programs, we estimate that Sightsavers' cost per treatment is $0.55. These estimates rely on a number of uncertain assumptions. Full details of our analysis are in this spreadsheet. For results, see sheet "Overall cost per treatment."
When possible, we prefer to rely on past results over projected future results, as projections can be overly optimistic (as was the case for Sightsavers' projections in 2016—see below). For Sightsavers, we have used projected costs and treatments because we have limited past data—when we attempted to analyze the data we have seen from Sightsavers on treatments and costs from existing programs, we estimated a wide range of cost per treatments.148
Note that the number of lives significantly improved is a function of a number of difficult-to-estimate factors. We incorporate these into a cost-effectiveness model which is available here.
Our approach
Our general approach to calculating the cost per treatment is to identify comparable cost and treatment data and take the ratio. We prefer to have a broadly representative selection of costs and treatments in order to mitigate possible distortions, such as using data from a new program, which may incur costs from advocacy, mapping, etc. before it has delivered any treatments.
To get the total costs of the program, we attempt to include all partners such that our cost per treatment represents everything required to deliver the treatments. In particular, in our cost per treatment analysis for Sightsavers, we have attempted to include these categories:
- Sightsavers' costs from providing technical assistance or financially supporting a program.
- Value of donated drugs. We attempt to include the full market value of all praziquantel and albendazole that is needed to deliver the treatments.
- Costs incurred by the government implementing the program (e.g., for staff salaries when working on treatment programs). We do not have estimates from Sightsavers for these costs.
We start with this total cost figure and apply adjustments in our cost-effectiveness analysis to account for cases where we believe the charity's funds have caused other actors to shift funds from a less cost-effective use to a more cost-effective use ("leverage") or from a more cost-effective use to a less cost-effective use ("funging"). More discussion of leverage and funging in this blost post.
Shortcomings of our analysis
There are several ways in which our analysis of Sightsavers’ cost per treatment is uncertain:
- Limited data from previous deworming programs: We have only limited data from past programs that Sightsavers has supported with a deworming component. Additionally, Sightsavers has not broken down the costs of past programs such that we can see the cost of the deworming component alone. Instead, we have chosen to rely on Sightsavers' budgets and treatment number projections for how it expects to use GiveWell-directed funds in 2017-2019. These projections may turn out to be under- or overestimated, but have the advantage of directly modeling the types of programs that will be supported with additional GiveWell-directed funding. We have applied a small discount to the number of expected treatments based on Sightsavers' past coverage rates, as seen in coverage surveys.
- Integrated NTD programs: Sightsavers' NTD programs combine treatment for schistosomiasis and STH with other MDA programs, such as for onchocerciasis, trachoma, and lymphatic filariasis. In cases where Sightsavers is adding a deworming component to an existing MDA program, there are several approaches we could take:
- Only incorporate the additional costs of adding deworming into our cost per treatment analysis.
- Include the full cost of the integrated program and estimate the total benefits from all components of the program.
- Include the full cost of the integrated program, but only consider the benefits from deworming treatments.
Our preferred approach would be the second of these, but we are not currently able to do that analysis because (a) we do not have data from Sightsavers on the full costs of the integrated programs, and (b) we have not yet completed a full analysis of the benefits of MDA programs for other NTDs. We are currently taking the first approach, which may undercount costs that are shared across components of the program.
In cases where GiveWell-directed funds support the full costs of an integrated MDA program (e.g. in Benue state, Nigeria) we include the full costs of the program and count deworming treatments as the only benefits of the program.
- Limited data on partners' costs: We have very limited data on the contributions of Sightsavers' partners, particularly contributions from governments. We have data from third parties on the value of donated drugs. We do not have any direct information on the value of government staff or volunteer time used in the program; the approach we have taken to roughly estimate government contributions for Sightsavers' programs, as well as SCI-, END Fund-, and some Deworm the World-funded programs, is to base the estimate on a single, likely outdated study from an SCI-funded program.149
- Estimated number of treatments: We assume that consuming only albendazole, only praziquantel, or both counts as being dewormed. This is consistent with how we count the number of treatments delivered by SCI, Deworm the World, and the END Fund. Because we generally do not have detailed enough data from Sightsavers to determine what portion of children received only albendazole or only praziquantel, we have assumed that the figures we have received fully overlap within each country.150
- Possible excluded costs: Some costs might be excluded from our estimate because we are not sure what costs are included in the budgets Sightsavers has shared with us. For example, the following may not be included: start-up costs (e.g., for setting up operations in a new location), the cost of office space, and vehicle costs.151
Is there room for more funding?
Sightsavers has provided details of deworming programs that it could fund with additional funding of up to about $6.4 million in 2018 and 2019.152 We believe it is likely that Sightsavers could absorb funding beyond this amount to extend programs to 2020 and/or seek out additional opportunities to fund deworming programs.
In short, we calculate this from:153
- Total opportunities to spend funds productively: Sightsavers has identified $6.5 million worth of opportunities to:
- Add deworming to existing NTD programs ($2.8 million):154 This includes funds to extend commitments to 2019 for programs where GiveWell-directed funds have been committed to fund the programs through 2018, some funding for previously unanticipated 2018 costs for these programs, and new opportunities to add deworming to NTD programs.
- Fund integrated programs ($3.7 million):155 For these opportunities, GiveWell-directed funding would fund NTD programs that would treat several NTDs, including schistosomiasis and STH, in areas without current programs or where other funding sources are expected to expire.
- Cash on hand: Sightsavers has committed all of the GiveWell-directed funding that it has received to programs and has no other uncommitted funding on hand.156
- Expected additional funding: Sightsavers staff told us there is some possibility that the US and UK governments or a private funder that Sightsavers has had conversations with could fund some of the work included in the list of opportunities. We expect that Sightsavers will receive a small amount (~$70,000) due to being on GiveWell's top charity list (independent of specific funding recommendations we make).157
More detail in the sections below and in this spreadsheet.
December 2017 update: In November 2017, we recommended that Good Ventures give $2.5 million to Sightsavers' deworming program, reducing its room for more funding for 2018 and 2019 to about $3.9 million.
Below, we also discuss:
- Past spending: We have limited information about how Sightsavers has used unrestricted funding in the past, although we know only a small portion of unrestricted funding has supported its NTD programs in recent years.
- Additional considerations: Sightsavers is a large organization and funds multiple programs. GiveWell-directed donations to Sightsavers specifically support its deworming programs.
Available and expected funds
Our impression is that Sightsavers will not fund the work listed above from its unrestricted funds. There is a possibility that some of this work would be funded by restricted grants if Sightsavers does not receive sufficient GiveWell-directed funds.
When we first engaged with Sightsavers about the possibility of funding its deworming programs in 2015, it told us about opportunities to scale up deworming treatments in Nigeria and Guinea-Bissau.158 In 2016, Sightsavers had not made progress on scaling up deworming treatments in these areas because it had not received funding to do so.159 This increases our confidence that Sightsavers is unlikely to allocate its unrestricted funding to deworming programs in the absence of other donors, and that other donors are difficult to find.
In 2016, before we had directed funding to Sightsavers, Sightsavers provided us with a list of opportunities to scale up deworming treatments. We asked Sightsavers multiple times if it expected to fund any of these opportunities in the next year if it did not receive a recommendation from GiveWell; Sightsavers told us that it would not, because:160
- Sightsavers does not expect to use significant amounts of its unrestricted funding to scale up deworming treatments. Deworming programs are not Sightsavers’ highest priority and there are many other demands on Sightsavers' limited amount of unrestricted funding.
- Sightsavers would be surprised if it were to receive enough restricted funding from another donor to scale up deworming. Sightsavers has not yet seen significant interest from large donors in funding the deworming programs it discussed with us. This may be because, according to Sightsavers and other deworming groups we've spoken to, two of the largest donors for NTD programs, the US and UK governments, are primarily interested in funding NTD programs that are focused on lymphatic filariasis, onchocerciasis, and trachoma.
In 2017, we again asked Sightsavers about other potential funders for deworming. It mentioned four possible funders:
- USAID, which has been funding MDAs for several NTDs in Cameroon through the ENVISION project. USAID has informed partners that it will provide limited support for SCH/STH impact surveys in 10-12 selected areas in Cameroon, but that starting in 2018 it will not support SCH/STH MDAs. Sightsavers is seeking funding to support activities in areas where USAID has withdrawn ENVISION funding.161
- The UK government's Department for International Development announced in 2017 that it will increase support for NTDs.162 The first grants from this round of funding are expected in early 2019.163
- Sightsavers has been in conversations with a private funder and has discussed the possibility of that funder supporting the Cameroon program.164
- Sightsavers has had early conversations with another potential funder about the potential for a very large contribution for NTDs. Our impression is that it is unclear whether a portion of it could be used for deworming.165
We expect that Sightsavers will receive a small amount of funding (~$70,000) due to being on GiveWell's top charity list (independent of specific funding recommendations we make). This projection is based on what Sightsavers received last year from donors who cited GiveWell as their reason for giving, excluding the grant we recommended Good Ventures make to Sightsavers.166
Uses of additional funding
Sightsavers has provided us with a list of opportunities it hopes to raise funding for, which consist of supporting deworming MDAs, and in some cases other NTD MDAs, in four countries: three of the four in which GiveWell-directed funds are funding MDAs in 2017 (DRC, Guinea, and Nigeria), plus Cameroon. We have summarized the opportunities in this spreadsheet ("Spending opportunities" sheet).167
In short, Sightsavers is seeking funding for the following, listed in the order of GiveWell's prioritization:
- Additional costs for previously-funded 2018 programs ($0.7 million): Over the course of 2017, Sightsavers has found that more resources are necessary for programs that have been funded with GiveWell-directed funds than it had budgeted for. It is seeking additional funds for these programs in 2018.168
- Extension of commitments for current programs that add deworming to existing programs through 2019 ($1.2 million): GiveWell-directed funds have been used to commit to adding deworming to programs in DRC (Ituri Nord),169 Guinea,170 and Nigeria (4 states)171 through 2018. Additional funds would allow Sightsavers to continue those programs through 2019.
- Adding deworming to existing programs in new geographies ($1.0 million): Sightsavers is seeking funding to add deworming to other NTD work in Yobe state, Nigeria (with more frequent treatment than recommended by WHO)172 and five additional districts in Guinea.173
- Integrated NTD programs ($3.7 million): Sightsavers is seeking funding to extend work to 2019 in Benue state, Nigeria (which has been previously funded with GiveWell-directed funds through 2018);174 to start new programs in Bauchi state, Nigeria175 and Ituri Sud, DRC;176 and to replace USAID funding177 in Cameroon.178
In total, Sightsavers would need about $6.5 million to fund all of the work in the above list.179 We believe it is likely that Sightsavers could use more than $6.5 million to deliver additional deworming treatments. It could use additional funds to extend commitments to current programs to 2020 and beyond and it might seek out additional opportunities to scale.
Past uses of unrestricted funding
We have some high-level data from Sightsavers on its past uses of unrestricted funding. In 2016, Sightsavers spent about $49 million in unrestricted funding. About 50% of this went to fundraising (about $25 million) and about 6% was spent on Sightsavers' NTD program (about $2.7 million), down from 9% ($4.7 million) in 2015. Aside from this decrease, Sightsavers' 2015 expenditures were similar.180
Sightsavers has supported some deworming treatments with unrestricted funding in the past. However, given limited amounts of unrestricted funding, Sightsavers has told us that it does not expect to use much additional unrestricted funding in the future to support new or larger deworming programs.181
Additional considerations relevant to assessing Sightsavers' room for more funding
- Sightsavers is a large organization and spends money on many programs that are not deworming, including other NTDs, eye health, education, cataract surgeries, job training for the disabled, and more. Because deworming programs are not a major priority for Sightsavers in its use of unrestricted funding, we have asked Sightsavers to use GiveWell-directed funding to support scale-up of deworming (including central costs needed to support such an increase in programming). Donors who would like their donation to Sightsavers to support deworming should consider giving to GiveWell for the support of Sightsavers' deworming work or, if giving directly to Sightsavers, communicating to Sightsavers that their gift was due to GiveWell's recommendation.
- For the funding opportunities listed above, Sightsavers has requested funding to allow it to commit funding for the following two years. We ask top charities to consider GiveWell-directed funds to be multi-year grants. The amount of GiveWell-directed funding that a top charity receives can vary greatly from year to year, and spending the funds over two to three years can help smooth these fluctuations. Sightsavers also told us that it is easier to work with governments and communities if it can commit to working multiple years. This is also something that the Deworm the World Initiative has argued.
Global need for treatment
There appears to be a substantial unmet need for STH and schistosomiasis treatment globally.
In 2017, the World Health Organization (WHO) released a report on 2016 treatments stating that:182
- 69% of school-age children in need of treatment were treated for STH in 2016, up from 63% in 2015 and 45% in 2014. Coverage was 65% in African countries in 2016, up from 51% in 2015 and 45% in 2014.
- 52% of school-age children in need of treatment were treated for schistosomiasis in 2016, up from 42% in 2015.
We have not vetted this data.
Sightsavers as an organization
We have spent less time investigating Sightsavers and have less insight into its activities and track record than we do for top charities we have followed for many years. As such, we have a limited view on the qualities below.
- Track record: Sightsavers has a limited track record of assisting governments with deworming programs, but a stronger track record of assisting governments with integrated NTD programs.
- Self-evaluation: Sightsavers' self-evaluation is strong compared to the vast majority of organizations we have considered. That said, this evidence is incomplete and has methodological limitations.
- Communication: We have not spent as much time communicating with Sightsavers as we have with the charities we have recommended for several years. To date, Sightsavers has generally communicated reasonably clearly with us.
- Transparency: Sightsavers has allowed us to publish most of the information it has shared with us.
More on how we think about evaluating organizations at our 2012 blog post.
Sources
{kind=link}
- 1
- GiveWell's non-verbatim summary of a conversation with Susan Walker and Katie Cotton, February 26, 2015
- GiveWell's non-verbatim summary of a conversation with Sightsavers staff, March 19, 2015
- GiveWell's non-verbatim summary of a conversation with Sightsavers staff, April 5, 2016
- GiveWell's non-verbatim summary of a conversation with Julia Strong, Dr. Imran Khan, and Mike Straney, April 14, 2016
- Sightsavers staff, conversation with GiveWell, September 6, 2016
- GiveWell's notes from its 2016 site visit to Ghana
- Sightsavers staff, conversation with GiveWell, October 2, 2016
- We have also had additional conversations for which we have not produced conversation notes.
- 2
"Sightsavers is one of the world’s leading non-profit organizations dedicated to combating avoidable blindness and promoting equal opportunities for people with disabilities in developing countries. We work with local partners in over 30 countries in Africa, Asia and the Caribbean, restoring sight through specialist treatment and eye care. We also support people who are irreversibly blind by providing education, counselling and training." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 1.
- 3
Of Sightsavers' 2016 total expenditure excluding gifts in kind, 75% was spent on program activities ("charitable activities," i.e. activities other than fundraising), including 35% on NTDs; NTDs accounted for about 47% of program expenditure (excluding gifts in kind) and 85% of total expenditure including gifts in kind.
Sightsavers, Finances 2016 actual and 2017 planned, Sheet "Organisational expenditure", columns F and G.
- 4
- "Currently, Sightsavers only wants to add deworming programs in countries where it already has an NTD program." GiveWell's non-verbatim summary of a conversation with Sightsavers staff, March 19, 2015, Pg 6.
- "Sightsavers takes an integrated approach to NTD elimination, as it is the most cost-effective, efficient and sustainable approach. Sightsavers has well established programs supporting the elimination of river blindness, trachoma and lymphatic filariasis (LF), and is leading efforts to scale up integrated treatments where needed, and to integrate deworming where possible." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 2.
- "STH is more problematic as it has the potential to be an indefinite control programme (until current treatment strategy changes; this will be a long way off) and we would only continue with STH support as part of school health programmes which also include eye health." Sightsavers, Now is the time to say goodbye to neglected tropical diseases, Pg 13.
- "We will confine our geographic spread in NTD work to Africa. There are three exceptions to this strategic choice: if funding is available to support trachoma and onchocerciasis in Yemen we will expand there; if we are invited or we choose to bid for contract management work globally we will undertake work outside Africa; and, if NTD work is linked to a programme covering other work ... we would seize this as an opportunity." Sightsavers, Now is the time to say goodbye to neglected tropical diseases, Pg 11.
- 5
See Sightsavers, Deworming program consolidated logframe, September 2017 update.
- 6
For more information on MDAs, see this justification for MDAs from Evidence Action's Deworm the World Initiative (another GiveWell top charity with a focus on deworming programs): "Is mass treatment justified? On cost-effectiveness grounds we believe that it clearly is, as the cost of treatment is cheaper than individual screening. The WHO states that the cost of screening is four to ten times that of the treatment itself. Because the drugs are very safe and has no side effects for the uninfected, the WHO does not recommend individual screening. The WHO instead recommends mass drug administration in areas where more than 20% of children are infected." Evidence Action website, Deworm the World Initiative (March 2016).
- 7
Julia Strong, International Foundations Executive, edits to GiveWell's draft 2017 review, November 14, 2017.
- 8
"It was on 5 Jan 1950 that the doors of the British Empire Society for the Blind, as we were known back then, opened for the first time. [...] As well as being the decade of teddy boys, petticoats and rock and roll, the 1950s were when Sightsavers made our first groundbreaking achievement in the fight against avoidable blindness. In 1953 a survey was conducted by Dr Freddie Rodger in West Africa. It showed that the majority of blindness was actually preventable, and led to a pioneering disease control programme for onchocerciasis, also known as river blindness." Sightsavers, Our history.
- 9
"In 2015, Sightsavers supported approximately 252,000 cataract surgeries through 55 projects in roughly 20 countries. Its larger cataract projects are located in Southeast Asia (for example in Bangladesh, India, and Pakistan), and it also has projects in Sub-Saharan Africa. Sightsavers works with governments to strengthen countries' cataract surgery systems. It also seeks to integrate this work with its eye health-related neglected tropical disease programs." GiveWell's non-verbatim summary of a conversation with Julia Strong, Dr. Imran Khan, and Mike Straney, April 14, 2016, Pg 1.
- 10
- "Our work also covers low vision, diabetic retinopathy, childhood blindness and the group (17 diseases in total) known as neglected tropical diseases, which incorporates not only trachoma and river blindness, but also buruli ulcer, Chagas disease, dengue/severe dengue, dracunculiasis, echinococcosis, foodborne trematodiases, human african trypanosomiasis, leishmaniasis, leprosy, lymphatic filariasis, rabies, schistosomiasis, soil transmitted helminthiases, taeniasis/cysticercosis and yaws." Sightsavers, What We Do - Sight
- "Integrated NTD programs (including deworming, when it is needed) represent just one of Sightsavers’ top priorities. For the past few years, programs for trachoma and onchocerciasis have been specifically identified as “fast-track” initiatives. Sightsavers has historically been known for providing services such as cataract surgery, ophthalmologist training, and hospital support, but it aims to make its NTD work as much as or even more of a priority than its traditional work." GiveWell's non-verbatim summary of a conversation with Susan Walker and Katie Cotton, February 26, 2015, Pgs 4-5.
- 11
- "Though we were undertaking small-scale lymphatic filariasis (LF) work as early as 2007, it was only in 2010 that we recorded our first LF treatment, followed by schistosomiasis and soil transmitted helminths (STH) in 2011." Sightsavers, Now is the time to say goodbye to neglected tropical diseases, Pg 9.
- Additional detail: "In 2011 we responded to the international call to scale up NTD treatments by developing ‘fast track initiative’ disease-specific programmes (now called our ‘flagship programmes’) covering onchocerciasis and trachoma. In 2016 we ensured the integration of LF into our onchocerciasis plans." Sightsavers, Now is the time to say goodbye to neglected tropical diseases, Pg 9.
- "The mandate of the organization and Royal Charter was changed in 2009 to accommodate the non-blinding NTDs. It was only in 2010 that Sightsavers recorded its first non-blinding neglected tropical disease treatment (LF, followed by schistosomiasis and STH in 2011) in its output statistics." GiveWell's non-verbatim summary of a conversation with Sightsavers staff, March 19, 2015, Pg 3.
- "Though we were undertaking small-scale lymphatic filariasis (LF) work as early as 2007, it was only in 2010 that we recorded our first LF treatment, followed by schistosomiasis and soil transmitted helminths (STH) in 2011." Sightsavers, Now is the time to say goodbye to neglected tropical diseases, Pg 9.
- 12
Julia Strong, Sightsavers International Foundations Executive, edits to GiveWell's draft 2017 review, November 14, 2017.
- 13
- "We have long been committed to the elimination of devastating neglected tropical diseases (NTDs). Sightsavers’ earliest work was in Ghana in the 1950s, where our Founder Sir John Wilson, Dr Geoffrey Crisp and Dr Freddie Rodger initially led the first ever surveys into the extent and transmission of river blindness and the introduction of rehabilitation services for people who are irreversibly blind. Sightsavers has also been involved in the control of trachoma since 1952, working with partners in 35 countries." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 1.
- Sightsavers believes that there can be significant efficiency gains from integrated NTD programs.
- "We support integration and coordination of NTD programmes in countries in which we are active to reach elimination goals within NTD national master plans." Sightsavers, Now is the time to say goodbye to neglected tropical diseases, Pg 11.
- We write more about the benefits Sightsavers believes come from integrated programs in our site visit notes: GiveWell's notes from its 2016 site visit to Ghana
- 14
- Sightsavers, Now is the time to say goodbye to neglected tropical diseases, Pg 7.
- "We have no intent to get involved with the Innovative and Intensified Disease Management (IDM) diseases, focusing on diseases for which cost-effective control tools do not exist and where large-scale use of existing tools is limited. Those diseases include buruli ulcer, chagas disease, human African trypanosomiasis and leishmaniasis. However, we will coordinate with others who work in this area if we note that these diseases are endemic and underserved in our operational target areas." Sightsavers, Now is the time to say goodbye to neglected tropical diseases, Pg 12.
- "Before taking his current role, Mr. Bush was Sightsavers’ Regional Director for West Africa. During this time, Sightsavers was beginning to expand its NTD work, which had historically focused on onchocerciasis and trachoma, into integrated preventive chemotherapy and transmission control (PCT) programs for other NTDs, including lymphatic filariasis (LF), soil‐transmitted helminthiasis (STH), and schistosomiasis." GiveWell's non-verbatim summary of a conversation with Sightsavers staff, March 19, 2015, Pg 1.
- 15
- See, for example, the London Declaration to move towards elimination and control of 10 NTDs by 2020.
- "This is a critical area and there is a choice to be made here: either continue with control or work towards elimination. This plan assumes that elimination is the goal and Sightsavers wants to become one of the premiere NGOs in elimination programmes." Sightsavers, Now is the time to say goodbye to neglected tropical diseases, Pg 13.
- GiveWell's notes from its 2016 site visit to Ghana
- 16
- We have heard this from conversations with several organizations working on deworming or integrated NTD programs.
- GiveWell's notes from its 2016 site visit to Ghana
- "To achieve and sustain elimination we must promote multi-sectorial integration and proactively develop strategic partnerships in all areas of work. For example, soil transmitted helminths (STH) programmes need to go beyond schools if national control targets are to be met. STH is more problematic as it has the potential to be an indefinite control programme (until current treatment strategy changes; this will be a long way off) and we would only continue with STH support as part of school health programmes which also include eye health. Onchocerciasis, lymphatic filariasis (LF) and trachoma elimination programmes, which are traditionally community focused, should also look towards school programming to achieve their elimination targets." Sightsavers, Now is the time to say goodbye to neglected tropical diseases, Pg 13.
- 17
- "Currently, Sightsavers only wants to add deworming programs in countries where it already has an NTD program." GiveWell's non-verbatim summary of a conversation with Sightsavers staff, March 19, 2015, Pg 6.
- Sightsavers staff, conversation with GiveWell, September 6, 2016
- 18
- "Many of Sightsavers’ MDA programs provide a hybrid of school‐based treatment (in which drugs are administered at school sites) and community‐based treatment (in which drug distributors travel from house to house in a community). School‐based treatment tends to be used in areas where school enrollment is high. In areas where STH and LF are co‐endemic, if LF is treated on a community level, deworming is achieved at the same time." GiveWell's non-verbatim summary of a conversation with Susan Walker and Katie Cotton, February 26, 2015, Pg 7.
- The CDD does not watch people apply or swallow their treatments. Rather, when the CDD visits a household, the CDD asks how many people live in that household and leaves the appropriate number of treatments with someone who was home during the visit. That person is then expected to distribute the treatments to the rest of the family. Grace Hollister, Global Director of Deworm the World Initiative, conversation with GiveWell, August 11, 2016
- Example from Nigeria (we don't know whether this is true elsewhere): "Where community based approaches are used, the community decides themselves whether it is house to house or fixed point." Sightsavers, Responses to GiveWell questions, October 2017, Pg 1.
- 19
This understanding comes from many conversations with representatives from non-governmental organizations (NGOs) supporting NTD programs.
- 20
- "Programmes are planned to avoid children being treated twice. In some cases this is
achieved through the different strategies (school versus community based) being
used in different implementation units. Where both strategies are used in the same area specific efforts are made to ensure an appropriate level of mass sensitisation and
in some cases markers are used. [...] [In Nigeria] in a few instances (and not most) where school coverage is very low, school and community based strategies are both used (to reach children at Islamic schools or out of school children etc). In these areas a marker is placed on the children to avoid treating them twice. [...] [In Guinea Conakry] children are asked if they’ve been treated before." Sightsavers, Responses to GiveWell questions, October 2017. - During a visit to Sightsavers' office in Guinea Conakry in October 2017, Sightsavers staff told us that children's fingernails had been marked to indicate that they had received deworming pills. Notes from a site visit to Sightsavers in Conakry, Guinea in October 2017, Pg 2.
- "Programmes are planned to avoid children being treated twice. In some cases this is
- 21
- "Sightsavers has well established programs supporting the elimination of river blindness, trachoma and lymphatic filariasis (LF), and is leading efforts to scale up integrated treatments where needed, and to integrate deworming where possible. We integrate deworming into programs where we are able to meet two key criteria:
- 1. That evidence from mapping on co-endemicity with other NTDS demonstrates that it is desirable and feasible to integrate deworming, thus improving quality of life and school attendance, as well as equitable access to medicines and the cost-effectiveness of the program.
2. That Sightsavers is able to source the funding required to integrate deworming into the program. Like many NGOs, Sightsavers’ unrestricted income is under substantial
pressure and is subject to competing priorities. We are therefore better able to integrate deworming activities into programs if we have restricted funding available for deworming activities. This is a key reason why the support of GiveWell would make a significant difference to our ability to deliver deworming activity on a larger scale."Sightsavers, Descriptions of current work - 2015 and 2016, Pg 2.
- "Before Sightsavers commences support to any partner, including government partners, it undertakes a due diligence assessment in a participatory manner with the partner. We use tools we have developed which have been tested and modified over a number of years. The tools assess the vision, goals, human resource, financing and risks of the partner, and are shared with them in advance of the assessment.
During the assessment, we ask the partner a series of questions, review the evidence and jointly grade the answers using a grading scale. After the assessment a strengths, weaknesses, opportunities and threats (SWOT) analysis is undertaken and a capacity development plan is developed, with timelines. Capacity development is then assessed annually to determine progress to ensure the partner is empowered to deliver on agreed objectives and systems are established to minimise risks.
We assess Sightsavers’ capacity to implement in terms of skills, human resource
and the availability of funding (see point 2 above). Where necessary, we recruit additional project staff to support implementation for the period of the project and identify institutions, consultants and coalitions with whom we wish to work for technical support." Sightsavers, Approach to deciding where to support deworming
- "Sightsavers has well established programs supporting the elimination of river blindness, trachoma and lymphatic filariasis (LF), and is leading efforts to scale up integrated treatments where needed, and to integrate deworming where possible. We integrate deworming into programs where we are able to meet two key criteria:
- 22
"Sightsavers’ country programs work with a country’s ministry of health (MOH) to identify implementation units (such as districts) in need of MDAs for each disease. This determination is based on data about the disease’s prevalence in the area obtained through mapping...Sightsavers uses mapping data to establish baseline prevalence for a particular disease in the area. It then uses guidelines from the World Health Organization (WHO) to determine what drug regime is needed in areas where prevalence exceeds minimum thresholds." GiveWell's non-verbatim summary of a conversation with Susan Walker and Katie Cotton, February 26, 2015, Pgs 1-2.
- 23
"Sightsavers has Memorandums of Understanding in place with Ministries of Health in the countries we work in and Sightsavers staff teams work in direct collaboration with Government ministry staff and partner organizations on all program activity. Sightsavers works closely with frontline service delivery teams and is in a unique position to influence and advocate effectively to Government partners." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 1.
- 24
- GiveWell's notes from its 2016 site visit to Ghana
- "The country director advocates government domestic spending on NTD programs, and initiation or prioritization of certain NTD programs by the Ministries of Health and Education." GiveWell's non-verbatim summary of a conversation with Sightsavers staff, April 5, 2016, Pg 1.
- 25
- "The key to this integration is supporting in-country ownership by working with national NTD Master Plans. NTD Master Plans need to be of good quality and based on recent robust prevalence data both for planning and for progress tracking – hence initiatives like Tropical Data. We have a role to play in supporting the development of these quality, comprehensive and budgeted master plans, including involvement in the renewal of existing plans and need to support capacity to deliver this crucial area of work. National NTD task forces need to own these plans and be vibrant and supported to deliver. Where required we can support these task forces financially – the country, however, must remain in the leadership position." Sightsavers, Now is the time to say goodbye to neglected tropical diseases, Pg 12.
- For example, in Nigeria: "Sightsavers supports the national and state NTD teams for better program coordination at various levels. Support is also provided to the National NTD Steering Committee which provides a forum for discussing the overall strategic direction for the national NTD program. At the local government area level Sightsavers has facilitated the establishment of NTD Task Force committees which has improved ownership of the program." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 3.
- In Cameroon: "Community participation is observed at every stage of program implementation. Community representatives took part in planning meetings at national, regional and district level. At health area level, community meetings were held before the campaign began. This led to increased community awareness and ownership of the program so communities understood their roles and responsibilities during MDA." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 13.
- GiveWell's notes from its 2016 site visit to Ghana
- "Sightsavers provides funding to and works with in-country partners, such as national NGOs and governments, to identify programming gaps, develop plans and budgets, and provide the necessary support for program implementation." GiveWell's non-verbatim summary of a conversation with Sightsavers staff, April 5, 2016, Pg 1.
- This sometimes includes sharing project management tools that Sightsavers has developed.
- "Sightsavers has entered into relationships with Schistosomiasis Control Initiative (SCI), Liverpool School of Tropical Medicine, London School of Hygiene and Tropical Medicine, and the Kilimanjaro Centre for Community Ophthalmology to provide technical advice and operational research to improve our programmes. With SCI and Liverpool we have arrangements where we also support them with implementation and financial management." Sightsavers, Now is the time to say goodbye to neglected tropical diseases, Pg 20.
- "We will work to leverage existing tools to add value to other Sightsavers programmes. Our suite of bespoke tools developed for programme management of the large grants (e.g. CLAIMS, project management tool for the UNITED programme in Nigeria, etc.) and tools developed for the consortia programmes could be cross-purposed to support other programmes, particularly when matched to tools such as Quality Standards Assessment Tool (QSAT). These systems should create efficiencies and not more work for country staff." Sightsavers, Now is the time to say goodbye to neglected tropical diseases, Pg 17.
- 26
- "With the support of the Children’s Investment Fund Foundation (CIFF), DFID and USAID, 19 states and the federal capital territory were mapped for schistosomiasis and STH from November 2013 to May 2015. CIFF provided funding to map 14 states and the remaining states were supported by the DFID funded Global Trachoma Mapping Project, RTI/ENVISION project and Sightsavers." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 7.
- "We were recently nominated by a group of organizations with expertise in the fields of NTDs and water and sanitation to lead a global project to map trachoma. This was the largest infectious disease survey ever undertaken and the project came to a close in 2015 as the 29th country was mapped." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 1.
- "Sightsavers’ country programs work with a country’s ministry of health (MOH) to identify implementation units (such as districts) in need of MDAs for each disease. This determination is based on data about the disease’s prevalence in the area obtained through mapping. Sightsavers may conduct the mapping itself, or it may be done by other organizations. For example, Sightsavers has received funding from the Children’s Investment Fund Foundation (CIFF) to map the prevalence of schistosomiasis and soil-transmitted helminthiasis (STH) in Nigeria. Sightsavers also coordinates the Global Trachoma Mapping Project (GTMP), funded by the U.K.’s Department for International Development (DFID), which has supported a great deal of trachoma mapping." GiveWell's non-verbatim summary of a conversation with Susan Walker and Katie Cotton, February 26, 2015, Pgs 1-2.
- 27
- In Nigeria: "Sightsavers and the state NTD teams engage with the Ministry of Education and Qur’anic and Basic Education Boards to plan and deliver teacher training." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 4.
- In Cameroon: "Sightsavers’ training activities are focused on training of government health personnel, who are employed as civil servants and carry out project activities. Program staff are supported to develop competences and skills through trainings and workshops." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 9.
- GiveWell's notes from its 2016 site visit to Ghana
- "In-country staff provide district-level authorities with program implementation support. Depending on the program, this might include supporting community distributors, doing information and education work around behavior change, or providing support for training, program monitoring and supervision, or data collection and analysis." GiveWell's non-verbatim summary of a conversation with Sightsavers staff, April 5, 2016, Pg 2.
- Julia Strong, International Foundations Executive, edits to GiveWell's review, November 9, 2016
- 28
"On shipment, drugs are initially delivered to National Central Medical Stores in Lagos. Drugs are then distributed to Sightsavers-supported State Ministry of Health Central Medical Stores, and through the health system to local government area medical stores for delivery in Sightsavers’ target areas." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 4.
- 29
- In Cameroon:
- "This is spearheaded by a large-scale sensitization and mobilization campaign during which all stakeholders are mobilized." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 10.
- "Please note: In North West region, the number of school aged children treated was exceeded as intensified sensitization and mobilization at community level enabled us to reach children not enrolled in school." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 11.
- "We supported a wide program of community awareness activities to encourage communities to accept treatment. Activities included trainings and community meetings…" Sightsavers, Descriptions of current work - 2015 and 2016, Pg 12.
- "In-country staff provide district-level authorities with program implementation support. Depending on the program, this might include supporting community distributors, doing information and education work around behavior change, or providing support for training, program monitoring and supervision, or data collection and analysis." GiveWell's non-verbatim summary of a conversation with Sightsavers staff, April 5, 2016, Pg 2.
- In Cameroon:
- 30
"Our quality standards manual is operationalised via the QSAT (our quality standards assessment tool). It is during a QSAT exercise that Sightsavers will review the listed means of verification per requirement, and rate each accordingly. A QSAT exercise may be conducted at one or more points of a project, including baseline, during implementation or at evaluation. When QSATs are required is established at the design phase of a project. To support a QSAT exercise, Sightsavers has developed means of verification guidance per technical theme. This guidance is to help an assessment team make a rating decision as it outlines what Sightsavers expects for a requirement to achieve a rating of fully met, mostly met and so on. The review of the means of verification is conducted at the source location. Where an interview is a means of verification, a list of questions to be asked should be agreed at the QSAT planning stage." Comment provided by Sightsavers in response to a draft of this page in November 2017.
- 31
- "Sightsavers’ selection criteria for Treatment coverage surveys: It will not be possible to conduct the survey after every round of MDA but if there is funding it is recommended a coverage survey is conducted:
- After the first round of MDA in an area
- If there are suspected issues with the health system or Community Health Worker (CHW) records or census data that need to be verified e.g poor population data, discrepancies between the drug store records/logs and the Community health Worker records or large variations in doses given year to year
- If the health system or Community Health Worker records show particularly low coverage e.g less than 60% or high coverage e.g 95 to over 100%
- If there have been issues in the area of operation with MDA coverage reporting in the past"
Julia Strong, International Foundations Executive, edits to GiveWell's review, November 9, 2016
- "Dr. Elhassan noted that Sightsavers has always followed a WHO protocol recommending that coverage surveys be conducted at a program's 1-, 3-, and 5-year marks." GiveWell's notes from its 2016 site visit to Ghana, Pg 6.
- "Sightsavers’ selection criteria for Treatment coverage surveys: It will not be possible to conduct the survey after every round of MDA but if there is funding it is recommended a coverage survey is conducted:
- 32
Sightsavers originally planned to conduct coverage surveys every 1-2 years and on our request plans to increase that to all MDAs (i.e., annually). In some cases, this will require additional GiveWell-directed funding in 2017-2018.
- See "Output Indicator 2.3: Number of treatment coverage surveys conducted with data disaggregated by age group and gender and school attendance" and cells E123-129, G123-129, Sightsavers, Deworming program consolidated logframe, September 2017 update, Sheet "Consolidated."
- "[GiveWell:] Would it be feasible to do coverage surveys in for MDAs in 2018 as well? None are currently scheduled. Approximately, how much would this cost (so we can add it to the wishlist)?
[Sightsavers:] Treatment coverage surveys have been partially budgeted for in Sightsavers’ new wishlist recently submitted to GiveWell, as such:- Guinea Conakry - TCS are included in our 2018 and 2019 wishlist budget requests
- Cameroon – TCS are included in our 2018 and 2019 wishlist budget requests
- DRC – TCS are included in our 2018 and 2019 wishlist budget requests
- Nigeria Bauchi State – TCS are included in our 2018 and 2019 wishlist budget requests
- Nigeria Yobe State - TCS are included in our 2018 and 2019 wishlist budget requests
However, we omitted to include TCS for each individual state in the Nigeria 4 States project, and also in the Benue state project. For these to be added into the programs in 2018, Sightsavers would wish to request the following additional funding added into our wishlist request. [...] Looking ahead, we would wish to add 2019 TCS budget requests for the same locations into a 2019 wishlist, should this become a possibility." Sightsavers, Responses to GiveWell questions, October 2017, Pg 2.
- 33
- Other types of monitoring we've heard that Sightsavers uses include: prevalence surveys at sentinel sites, quality standard assessment tools, and spot checks of randomly selected projects. GiveWell's non-verbatim summary of a conversation with Susan Walker and Katie Cotton, February 26, 2015, Pg 1. More detailed descriptions of monitoring can be found on Pgs 1-4.
- "Assessing the impact of treatment programs on schistosomiasis and STH prevalence levels generally requires conducting pre- and post-treatment prevalence surveys. However, for routine programming, treatment plans are based on prevalence mapping results, and post-treatment surveys are unlikely to be undertaken, particularly while the program is ongoing. As treatments are effective when taken properly, high coverage rates likely result in a reduction in prevalence levels over time." GiveWell's non-verbatim summary of a conversation with Sightsavers staff, April 5, 2016, Pg 3.
- 34
Comment provided by Sightsavers in response to reviewing a draft of this page in November 2016.
- 35
See our review of SCI.
- 36
We note that Sightsavers has advised it will provide the results by the end of 2017: Julia Strong, Sightsavers International Foundations Executive, edits to GiveWell's draft 2017 review, November 14, 2017.
- 37
- GiveWell's notes from its 2016 site visit to Ghana
- "Sightsavers provides funding to and works with in-country partners, such as national NGOs and governments, to identify programming gaps, develop plans and budgets, and provide the necessary support for program implementation." GiveWell's non-verbatim summary of a conversation with Sightsavers staff, April 5, 2016, Pg 1.
- 38
- 39
- GiveWell's notes from its 2016 site visit to Ghana
- "Government partners fund the salaries of their staff who work on the program, and agree to contribute a certain proportion of domestic funding to ensure the program's sustainability." GiveWell's non-verbatim summary of a conversation with Sightsavers staff, April 5, 2016, Pg 1.
- 40
These budgets are supposed to provide enough detail for Sightsavers to know, for example, what the programs are paying in per diems. GiveWell's notes from its 2016 site visit to Ghana
- 41
- GiveWell's notes from its 2016 site visit to Ghana
- "Sightsavers has been working in Nigeria for over 40 years, in partnership with the Ministry of Health. During this time we have supported eye care programs to address conditions amongst the population including cataract and glaucoma, human resource development programs to increase the number of practising ophthalmologists, cataract surgeons and eye health professionals, and widespread NTD programs focused on the elimination of five NTDs." Sightsavers, Nigeria NTD program information prepared for GiveWell, May 2015, pg. 1.
- "Nigeria is the country in which Sightsavers began its deworming programs and has been the flagship country for the organization’s integrated approach. Since 2011, when Nigeria’s deworming treatment program started in Zamfara and Sokoto states, Sightsavers has provided a total of about 14 million treatments per year for STH, and around 3 million treatments per year for schistosomiasis." GiveWell's non-verbatim summary of a conversation with Susan Walker and Katie Cotton, February 26, 2015, Pg 6.
- 42
- "Nigeria – 4 states: Kebbi, Kogi, Kwara and Sokoto states … Duration of project: 2 Years, in the first instance, January 2017 – December 2018", Sightsavers, GiveWell Project Narrative, Nigeria Four States 2017, Pg 1.
- "Project name: Benue State Nigeria GiveWell Integrated NTDs Programme … Duration: 2 Years, in the first instance, January 2017 – December 2018", Sightsavers, GiveWell Project Narrative, Benue State Nigeria 2017, Pg 1.
- For project history, see the charts in Sightsavers, Descriptions of current work - 2015 and 2016, Pgs 4 and 6.
- 43
- "SCH and STH MDA generally uses a school based treatment strategy in all LGAs, and community based treatments in those LGAs with a prevalence rate of over 50%. Due to learning arising from this project, we have changed to a combination of school and community based treatments in all states in order to target out-of-school children. This is particularly important in areas where enrolment in public schools is low, for example in Northern states where the majority of children attend Islamic schools." Sightsavers, Country narrative report, Nigeria Four States, Pg 1.
- "Output 2 - Treat school aged children between 5-15 years for STH and for schistosomiasis through MDA. … Activities … Conduct monitoring and supportive supervision of school based and community based MDA.", Sightsavers, GiveWell Project Narrative, Nigeria Four States 2017, Pg 6.
- 44
- "GiveWell’s support is enabling MDA in a total of 51 local government areas (LGAs) across the four states, including the following numbers in each state:
- Kebbi state: Schistosomiasis – 12 LGAs / STH - 0
- Kogi state: Schistosomiasis –13 LGAs / STH – 9 LGAs
- Kwara state: Schistosomiasis –11 LGAs / STH – 5 LGAs
- Sokoto state: Schistosomiasis –15 LGAs / STH – 3 LGAs"
Sightsavers, GiveWell Project Narrative, Nigeria Four States 2017, Pg 2.
- "In Sokoto state, one Local Government Area, Kebbe, has a prevalence of >50% for Schisto, as per WHO protocol, the Mass drug administration strategy in that LGA will include treating adults. The target is 75,631." Sightsavers, Responses to GiveWell questions, May 2017, Sheet "Nigeria 4 States Project," Cell C10.
- See map of Sokoto state indicating that Kebbe will be treated for both schistosomiasis and STH: Sightsavers, GiveWell Project Narrative, Nigeria Four States 2017, Pg 5.
- "GiveWell’s support is enabling MDA in a total of 51 local government areas (LGAs) across the four states, including the following numbers in each state:
- 45
- "In 2017 Sightsavers has received additional complementary funding from the Schistosomiasis Control Initiative (SCI) to support scaling up our deworming work in these four states to full capacity as well as supporting work in Jigawa state. SCI have recently (March 2017) provided Sightsavers with a grant of £398,898 to support activity until September 2017." Sightsavers, GiveWell Project Narrative, Nigeria Four States 2017, Pg 1.
- Number of SCI-supported LGAs derived from the maps presented at Sightsavers, GiveWell Project Narrative, Nigeria Four States 2017, Pgs 2-5.
- We note we do not know why Sightsavers applies GiveWell-directed funds to certain LGAs and SCI funds to others. We have not pursued this question as we think it is unlikely to affect our decision-making.
- 46
- "School aged children between 5-15 years in all schools and communities within the intervention zone are effectively treated with mebendazole/albendazole and praziquantel yearly. This will be integrated with onchocerciasis and Lymphatic Filariasis (LF) activities to provide 17.3 million treatments for onchocerciasis and LF in an integrated manner." Sightsavers, GiveWell Project Narrative, Benue State Nigeria 2017, Pg 1.
- Sightsavers set out how it integrates treatment in Benue state as follows: "In LGAs co-endemic with SCH, STH, onchocerciasis and LF, we aim to integrate CDD [community drug distributor] training, community sensitization and advocacy. If all necessary drugs arrive at the same time, we are also able to integrate drug distribution, taking into account an interval of two weeks for the distribution of the actual drugs (as required by the Standard Operating procedures for NTDs in Nigeria Sept 2015 – see document 6.1).
"For example, in an onchocerciasis, LF and SCH endemic community, CDD training, community sensitization and advocacy will happen together. Mectizan® and albendazole are then administered simultaneously, whilst praziquantel will be distributed two weeks later. We do not implement triple drug treatments even when other activities are integrated.
Although Benue MDA has not yet begun due to delays in the arrival of albendazole and praziquantel, the drug order has been approved and national drug deliveries are expected in September."Once the drugs arrive in state, the deworming programme will immediately begin. Training of CDDs and teachers to administer treatments is timed to coincide with the arrival of the drugs. It is beneficial for trainees to be able to start drug administration immediately after the training whilst it’s still fresh in their minds, rather than having a break between completing the training and beginning their work." Sightsavers, Country narrative report, Benue State Nigeria, Pgs 2-3.
- "Only school aged children will be targeted in Benue state as none of the LGAs qualitify [sic] for community MDA. However, a very small proportion of adults will be targeted within the schools - ie. teachers. Teachers are targeted after students are treated and there is balance of drugs." Sightsavers, Responses to GiveWell questions, May 2017, Sheet "Nigeria Benue State Project," Cell C10.
- For more detail on which diseases are treated in which local government areas in Benue state see the graphic on Sightsavers, GiveWell Project Narrative, Benue State Nigeria 2017, Pg 1.
- 47
- "In addition [to GiveWell-directed funding], for our wider NTD work within these integrated NTD programs, funds are made available from:
- Sightsavers unrestricted funds
- The UK Government's UKAID match - who are funding Sightsavers oncho and LF elimination program in four states (Kebbi, Kogi, Kwara and Sokoto states with a grant of £1,435,440 from April 2016 – March 2019
-Two state governments have pledged funding for NTDs activities, with details to be confirmed (Sokoto State and Kogi State)," Sightsavers, Responses to GiveWell questions, May 2017, Sheet "Nigeria 4 States Project," Cell C8. - "In addition [to GiveWell funding], funds are made available from:
- The UK Government's UKAID match - who are funding Sightsavers oncho and LF elimination program with a grant of £108,103 from April 2016 - March 2019.
- Sightsavers unrestricted funds." Sightsavers, Responses to GiveWell questions, May 2017, Sheet "Nigeria Benue State Project," Cell C8. - "Delivering this project will be cost effective as it is a part of NTDs programme which is already ongoing in all the beneficiary states." Sightsavers, GiveWell Project Narrative, Nigeria Four States 2017, Pg 16 and Sightsavers, GiveWell Project Narrative, Benue State Nigeria 2017, Pg 11.
- "In addition [to GiveWell-directed funding], for our wider NTD work within these integrated NTD programs, funds are made available from:
- 48
- Sightsavers used its unrestricted funding to support deworming in Kebbi, Kogi, Kwara and Sokoto states in 2015: see the charts in Sightsavers, Descriptions of current work - 2015 and 2016, Pgs 4 and 6.
- "The four projects Sightsavers submitted information on to GiveWell in May 2015, Kebbi state, Kogi state, Kwara state and Sokoto state, all took place as planned….Looking forward, 2016 budget expenditure for the onchocerciasis and LF elements of these four state programs is now expanded due to securing a new grant through the UKAID match program run by the UK government’s Department for International Development. This funding is for three years, 1 April 2016 – 30 March 2019, and will support the scale up of onchocerciasis and LF activities specifically in the four states." Sightsavers, Descriptions of current work - 2015 and 2016, Pgs 4-5.
- "We secured further new funding for the Sokoto State integrated NTD program from the Jersey Overseas Aid Commission, who will support the programme with a grant over three years from January 2016." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 6.
- 49
Commencing a project in Benue state was proposed to GiveWell by Sightsavers:
"2016 estimated costs featured in Sightsavers Phase 1 submission (to scale up in 4 states and begin work in Benue state at $415,973)." GiveWell, Analysis of Sightsavers deworming wishlist, 2016, Sheet "Deworming wishlist," Cell F14.
- 50
- "Sightsavers’ Nigeria country office is based in Kaduna with 35 staff, led by Country Director Sunday Isiyaku. Sightsavers also has a small annex office in the capital city of Abuja. The Government of Nigeria is responsible for program implementation in Sightsavers-supported state programs. Training on mass drug administration (MDA) is cascaded, with the Federal Ministry of Health supporting the training of the State NTD Teams, who in turn train the local government area (LGA) NTD teams. The LGA teams train the frontline health facility workers who train the community directed drug distributors. Supply of drugs flows through the same levels. Similarly, monitoring of MDA follows through the same channels and cascaded monitoring is undertaken. Reporting flows from the community level up to the federal level. NGO staff in all states provide technical support and conduct targeted monitoring and supportive supervision." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 3.
- "Sightsavers - Inputs to be provided:
- Advocacy to state and other stakeholders.
- Facilitate the distribution of NTDs control drugs to endemic communities working with the Federal Ministry of Health (FMOH).
- Procurement of NTDs control drugs for each state.
- Logistical support - donation of vehicles, equipment and instruments.
- Provide information, education and communication materials.
- Provide technical oversight on programme and financial activities for the programme.
- Undertake monitoring and supervision."
Sightsavers, GiveWell Project Narrative, Nigeria Four States 2017, Pg 3 and Sightsavers, GiveWell Project Narrative, Benue State Nigeria 2017, Pg 3.
- 51
"Sightsavers supports the national and state NTD teams for better program coordination at various levels. Support is also provided to the National NTD Steering Committee which provides a forum for discussing the overall strategic direction for the national NTD program. At the local government area level Sightsavers has facilitated the establishment of NTD Task Force committees which has improved ownership of the program." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 3.
- 52
"UNICEF is supporting sanitation and WASH activities in Benue State and Sightsavers is collaborating with them to promote WASH components of the deworming activities in the state." Sightsavers, Country narrative report, Benue State Nigeria, Pg 2.
- 53
"The Sightsavers led-UNITED programme (2013 – 2017) in Northern Nigeria aims to control NTDs in five states, Zamfara, Kaduna, Niger, Kano and Katsina. Fully funded by the UK Government, the project is treating blinding trachoma, schistosomiasis, lymphatic filariasis (LF), onchocerciasis and soil transmitted helminths (hookworm, whipworm and roundworm). Sightsavers leads the program and partners include CBM, Helen Keller International and MITOSATH." Sightsavers, Schistosomiasis (SCH) and STH program activity (non-GiveWell funded), 2016 and 2017, Pg 2.
- 54
"Sightsavers' broader NTD elimination projects in Guinea Bissau are funded through the following means:
- Trachoma elimination project - funded in 2017 through use of Sightsavers unrestricted funds.
- Oncho and LF elimination project - funded through the UK Government's UKAID match scheme - in all 11 regions with a grant of £840,000 from April 2016 - March 2019," Sightsavers, Responses to GiveWell questions, May 2017, Sheet "Guinea Bissau project," Cell C7. - 55
- "Country: Guinea Bissau … Duration: Two years, in the first instance, January 2017 – December 2018"
- "The support from Givewell will enable the Ministry of Health (MOH) NTD programme to scale up to support programming for schistosomiasis and STH; this will start with a reassessment of baseline endemicity levels and corresponding treatment plans. The surveys supported by Givewell will support all provinces with the exception of the Bijagos archipelago – wherein high resolution baseline mapping is being supported by the London School of Hygiene and Tropical Medicine"
Sightsavers, GiveWell Project Narrative, Guinea Bissau 2017, Pg 1.
- 56
"Sightsavers' broader NTD elimination projects in Guinea Bissau are funded through the following means:
- Trachoma elimination project - funded in 2017 through use of Sightsavers unrestricted funds.
- Oncho and LF elimination project - funded through the UK Government's UKAID match scheme - in all 11 regions with a grant of £840,000 from April 2016 - March 2019," Sightsavers, Responses to GiveWell questions, May 2017, Sheet "Guinea Bissau project," Cell C7. - 57
- "Treatments for school aged children in Guinea Bissau will be delivered through both school based treatment and community based treatment." Sightsavers, Responses to GiveWell questions, May 2017, Sheet "Guinea Bissau project" Cell C11.
- "Output 2 … Treat school aged children between 5-14 years for STH and for schistosomiasis through mass drug administration (MDA).
Activities: Collaborate with the NTD team of the Ministry of Health (MoH), Ministry of Education (MoE) and other partners to annually plan MDA, targeting both schools and communities." Sightsavers, GiveWell Project Narrative, Guinea Bissau 2017, Pg 3. - The figures titled "Map of program implementation areas Guinea Bissau 2017 and Guinea Bissau 2018" in Sightsavers, GiveWell Project Narrative, Guinea Bissau 2017, Pg 2 show that deworming work will occur in all districts of Guinea-Bissau, with treatments for STH occurring each year and treatments for schistosomiasis occurring every second year.
- 58
- "The study protocol and the mapping for SCH and STH will begin in October 2017 to align with schools re-opening after the summer break, followed by MDA, as required, in November/December 2017." Sightsavers, Country narrative report, Guinea Bissau, Pg. 1.
- "Ministry of Health - Inputs to be provided: Support the distribution of drugs from national to regional, districts, schools and community." Sightsavers, GiveWell Project Narrative, Guinea Bissau 2017, Pg 5.
- "Ministry of Education - Inputs to be provided: Provide teachers to support the MDA." Sightsavers, GiveWell Project Narrative, Guinea Bissau 2017, Pg 5.
- 59
- "Sightsavers - Inputs to be provided:
- Provide technical and financial support throughout the project cycle;
- Support in capacity building for partners, programme monitoring and quality assurance;
- Advocate for increased government ownership;
- Ensuring that donor requirements are met."
Sightsavers, GiveWell Project Narrative, Guinea Bissau 2017, Pg 5.
- "Output 1 Train health staff, community members and teachers to deliver schistosomiasis / STH MDA to schools and endemic communities. Activities … Train health workers at regional and district levels who will supervise the MDA campaign in the schools and communities; health workers have an important role to play in project implementation." Sightsavers, GiveWell Project Narrative, Guinea Bissau 2017, Pg 3.
We're not sure what activities, specifically, "quality assurance" refers to.
- "Sightsavers - Inputs to be provided:
- 60
- "Output 2 Treat school aged children between 5-14 years for STH and for schistosomiasis through mass drug administration (MDA). Activities … Collaborate with the NTD team of the Ministry of Health (MoH), Ministry of Education (MoE) and other partners to annually plan MDA, targeting both schools and communities." Sightsavers, GiveWell Project Narrative, Guinea Bissau 2017, Pg 3.
- "Sightsavers - Inputs to be provided:
- Provide technical and financial support throughout the project cycle;
- Support in capacity building for partners, programme monitoring and quality assurance;
- Advocate for increased government ownership;
- Ensuring that donor requirements are met."
Sightsavers, GiveWell Project Narrative, Guinea Bissau 2017, Pg 5.
- 61
"The support from Givewell will enable the Ministry of Health (MOH) NTD programme to scale up to support programming for schistosomiasis and STH; this will start with a reassessment of baseline endemicity levels and corresponding treatment plans. The surveys supported by Givewell will support all provinces with the exception of the Bijagos archipelago – wherein high resolution baseline mapping is being supported by the London School of Hygiene and Tropical Medicine. Sightsavers is in close communication with LSHTM about this mapping and as planned will support the MOH with any required interventions in this archipelago." Sightsavers, GiveWell Project Narrative, Guinea Bissau 2017, Pg 1.
- 62
- "However, due to the age of this data (baseline from 2004/5) and methodological limitations a new baseline study will now take place in 2017 (year 1 of the project) with funding from GiveWell." Sightsavers, Responses to GiveWell questions, May 2017, Sheet "Guinea Bissau project" Cell C11.
- "Given the planned surveys, Sightsavers expects a readjustment of treatment targets during 2017 for LF, oncho, schistosomiasis and STH." Sightsavers, GiveWell Project Narrative, Guinea Bissau 2017, Pg 1.
- 63
- "Sightsavers Cameroon has partnered with the Ministry of Public Health (MoH) since 1996, with our early work focused on the fight against onchocerciasis in Cameroon. This work comprised of a community-based onchocerciasis control project in Haute Sanaga Division, Centre Region." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 9.
- "Sightsavers has supported school based mass drug administration as part of integrated NTD programs in three regions of Cameroon since 2011, South-West, North West and West." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 8.
- 64
- "Sightsavers Cameroon has partnered with the Ministry of Public Health (MoH) since 1996, with our early work focused on the fight against onchocercisasis in Cameroon. This work comprised of a community-based onchocerciasis control project in Haute Sanaga Division, Centre Region. Following the advent of the African Programme for Onchocerciasis Control (APOC) and the Community Directed Treatment with Ivermectin (CDTI) strategy, Sightsavers expanded program activities to the South West and North West regions in 1998 and 2003 respectively. In 2003, in order to ensure that NGOs had a regional focus, the Haute Sanaga Project was ceded to Helen Keller International." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 9.
- "On an annual basis, a fixed obligation grant agreement is signed with Helen Keller International (USAID grantee) for implementation of regional program activities with USAID funds. Agreements are also signed with regional delegation teams to ensure fulfilment of annual obligations." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 9.
- "All projects in Cameroon are integrated schistosomiasis/STH programs. Most of the current funding is provided by USAID, and the key recipient is Helen Keller International (HKI). Sightsavers is one of the non-governmental organization (NGO) partners with which HKI works." GiveWell's non-verbatim summary of a conversation with Susan Walker and Katie Cotton, February 26, 2015, Pg 6.
- 65
- "Expected outputs: Establish baseline prevalence and intensity of SCH/STH in schools and communities."
- "Illustrative activities: Conduct a parasitological impact assessment survey in 15/16 health districts of the three supported regions."
- 66
- "The project has three key outcomes:
1) To complete sub-district level population-based SCH/STH prevalence surveys
2) To develop a Behaviour Change Communications (BCC) plan and evaluation strategy based on the use of environmental cues ('nudges') which engage unconscious decision-making processes to prompt behavior change (see recent research of Dreibelbis et al. 2015).
3) To train field actors (health professionals, community members) and teachers to undertake BCC activities in schools and communities where the prevalence of schistosomiasis or STH is determined to still be >50%* after five effective rounds of MDA (>75% coverage of school-aged children)." Sightsavers, Responses to GiveWell questions, May 2017, Sheet "Cameroon project," Cell C6. -
- "Objective 1: Complete population-based schistosomiasis / STH prevalence surveys in 15 districts in the three regions. ...
- Objective 2: Develop a behaviour change communication plan and evaluation strategy based on recent research by Dreibelbis et al. in the three supported regions. ...
- Objective 3: Train field actors (health professionals, community members and teachers) to undertake behaviour change communication activities in schools and communities. ...
- Objective 4: To improve hygiene and sanitation practices amongst school aged children (SAC) and parents in communities."
- "Based on the parasitological survey to be conducted in February 2018, the most SCH endemic health districts will be chosen to conduct SBCC activities related to SCH and STH. During this survey, sentinels sites will be established and will serve as reference points during impact assessment studies. A total of six health districts will be targeted by the project." Sightsavers, GiveWell Project Document Cameroon, Pg 8.
- "The six chosen health districts for this SBCC project (highlighted in red [in the table "Treatments to date in 2017") show high baseline prevalence; therefore, effective SBCC and WASH activities are likely to significantly reduce transmission of SCH and STH," Sightsavers, Country narrative report, Cameroon, Pg 1
- "The project has three key outcomes:
- 67
- "Sightsavers has supported NTDs in Guinea since 1993 through community directed treatment with ivermectin (CDTI) for onchocerciasis control, when it initiated a pilot project covering the sub-districts of Kègnèko, Saramoussaya and Ourékaba in the district of Mamou," Sightsavers, GiveWell Project Narrative, Guinea Conakry 2017, Pg 1.
- "In more recent years Sightsavers has extended its work in Guinea to support trachoma and LF elimination activities in 23 Health Districts (15 districts for trachoma and 8 districts for LF). This narrative project plan presents how Sightsavers support will now expand to support mass drug distribution for schistosomiasis and STH in districts with high prevalence, with the explicit intention of helping the Guinea government effect disease control." Sightsavers, GiveWell Project Narrative, Guinea Conakry 2017, Pg 1.
- 68
- "Sightsavers Deworming Programme - Guinea GiveWell Schistosomiasis / STH Project Narrative
Project Name: Guinea GiveWell schistosomiasis and STH project
Country: Guinea
Location: Districts of N’zérékouré, Lola and Yomou.
Duration: Two years, in the first instance, January 2017 – December 2018" Sightsavers, GiveWell Project Narrative, Guinea Conakry 2017, Pg 1. - "A gap exists in three health districts which have the highest prevalence in the country; N'Zérékoré, Lola and Yomou." Sightsavers, GiveWell Project Narrative, Guinea Conakry 2017, Pg 1.
- "Soil-transmitted helminthiasis (STH) and schistosomiasis are endemic in 17 and 31 health districts respectively, and co-endemic in a further 15. Mass Drug Administration (MDA) for both diseases is largely supported by Helen Keller International / ENVISION." Sightsavers, GiveWell Project Narrative, Guinea Conakry 2017, Pg 1.
- "In more recent years Sightsavers has extended its work in Guinea to support trachoma and LF elimination activities in 23 Health Districts (15 districts for trachoma and 8 districts for LF). This narrative project plan presents how Sightsavers support will now expand to support mass drug distribution for schistosomiasis and STH in districts with high prevalence, with the explicit intention of helping the Guinea government effect disease control." Sightsavers, GiveWell Project Narrative, Guinea Conakry 2017, Pg 1.
- "Sightsavers Deworming Programme - Guinea GiveWell Schistosomiasis / STH Project Narrative
- 69
- "Treatment in Guinea Conakry will be delivered through both school based treatment and community based treatment." Sightsavers, Responses to GiveWell questions, May 2017, Sheet "Guinea Conakry project," Cell C11.
- "Output 2 - Treat school aged children between 5-15 years for STH and for schistosomiasis through Mass Drug Administration (MDA)." Sightsavers, GiveWell Project Narrative, Guinea Conakry 2017, Pg 3.
- 70
"Sightsavers: Inputs to be provided:
- Provide technical, financial and human resources throughout the project cycle.
- Logistical support.
- Ensuring that donor requirements are met." Sightsavers, GiveWell Project Narrative, Guinea Conakry 2017, Pg 4.
- 71
"Advocacy for the programme was done at the national level to enable the integration of NTD MDA into one nationwide calendar, rather than having separate MDA schedules for each implementing partner. The Sightsavers team were able to influence the incorporation of the SCH and STH deworming project for the three districts into the national integrated plan." Sightsavers, Country narrative report, Guinea Conakry, Pg 1.
- 72
"Sightsavers has been supporting an onchocerciasis elimination project in the Democratic Republic of the Congo (DRC) since 2011, supporting the community directed distribution of Ivermectin (CDTI)." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 14.
- 73
"Our project operates in three areas of Lubutu Nord in Maniema province, Ituri Nord in Oriental province and Katanga Sud in Katanga province. Sightsavers provides support for this work through the United Front Against Riverblindness (UFAR) – a US-based non-profit organization established in 2004, which has been involved since 2006 in the control and elimination of onchocerciasis in DRC. Through established agreements Sightsavers has been providing support to UFAR to support the CDTI projects of Lubutu and Ituri Nord since 2011 and the CDTI project of Katanga Sud since 2013. All three projects are targeted for the elimination of onchocerciasis by 2025." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 14.
- 74
- "During 2015, we were additionally able to support 17,317 treatments for STH and schistosomiasis in the Ferekeni area of Lubutu, in partnership with Schistosomiasis Control Initiative (SCI). Sightsavers will support this mass drug administration for one final year in 2016." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 14.
- "Sightsavers has a strong relationship with SCI, and the two work closely together on many programs and sometimes in the same countries. One such country is DRC, where Sightsavers has no country office but provides support for an onchocerciasis partner, United Front Against Riverblindness. Sightsavers has facilitated SCI’s entry into the DRC and collaborates with SCI, providing financial coordination and technical support. Both organizations also have a presence in Côte d’Ivoire, where Sightsavers’ NTD adviser (who also covers Burkina Faso) works closely with SCI’s adviser. In both DRC and Côte d’Ivoire, the ministries of health usually hold an annual review and planning meetings, which Sightsavers will attend along with SCI. Sightsavers and SCI use this opportunity to discuss overall plans and budgeting for each country." GiveWell's non-verbatim summary of a conversation with Susan Walker and Katie Cotton, February 26, 2015, Pgs 7-8.
- 75
- "Sightsavers Deworming Programme – DRC GiveWell Schistosomiasis / STH Project Narrative … Location: Ituri Nord, Ituri Province … Duration of project: 2 Years, in the first instance, January 2017 – December 2018", Sightsavers, GiveWell Project Narrative, DRC 2017, Pg 1.
- "Within the Ituri Nord project area, support from Givewell in 2017 and 2018 is facilitating schistosomiasis / STH MDAs in all the health zones which reach the WHO-defined minimum thresholds for MDA; Schistosomiasis: Nyarambe (92.3%), Angumu (78.6%), Biringi (15.7%), Aru (12.7%), Mahagi (2.8%), Logo (0.8%); STH: Augnba (22.9%)", Sightsavers, GiveWell Project Narrative, DRC 2017, Pg 2.
- "Within the Ituri Nord project area, five of the eight health zones eligible for STH / schistosomiasis MDAs overlap with those in the oncho /LF elimination programme. As such, some support for deworming activities in these five health zones may be leveraged from the existing MDA program." Sightsavers, Responses to GiveWell questions, May 2017, Sheet "DRC Project," Cell C8.
- 76
- "Treatments in the DRC will be delivered through both school based treatment and door to door based treatment." Sightsavers, Responses to GiveWell questions, May 2017, Sheet "DRC Project," Cell C11.
- "School aged children between 5-15 years in all schools and communities within the intervention zone are effectively treated with mebendazole/albendazole and praziquantel yearly." Sightsavers, GiveWell Project Narrative, DRC 2017, Pg 2.
- 77
"A post-treatment coverage survey is planned for the end of December 2017, based on MDA taking place in late October/November," Sightsavers, Country narrative report, DRC, Pg 3.
- 78
"Stakeholder: Sightsavers / UFAR; Inputs to be provided:
- Advocacy to state and other stakeholders;
- Facilitate in collaboration with Ministry of Health, the distribution of NTD control drugs to endemic communities;
- Lead on procurement of NTD control drugs for the country;
- Logistical support, including donation of equipment and instruments;
- Provide information, education and communication materials to projects;
- Provide technical oversight on programme and financial activities for the programme;
- Undertake monitoring and supervision;
- Provide timely funds for field activity."
- 79
- 80
Julia Strong, International Foundations Executive, edits to GiveWell's review, November 9, 2016
- 81
- GiveWell's notes from its 2016 site visit to Ghana, Pg 1.
- "Sightsavers has a strong in-country presence in each of the countries we work in. Sightsavers has country offices in 24 countries led by experienced Country Directors and supported by teams of expert staff. Where we do not have an established country office, Sightsavers’ staff are embedded with the partner organization. Please see the map below detailing where we work." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 1.
- "We have 20 staffed offices in Africa (we have 24 program country offices including South Asia)." Julia Strong, International Foundations Executive, edits to GiveWell's review, November 9, 2016
- 82
Countries that don't have a country director based in-country include Guinea, Cote d'Ivoire, Guinea-Bissau, Burkina Faso, Togo, Benin, Niger, and DRC. GiveWell's notes from its 2016 site visit to Ghana
- 83
- GiveWell's notes from its 2016 site visit to Ghana
- For example, the project in the DRC that is supported by GiveWell-directed funds is implemented through Sightsavers' partner office, UFAR (United Front Against River Blindness). Sightsavers, Responses to GiveWell questions, May 2017, Sheet "DRC project", Cell C7 describes the staffing of UFAR's office and how its staff allocate time to the projects GiveWell-directed funds support.
- "Sightsavers has a strong in-country presence in each of the countries we work in. Sightsavers has country offices in 24 countries led by experienced Country Directors and supported by teams of expert staff. Where we do not have an established country office, Sightsavers’ staff are embedded with the partner organization. Please see the map below detailing where we work." Sightsavers, Descriptions of current work - 2015 and 2016, Pg 1.
- 84
- "Several of the country offices also have an M&E manager, who works with the NTD team but reports to the country director. Sightsavers also works closely with the NTD departments at the countries’ ministries of health and often has an NTD manager working inside the ministries’ offices." GiveWell's non-verbatim summary of a conversation with Susan Walker and Katie Cotton, February 26, 2015, Pg 6.
- Other M&E staff include:
- Monitoring and Evaluation Officers. For example, in 2017 Sightsavers hired dedicated Monitoring and Evaluation officers to support projects in Guinea-Bissau and Guinea Conakry. Sightsavers, Responses to GiveWell questions, May 2017, Sheet "Guinea Bissau project", Cell C7 and Sheet "Guinea Conakry project", Cell C7.
- Data Officers. For example, in 2017 a Data Officer in the Nigeria Country office was devoted (10% time) to "provid[ing] data management support to [Benue, Kebbi, Kogi, Kwara and Sokoto] states on data entry, analysis and cleaning of data to ensure its accuracy." Sightsavers, Responses to GiveWell questions, May 2017, Sheet "Benue state project", Cell C7.
- "We have promoted the idea of having NTD Managers in country (reporting to the country director/regional office) and a number of these positions are in place. We need to review if this structure has worked and also if capacity building/training is required in core areas of NTD work." Sightsavers, Now is the time to say goodbye to neglected tropical diseases, Pg 27.
- 85
The technical advisors also review Program Managers' reports and discuss any issues with the reports, and help analyze the data Sightsavers collects via monitoring. GiveWell's notes from its 2016 site visit to Ghana, Pg 2.
- 86
Julia Strong, International Foundations Executive, edits to GiveWell's draft 2017 review, November 14, 2017.
- 87
- 88
Partners are assessed for financial competence before projects are initiated and the frequency of reporting is agreed upon at that point – for most partners reporting is required either every month or on a quarterly basis. The finance team often visits partners with the program officers to help assess partners' work. Julia Strong, International Foundations Executive, edits to GiveWell's review, November 9, 2016
- 89
Sightsavers, Organizational expenditure 2014 and 2015 and Sightsavers, Finances 2016 actual and 2017 planned, Sheet "Organisational expenditure."
- 90
- "Gift in Kind: this figure is inclusive of the value of Mectizan tablets donated by Merck and Co. Inc towards Sightsavers onchocerciasis elimination programs" Sightsavers, Organizational expenditure 2014 and 2015. "Gift in Kind" is not defined in the 2015 and 2016 spending document. We assume it has the same meaning as in 2014 and 2015.
- Sightsavers, Data on in-kind drug donations
- "Donated costs from partners refers to the value of Mectizan® tablets donated by Merck & Co. Inc towards Sightsavers onchocerciasis elimination programs. Mectizan® is donated for a set number of countries and relates to the market value of the number of tablets required for shipment." Sightsavers, Response to document questions, October 5, 2016
- 91
Sightsavers, Organizational expenditure 2014 and 2015 and Sightsavers, Finances 2016 actual and 2017 planned, Sheet "Organisational expenditure." Also see our summary of Sightsavers' spending in the table below.
- 92
Sightsavers, Organizational expenditure 2014 and 2015, Sightsavers, NTD Project Expenditure, 2014-2016 and Sightsavers, Finances 2016 actual and 2017 planned, Sheet "Organisational expenditure."
- 93
See this spreadsheet for details.
- 94
See this spreadsheet for details.
- 95
See this spreadsheet, row 7.
Also see our summary of Sightsavers' spending in the table below (which shows spending in dollars rather than pounds).
- 96
Sightsavers, NTD Project Expenditure, 2014-2016 and Sightsavers, Finances 2016 actual and 2017 planned, Sheet "Organisational expenditure." See our spreadsheet for a breakdown in USD.
Note that the final figures for NTD spending in these documents do not include the indirect cost allocation that Sightsavers adds to all projects for its central costs. See note from Sightsavers: "Expenditure includes project values only and does not include the cost recovery or large programmatic core spend," Sightsavers, Finances 2016 actual and 2017 planned, Sheet "NTD Portfolio 2016-2017," Cell A87.
- 97
See our spreadsheet, Sheet "2014-2017 spending by NTD," Cell K112.
- 98
See this spreadsheet, Sheet "2017 deworming projects using GW influenced funds," Cell G16.
- 99
- See our spreadsheet, Sheet "Sightsavers budget for GW-influenced funds 2017".
- Our interim review sets out information Sightsavers shared with us about its projected spending for NTD programs in two countries (Nigeria and Guinea-Bissau) in 2015.
- 100
See this spreadsheet, Sheet "Total spending 2014-2016," Row 5.
- 101
Sightsavers staff, conversation with GiveWell, October 2, 2016
- 102
Sightsavers staff, conversation with GiveWell, October 2, 2016
- 103
- WHO, Helminth control in school-age children, Pg 74.
- This understanding comes from multiple conversations and documents.
- 104
- Details of the Kenya studies (Miguel and Kremer 2004, Baird et al. 2012) in our Reanalysis of the Miguel and Kremer deworming experiment page.
- Details of the Uganda study (Croke 2014) here.
- 105
Comment from Sightsavers provided in response to a draft of this page in November 2016.
- 106
We note that Sightsavers has advised it will provide the results by the end of 2017. Julia Strong, Sightsavers International Foundations Executive, edits to GiveWell's draft 2017 review, November 14, 2017.
- 107
- "Independent coverage assessments
"Sightsavers conducts independent assessments of treatment coverage in order to:- Estimate actual treatment coverage and compare this against reported treatment coverage (the official MOH statistics)
- Assess service delivery, or whether the treatment has been administered as recorded
- Investigate reasons for low coverage
"Methodology for independent assessments of treatment coverage
"To conduct these independent assessments on a community level, Sightsavers first calculates a statistically robust sample size, then randomly selects households for surveying within randomly selected villages. All members of each household are surveyed. Sightsavers aims to minimize recall re-bias (i.e. whether respondents forget what treatments they’ve received after a long period of time elapses) by undertaking assessments within 12 weeks of the distribution and showing the tablets to the household members who are being interviewed. The survey asks each respondent whether s/he has received treatment; if treatment has not been received the reason for this is recorded (e.g. ineligibility, concern over side effects, not offered, etc.)." GiveWell's non-verbatim summary of a conversation with Susan Walker and Katie Cotton, February 26, 2015, Pgs 2-3. - "Sightsavers hires external consultants to carry out coverage surveys. The process is managed by its policy and strategy department. The coverage surveys that GiveWell received are the first that were fully funded by Sightsavers; previous ones were funded by other organizations." GiveWell's notes from its 2016 site visit to Ghana, Pg 5.
- "Independent coverage assessments
- 108
- "Sightsavers’ selection criteria for Treatment coverage surveys: It will not be possible to conduct the survey after every round of MDA but if there is funding it is recommended a coverage survey is conducted:
- After the first round of MDA in an area
- If there are suspected issues with the health system or Community Health Worker (CHW) records or census data that need to be verified e.g poor population data, discrepancies between the drug store records/logs and the Community health Worker records or large variations in doses given year to year
- If the health system or Community Health Worker records show particularly low coverage e.g less than 60% or high coverage e.g 95 to over 100%
- If there have been issues in the area of operation with MDA coverage reporting in the past"
Julia Strong, International Foundations Executive, edits to GiveWell's review, November 9, 2016
- "Dr. Elhassan noted that Sightsavers has always followed a WHO protocol recommending that coverage surveys be conducted at a program's 1-, 3-, and 5-year marks." GiveWell's notes from its 2016 site visit to Ghana, Pg 6.
- "Sightsavers’ selection criteria for Treatment coverage surveys: It will not be possible to conduct the survey after every round of MDA but if there is funding it is recommended a coverage survey is conducted:
- 109
Sightsavers originally planned to conduct coverage surveys every 1-2 years and on our request plans to increase that to all MDAs (i.e., annually). In some cases, this will require additional GiveWell-directed funding in 2017-2018.
- See "Output Indicator 2.3: Number of treatment coverage surveys conducted with data disaggregated by age group and gender and school attendance" and cells E123-129, G123-129, Sightsavers, Deworming program consolidated logframe, September 2017 update, Sheet "Consolidated."
- "[GiveWell:] Would it be feasible to do coverage surveys in for MDAs in 2018 as well? None are currently scheduled. Approximately, how much would this cost (so we can add it to the wishlist)?
[Sightsavers:] Treatment coverage surveys have been partially budgeted for in Sightsavers’ new wishlist recently submitted to GiveWell, as such:- Guinea Conakry - TCS are included in our 2018 and 2019 wishlist budget requests
- Cameroon – TCS are included in our 2018 and 2019 wishlist budget requests
- DRC – TCS are included in our 2018 and 2019 wishlist budget requests
- Nigeria Bauchi State – TCS are included in our 2018 and 2019 wishlist budget requests
- Nigeria Yobe State - TCS are included in our 2018 and 2019 wishlist budget requests
However, we omitted to include TCS for each individual state in the Nigeria 4 States project, and also in the Benue state project. For these to be added into the programs in 2018, Sightsavers would wish to request the following additional funding added into our wishlist request. [...] Looking ahead, we would wish to add 2019 TCS budget requests for the same locations into a 2019 wishlist, should this become a possibility." Sightsavers, Responses to GiveWell questions, October 2017, Pg 2.
- 110
- Sightsavers, Coverage survey Benin and Togo 2015
- Sightsavers, Coverage survey Burkina Faso and Côte d'Ivoire 2015
- Sightsavers, Coverage survey Cameroon 2015-16
- Sightsavers, Coverage survey South Sudan 2015
- DFID-UNITED Integrated Post MDA Coverage Survey Report 2014
- DFID-UNITED Integrated Post MDA Coverage Survey Report 2015
- Sightsavers, Coverage survey Malawi 2015
- 111
"Three health districts received mass treatment in May 2017: N'Zérékoré, Lola and
Yomou. The coverage survey was conducted in the district of N'Zérékoré due to
constraints of time and logistics. The health district N'Zérékoré was chosen according to the following criteria:- It has the largest number of health centers (16 in total);
- Its strategic position in the region of the same name;
- All the villages in this district have a school;
- Its population is cosmopolitan, made up of people from other districts of the region (Gueckedou, Macenta, Beyla, Lola and Yomou)."
Sightsavers, Guinea Conakry Treatment coverage survey (English translation), Pg 4-5.
- 112
The report on the coverage surveys in Benin and Togo does not discuss how Abomey district was chosen in Benin or Sotouboua district in Togo (translated from French):
"On the basis of this manual, Sightsavers in collaboration with MURAZ Centre conducted an independent evaluation to assess the ivermectin treatment coverage and populations’ attitudes, knowledge and practices related to onchocerciasis CDTI projects in the health districts of Abomey (Benin) and Sotouboua (Togo). This independent evaluation also assessed the albendazole treatment coverage rate in Abomey district." Sightsavers, Coverage survey Benin and Togo 2015, Pg 12.
- 113
- The length of time between the MDA and the 2014 coverage survey in Nigeria was around 1 to 3 months: "The drug supplies were received in April 2014 and actual distribution of the drugs commenced in July 2014 in a staggered manner to avoid cross reaction between drugs. The last set of drugs that was distributed was in September; with Zithromax. Two weeks after the distribution of the last set of drugs, the Sightsavers International-lead partner of the UNITED consortium in collaboration with Zamfara State Ministry of Health initiated conducted a post MDA coverage survey principally to validate the reported coverage. This activity which took place from 15 th to 30th October 2014 was sponsored by the UNITED consortium." DFID-UNITED Integrated Post MDA Coverage Survey Report 2014, Pg 4.
- The report of the 2015-16 survey in Cameroon does not state when the MDA program occurred: "Technical preparation, data collection / analysis and report writing were carried out from December 10th 2015 to January 31th, 2016 ) according to the chronogram." Sightsavers, Coverage survey Cameroon 2015-16, Pg 11.
- Full details on the length of time between the MDA and the coverage survey for all Sightsavers' coverage surveys that are publicly available can be found in this spreadsheet, Sheet "Methods."
- 114
"For context, ideally we look to do within 1-2 months after the distribution. The anomaly was in Nigeria where we decided to do an integrated treatment coverage survey which took into account multiple MDAs for different drugs over a wider timeframe, this is the exception rather than the norm for programs.
Recall bias could be an issue but research into the recall bias of MDA has suggested that it is not as big an issue as feared and actually even 1 year after the MDA can give valid and relevant results.
Budge et al (2016) PLOS NTD https://www.ncbi.nlm.nih.gov/pubmed/26766287"
Julia Strong, International Foundations Executive, edits to GiveWell's review, November 9, 2016 - 115
- Details on data quality control processes for all Sightsavers' coverage surveys we have seen are available in this spreadsheet, Sheet "Methods."
- Sightsavers told us about some informal verification processes it uses:
- "Supervisors monitor the data that surveyors are collecting. For example, in a survey that took place in Cote d'Ivoire and Burkina Faso, there were six teams of three surveyors. Four supervisors (two teams of two supervisors) accompanied surveyors on their visits to listen to their interviews and check their forms to be sure they had been correctly filled in. If there were mistakes, these were corrected on the spot so that surveyors could improve as the day went on." GiveWell's notes from its 2016 site visit to Ghana, Pg 6.
- "For context, we ensure supervisors work closely with teams when collecting data to ensure they are following protocol, check questionnaires at the end of the day for data quality and completeness and also have regular team and feedback meetings. We are now using electronic data capture which allows for basic consistency checks during data collection and also tracks the GPS location of the teams so we can provide some additional external support supervision of the teams." Julia Strong, International Foundations Executive, edits to GiveWell's review, November 9, 2016
- 116
- DFID-UNITED Integrated Post MDA Coverage Survey Report 2014 The report's summary states that praziquantel (PZQ) coverage rates were 46% in Bungudu and 54% in Shinkafi, the two LGAs studied (Pg 4). The data table later in the report shows PZQ coverage rates were 68% in total, 55% in Bungudu and 88% in Shinkafi (Pg 21). The report mentions that some PZQ treatment was delayed partly due to the MDA timing conflicting with Ramadan and schools shutting down due to the Ebola outbreak, and some PZQ treatment was still ongoing at the time of the coverage survey (Pg 27). It is possible that the larger numbers include mop-up treatment that was done due to low initial coverage (Pg 28).
- We have found the report on the 2015 coverage survey in Malawi to be difficult to interpret due to several inconsistencies. Sightsavers, Coverage survey Malawi 2015:
- It is not clear whether the survey took place in 8 districts or 9 districts:
- "Coverage surveys were conducted between November and December 2015 in 9 of the 13 districts (Nsanje, Zomba, Machinga, Mwanza, Neno, Ntcheu, Lilongwe East, Dowa and Ntchisi) that implemented MDA in 2015." Pg 1.
- "The survey that was conducted using the standard 30 by 7 methodology for coverage surveys, and the compact segment sampling. 30 clusters (villages) were sampled randomly in each of the 8 districts." Pg 2.
- The report states that surveys were not conducted in Lilongwe West, but also reports survey coverage for Lilongwe West:
- "Surveys were not conducted in Kasungu, Nkhotakota, Salima and Lilongwe West." Pg 1.
- "Coverage by survey - before mop-up" reported as 83.9% for Lilongwe West in Table 3, Pg 5.
- Coverage rates from the survey by district are reported in Table 2 on Pg 4 and Table 3 on Pg 5. Both tables report the same survey coverage rates for Nsanje, Mwanza, Neno, Ntchisi, and Lilongwe West districts, but survey coverage rates differ between the two tables for Ntcheu, Machinga, Dowa, and Zomba districts.
- Our best guess is that some of the data in the rows in one of the tables may have been reshuffled, but we are uncertain which of the two tables is correct.
- It is not clear whether the survey took place in 8 districts or 9 districts:
- 117
"The surveyed data for Praziquantel could not be compared health system records because treatment was still on-going in most communities and the records for the health system were not complete." DFID-UNITED Integrated Post MDA Coverage Survey Report 2014, Pg 5.
- 118
For the results of these coverage surveys, see this spreadsheet, "Results" sheet.
- 119
"The results of this survey showed that coverage of MDA was 57.58% (95% CI: 46.91 to 67.60) overall. … In our survey, considering the main target of treatment, which are the children in the schools, the results of the survey showed that 69.9% (95% CI: 58.0 to 80.0) of children enrolled were treated." Sightsavers, Guinea Conakry Treatment coverage survey (English translation), Pg 3.
- 120
For example, Sightsavers shared some sample coverage survey results with us and we have not seen reports from some of those surveys. Sightsavers, Coverage surveys presentation, August 2016, Pg 5.
- 121
Translated from French: "Among the population that did not take ivermectin during the last treatment campaign, the primary reason was community distributors not going to their homes and village, particularly in the health district of Abomey (67.8%)." Sightsavers, Coverage survey Benin and Togo 2015, Pg 28.
- 122
- "The combined analysis of Tables 2 and 3 enables us to say that the distribution strategy of drugs in schools was more favored by distributors than the distribution in the community. Since the distribution took place in schools, many children were treated at school even those who did not attend school because distributors asked out-of-school children to go to school to receive their treatment. Another aspect that could explain the low overall coverage rate is that the survey was conducted during the school holidays. Children that were treated for MDA would already be on vacation outside N'Zérékoré at the time of the survey, and it was also the end of the Ramadan period." Sightsavers, Guinea Conakry Treatment coverage survey (English translation), Pg 9.
- We spoke with Sightsavers about how timing the coverage survey during the holiday period would affect the coverage rate that the survey estimates during our visit to Guinea in October 2017. Notes from a site visit to Sightsavers in Conakry, Guinea in October 2017, Pg 2.
- 123
- 124
Tekle et al. 2012, Pg 1.
- "Methods: In 2008, an epidemiological evaluation using skin snip parasitological diagnostic method was carried out in two onchocerciasis foci, in Birnin Gwari Local Government Area (LGA), and in the Kauru and Lere LGAs of Kaduna State, Nigeria. The survey was undertaken in 26 villages and examined 3,703 people above the age of one year. The result was compared with the baseline survey undertaken in 1987."
- "Results: The communities had received 15 to 17 years of ivermectin treatment with more than 75% reported coverage. For each surveyed community, comparable baseline data were available. Before treatment, the community prevalence of O. volvulus microfilaria in the skin ranged from 23.1% to 84.9%, with a median prevalence of 52.0%. After 15 to 17 years of treatment, the prevalence had fallen to 0% in all communities and all 3,703 examined individuals were skin snip negative."
- 125
- The report does not appear to address confounding factors that could have also impacted prevalence. The treatment was carried out over a long time period: treatments began in 1991, the Community Directed Treatment with Ivermectin was introduced in 1997 (and Sightsavers became involved), and treatment continued for 15-17 years through 2008 (when this survey was conducted) (pg. 2). Given this, it seems possible that other improvements (e.g. in economic and/or health systems or environment) could have played a role in the observed decline in infection.
- The surveyed communities were selected partially because they had the longest treatment periods and high coverage rates: "The two foci were selected for the following reasons: i) communities in these foci had pre-control epidemiological data; among the areas where large-scale ivermectin treatment was first introduced in Africa were these two foci in Kaduna in which treatment of a sample of the population started as part of a randomised controlled trial of ivermectin in 1988 and 1989, and where skin-snip surveys had been done in preparation for the trial [6,17]. ii) the foci included hyper-endemic villages, i.e. villages with a prevalence of microfilaridermia > 60% [15-17]; iii) the area was located along a river with known breeding sites of Simulium damnosum s.l., iv) the communities had had 15 - 17 years of annual treatment with ivermectin using the community-based programme since 1991, and subsequently through the community-directed treatment with ivermectin (CDTI) strategy from 1997 with more than 65% treatment coverage." Pg 3.
- "A limitation of the epidemiological surveys is that a third of the population in the selected communities did not participate in the skin-snip examination. Though some of these had valid reasons for non-participation (age < 1 year, illness, absence from the village etc), for a large majority the reasons for non-participation were not known. This high non-participation rate could have created a bias in the survey results if those who did not participate in the survey were also more likely not to have participated in ivermectin treatment." Pg 8.
- The study does not discuss the methods of the baseline survey.
- 126
Lakwo et al. 2015
- 127
“Results: […] The prevalence of onchocerciasis ranged from 0.8% to 5.5% while the CMFL ranged from 0.01 to 0.11 mf/ss.” Lakwo et al. 2015, Pg 3.
- 128
"One of the shortcomings is inadequate mf [microfilariae] prevalence data in this focus. Baseline data on mf prevalence is only available for Nyakabale and Kyeramya villages Hoima district which was collected in 2007. This information is very vital for decision making within the framework of elimination." Lakwo et al. 2015, Pg 4.
- 129
Lakwo et al. 2015, Pg 3.
- "Conclusion: The performance of mass treatment in Budongo focus has been good since out of the 15 villages assessed only three of them have mf prevalence >5% and CMFL far below the threshold of >5 mf/s."
- "Results: A total of 2,728 people were examined, composing of 55% (1494/2728) females and 45% (1231/2728) males. The overall mf [microfilariae] prevalence was 2.6% (73/2728) and CMFL [Community Microfilaria Load] was 0.04 mf/s and varied significantly in the communities (p <0.05). The prevalence of onchocerciasis ranged from 0.8% to 5.5% while the CMFL ranged from 0.01 to 0.11 mf/ss [microfilariae per skin snip]. Infection was recorded more among the males (3.7%) compared to the females (1.7%). Mf prevalence was recorded highest in Masindi district (5.5%) and lowest in Hoima district (0.8%). The CMFL recorded was far <5 microfilariae per skin snip, i.e. recognized by WHO as threshold value in certifying the communities to be free of onchocerciasis as public health problem, thus, signifying the possibility of onchocerciasis elimination in the focus." See also discussion of results on Pgs 15-17.
- 130
A few observations from Lakwo et al. 2015:
- "Methods: Villages were selected in each of the districts following APOC procedures. Mobilizations were conducted by use of local authorities in each respective village. Questionnaires were administered among those who participated in the study. Skin snip was conducted in the selected communities (n=15) in Hoima, Buliisa and Masindi districts. Microfilaria prevalence and CMFL were calculated for each village," Pg 3. Participation in the prevalence study appears to have been opt-in and nonrandom. "Those eligible from 5 years and above from household were invited to participate in the survey. Participants were recruited consecutively from families until the required sample size was achieved," Pg 6. Participation rate or representativeness of the sample are not discussed apart from listing "Low turn up of participants in some of the villages in some districts" as a challenge, Pg 17.
- The report does not appear to address confounding factors that could have impacted prevalence. The treatment was carried out over a long time period: treatment started in 1993, the Community Directed Treatment with Ivermectin was introduced in 1999, and an elimination policy was launched in 2007, with treatment presumably ongoing. “Mass treatment with ivermectin started in the 1993 with support from Sightsavers International. In 1999, the Community Directed Treatment with Ivermectin (CDTI) strategy was introduced to ensure sustainability of the program. When elimination policy was launched in 2007, bi-annual treatment and vector elimination strategies were adopted to enhance elimination,” Pg 3. Given this, it seems possible that other improvements (e.g. in economic and/or health systems, or the environment) could have played a role in the reported improvements.
- 131
- 132
- "The Guinea-Bissau Programa Nacional de Saude Visuel(PNSV) , with support from Sightsavers International has conducted three rounds of azithromycin distribution between 2009-2012 -in the regions of Oio, Bafata and Farim(formerly part of Oio)." Bailey 2013, Pg 1.
- "Sightsavers’ Guinea Bissau trachoma elimination program has run since 2011 and is working to ensure Guinea Bissau can be declared free of blinding trachoma by 2020. The project is supporting the implementation of the full SAFE strategy for trachoma elimination (Surgery to treat trichiasis, Antibiotics to treat infection, Facial cleanliness and Environmental improvement to interrupt disease transmission). Project activities include the distribution of the antibiotic treatment Zithromax, the training of trichiasis (TT) surgeons and the provision of TT surgeries, and the improvement of environmental sanitation in target areas through the construction of water points and latrines, alongside behaviour change activities to ensure their use.” Sightsavers, Guinea-Bissau NTD program information prepared for GiveWell, May 2015, Pg 2.
- "Sightsavers is the key Ministry of Health partner for trachoma elimination activities in Guinea Bissau and is supporting the distribution of the antibiotic treatment Zithromax, the training of trichiasis (TT) surgeons and the provision of TT surgeries, and the improvement of environmental sanitation in target areas through the construction of water points and latrines, alongside behaviour change activities to ensure their use. The prevalence of trachoma in Guinea Bissau ranges between 10%-39.9%. (see Map 1)We are supporting the MoH to meet the WHO recommended target of reducing the prevalence of active trachoma (TF) to less than 5% among children aged 1-9 years, to reduce the prevalence of TT to less than 1 case per 1000 population above 15 years old, and to maintain (TT) recurrence to below 10%. The implementation of the SAFE strategy has resulted in the reduction of prevalence as shown in Table 2. Other NGO partners involved in implementing the SAFE strategy for trachoma elimination in Guinea Bissau include The International Trachoma Initiative (supporting Zithromax distribution). Sightsavers plans to support the writing of a trachoma Action Plan for Guinea Bissau in October 2015, in partnership with the International Trachoma Initiative and the London School of Hygiene and Tropical Medicine." Sightsavers, Guinea-Bissau NTD program information prepared for GiveWell, May 2015, Pg 4.
- 133
- “Following three rounds of MDA the estimated prevalence of TF in 1-9 year olds is below the 5% threshold in Oio, Bafata and Farim: 2.9% in Oio, 1.4% in Bafata and 4.2% in Farim. There seems to be no need for further distribution in these regions.” Bailey 2013, Pg 3.
- Methodology is discussed in Bailey 2013, Pgs 1-2, including that households absent at the time of the survey were excluded rather than revisited at a later time: "In the event that the 15 households did not contain 50 children, or that the selected households were unavailable reserves were used until 50 children had been examined," Pg 1. Diagnosis and grading of trachoma was performed by "ophthalmic nurses and cataract surgeons from the PNSV who had received training in the grading of trachoma according to the WHO simplified system, and had received training in the field in the study procedures," Pg 2.
- 134
In Sightsavers, Guinea-Bissau NTD program information prepared for GiveWell, May 2015, Pg 4, Sightsavers sent us a table of trachoma (TF) and trichiasis (TT) prevalence rates in 2005 compared to prevalence found in the 2013 impact study. 2005 data is available for eleven regions, including the three regions targeted by the 2013 study. We have not seen the methodology for the 2005 prevalence survey and we are unsure whether it is appropriately comparable to the 2013 survey.
Region Trachoma prevalence (2005) Trachoma prevalence (2013) Bafata 28.7% 1.38% Oio 21.7% 2.94% Farim 21.7% 4.21% - 135
- 136
Sightsavers told us that "Sightsavers follows recommended WHO guidelines with regard to the establishment of sentinel sites. For deworming programs sentinel sites are typically established at schools. Impact indicators track change in prevalence and intensity of infection (intensity is recognized as a more sensitive indicator of impact)." GiveWell's non-verbatim summary of a conversation with Susan Walker and Katie Cotton, February 26, 2015, Pg 2. It is possible that impact assessments conducted at sentinel sites (where programs may be higher quality) may not be representative of impact at other sites. Of the three impact assessments discussed above, the first (Tekle et al. 2012) explicitly selected sentinel sites for assessment. We are unsure whether the other two impact assessments took place at sentinel sites.
- 137
We note that Sightsavers has advised that it will provide the results by the end of 2017. Julia Strong, International Foundations Executive, edits to GiveWell's draft 2017 review, November 14, 2017.
- 138
"In all MDAs, supervisors should conduct routine monitoring of the work of community CDDs by using checklists for each monitoring level (for example, local and national) and produce reports for the implementation areas. Sightsavers told us that it could share these reports, which differ from those generated through Sightsavers' newly developed quality standard assessment tool (QSAT)." GiveWell's notes from its 2016 site visit to Ghana, pg. 7.
- 139
- 140
- 141
"CDDs were observed conducting census updates using the treatment register and conducting treatment. Health workers and LGA teams also conducted supervision using the supervision plan developed at the LGA level. The NTD checklist was used for supervision by the independent monitors. The supervisory checklist was uploaded into an android phone and information collected was uploaded to a cloud server.
The following activities were supervised:
i. Presence of CDDs.
ii. Correct register data entry
iii. Appropriate use of dose pole.
iv. Drug availability and sufficiency.
v. Presence of water sources in the community
vi. Presence of adverse effects" Sightsavers, Kebbi monitoring trip report 2016, Pg 2. - 142
- Sightsavers' templates suggest that monitoring reports are produced quarterly and annually, but we are uncertain if reports are produced with this frequency in practice.
- Sightsavers, Quarterly monitoring report template
- Sightsavers, Annual project report template
- 143
"In all MDAs, supervisors should conduct routine monitoring of the work of community CDDs by using checklists for each monitoring level (for example, local and national) and produce reports for the implementation areas. Sightsavers told us that it could share these reports, which differ from those generated through Sightsavers' newly developed quality standard assessment tool (QSAT)." GiveWell's notes from its 2016 site visit to Ghana, Pg 7.
- 144
"Sightsavers QSAT does not replace routine monitoring, it is additional to it. The action plans developed after a QSAT assessment are typically followed up in routine monitoring visits following the QSAT. QSATs can be undertaken to inform project design at baseline, during the course of project implementation or at the end of a project." Julia Strong, International Foundations Executive, edits to GiveWell's review, November 9, 2016
- 145
- Our intervention report discusses this briefly.
- Other conversations and observations have reinforced our impression that administering deworming drugs is fairly straightforward.
- The WHO factsheet on STH: "The recommended medicines – albendazole (400 mg) and mebendazole (500 mg) – are effective, inexpensive and easy to administer by non-medical personnel (e.g. teachers)." WHO STH factsheet
- 146
- "In Tanzania matters came to a head in places around Morogoro in 2008. Distribution in schools of tablets for schistosomiasis and soil-transmitted helminths provoked riots, which had to be contained by armed police. It became a significant national incident, and one of the consequences has been the delay in Tanzania adopting a fully integrated NTD programme, and the scaling back some existing drug distributions." Allen and Parker 2011, Pg 109.
- "From these reports a number of problems with the MDA were raised which included fear of side effects from the tablets, particularly following the mass hysteria and death in Blantyre and Rumphi respectively and may explain some of the geographic heterogeneity seen. Furthermore most districts reported that MDA occurred after standard 8 students had finished exams and left school, and due to having inadequate resources for drug distribution...The side-effects incident in Blantyre and death in Rumphi had a large effect on districts and with many district reports stating that after the incidence many families refused to participate." SCI Malawi coverage survey 2012 Pgs 5 and 21.
- 147
"There was confusion on Wednesday in some public primary and secondary schools in Ogun State, over the administration of anti-worm tablets. Nigerian Tribune gathered that some students reportedly collapsed in the cause of administering the tablets on them. This resulted into rumour that spread like wildfire across the length and breadth of the state, as parents stormed various school to withdraw their wards. When the Nigerian Tribune visited Egba High School, Asero and Asero High School both in Abeokuta South Local Government Area of the state, some parents were sighted at the school gate, who had come to confirm the incident and probably withdraw their wards. There was calmness in both schools as students in the Senior Secondary Classes were said to be preparing for their examinations. Meanwhile, the Ogun State Government through the State Commissioner for Health, Dr Babatunde Ipaye, has denied any case as a result of the anti-worm drug. Ipaye in a statement made available to the Nigerian Tribune in Abeokuta, said that no pupil or student to the best of his knowledge had reacted to the drug in the state. He explained that the exercise was done by his Ministry in collaboration with Evidence Action." Nigerian Tribune, "Panic in Ogun schools over deworm exercise," December 2017
- 148
- 149
The study assumes that government staff costs account for approximately 30% of the program's expenses. See our review of SCI for more information.
- 150
For example, if Sightsavers reports treating 100 children in Country X with albendazole and 90 children in Country X with praziquantel, we assume the populations fully overlap, so Sightsavers has treated 100 children (90 children with albendazole + praziquantel and 10 children with just albendazole).
- 151
For an example of Sightsavers' budget categories, see this spreadsheet, "Sightsavers budget for GW-influenced funds" tab, column A.
- 152
See this spreadsheet for more detail.
- 153
See this spreadsheet for more detail.
- 154
See this spreadsheet, "Spending opportunities" tab, cells D56 and D57.
- 155
See this spreadsheet, "Spending opportunities" tab, cell D58.
- 156
See this spreadsheet, "Available and expected funding" tab, row 18.
- 157
See this spreadsheet, "Available and expected funding" tab, row 28.
- 158
See our interim review of Sightsavers.
- 159
- "As previously submitted during Sightsavers’ Phase 1 submission to GiveWell, Nigeria represents a country where Sightsavers is keen to expand its operations to increase schisto and STH integrated control. Whilst we have secured new funding to expand our oncho and LF elimination work in Nigeria over the past year (detailed in document 16.1), the situation as regards how we would like to expand STH and schisto activities remains similar to our submission to GiveWell in May 2015. We have incorporated summary information from our 2015 submission in the table." Sightsavers, Deworming wishlist notes, 2016, Pgs 1-2.
- "As previously presented in Sightsavers’ Phase 1 submission to GiveWell, Guinea-Bissau represents a country where Sightsavers is keen to expand its operations to include schistosomiasis (schisto) and soil-transmitted helminths (STH) integrated control. While we have secured new funding from UK Aid Match to expand our oncho and LF elimination work in Guinea Bissau between 2016-19, the situation as regards how we would like to expand STH and schisto activities remains similar to our submission to GiveWell in May 2015." Sightsavers, Deworming wishlist notes, 2016, Pg 1.
- 160
Sightsavers staff, conversation with GiveWell, October 2, 2016
- 161
- "USAID has informed partners that the FY18 budget for Cameroon will not include support for SCH/STH MDAs previously supported. However, USAID will provide limited support for SCH/STH impact surveys in 10-12 selected areas. While USAID has been clear that they are committed to supporting NTD control and elimination efforts in Cameroon, any funding support for SCH/STH MDAs will need to be supported by the government or other funding partners starting in 2018. While the emphasis on conducting impact assessments in 2018 will be helpful in developing new treatment strategies, the fact remains that the West, North West, and South West Regions, will not have any funding from USAID for SCH/STH MDA in 2018. This support has been requested as part of Sightsaver’s GiveWell wish-list submission."
Julia Strong, Sightsavers International Foundations Executive, edits to GiveWell's draft 2017 review, November 14, 2017. - "During the 2018 ENVISION planning session in Cameroon, it was announced that the ENVISION programme will end in 2019 with a significant reduction of the budget in 2018. ... the Cameroon wish list provides for support in the three regions currently supported by Sightsavers, for:
- All deworming MDAs (2018)
- All STH, SCH, onchocerciasis and LF MDAs (2019)
- The expansion / strengthening of PZQ access to adults and non- enrolled school age children (SAC) (both 2018 and 2019)" Sightsavers, Deworming wishlist, Cameroon 2018-19, explanatory narrative, pg. 1
- "USAID has informed partners that the FY18 budget for Cameroon will not include support for SCH/STH MDAs previously supported. However, USAID will provide limited support for SCH/STH impact surveys in 10-12 selected areas. While USAID has been clear that they are committed to supporting NTD control and elimination efforts in Cameroon, any funding support for SCH/STH MDAs will need to be supported by the government or other funding partners starting in 2018. While the emphasis on conducting impact assessments in 2018 will be helpful in developing new treatment strategies, the fact remains that the West, North West, and South West Regions, will not have any funding from USAID for SCH/STH MDA in 2018. This support has been requested as part of Sightsaver’s GiveWell wish-list submission."
- 162
"In 2017 the UK Government Department for International Development announced a doubling of its support to fight neglected tropical diseases over the next 5 years.This will support programme implementation and research, further information is available online: https://www.gov.uk/government/news/uk-to-protect-200-million-people-fro…." Sightsavers, Other Funding Opportunities (2017; unpublished source)
- 163
Conversation with the Schistosomiasis Control Initiative, October 2017.
- 164
Sightsavers, Other Funding Opportunities (2017; unpublished source)
- 165
Mike Straney, conversation with GiveWell, October 10, 2017
- 166
Internal donation records
- 167
Sightsavers is also seeking funding for water, sanitation and hygiene (WASH) work in Guinea. We have excluded this item from the list of spending opportunities because we believe it is outside the scope of our review.
- 168
Sightsavers, Deworming wishlist 2018 and 2019
- 169
For details, see Sightsavers, Deworming wishlist, DRC 2018-19, explanatory narrative and Sightsavers, DRC Annex 1.
- 170
For details, see Sightsavers, Deworming wishlist, Guinea Conakry 2018-19, explanatory narrative, Sightsavers, Guinea Conakry WASH wishlist activities, Sightsavers, Guinea Conakry Annex 1, and Sightsavers, Guinea Conakry Annex 2.
- 171
For details, see Sightsavers, Nigeria Four states and Benue state projects wishlist narrative and Sightsavers, Amendments to original documents for Nigeria four states and Benue state projects.
- 172
- For details, see Sightsavers, Deworming wishlist, Yobe State, Nigeria 2018-19, explanatory narrative.
- "[GiveWell:] In Yobe state, WHO strategy says to treat 10 LGAs every other year and 7 twice during primary school. Sightsavers is proposing to treat the 10 LGAs in each 2018 and 2019. Why diverge from WHO recommendations here?
[Sightsavers:] [...] Sightsavers’ Nigeria team are aware of WHO recommendations, however, we take the lead from the FMOH, who have found that in practice disease prevalence in the state is increasing in project areas, hence treatment being planned for both consecutive years." Sightsavers, Responses to GiveWell questions, October 2017, Pg 4.
- 173
For details, see Sightsavers, Deworming wishlist, Guinea Conakry 2018-19, explanatory narrative, Sightsavers, Guinea Conakry WASH wishlist activities, Sightsavers, Guinea Conakry Annex 1, and Sightsavers, Guinea Conakry Annex 2.
- 174
For details, see Sightsavers, Nigeria Four states and Benue state projects wishlist narrative and Sightsavers, Amendments to original documents for Nigeria four states and Benue state projects.
- 175
For details, see Sightsavers, Deworming wishlist, Bauchi State, Nigeria 2018-19, explanatory narrative.
- 176
For details, see Sightsavers, Deworming wishlist, DRC 2018-19, explanatory narrative and Sightsavers, DRC Annex 1.
- 177
"[GiveWell:] What do you think the probability is that USAID funds the work in Cameroon? Why did they end the ENVISION program?
[Sightsavers:] The ENVISION project has not yet ended, and will continue in 2018 and 2019. USAID will continue to fund work in Cameroon, however this is more likely to focus on funding for LF, onchocerciasis and trachoma (including beyond 2019), with a possible reduction in funding for STH and schisto, hence Sightsavers’ request to GiveWell. There is still a chance that they will be supporting a certain number of surveillance surveys for SCH/STH, but the location of those surveys has not yet been determined." Sightsavers, Responses to GiveWell questions, October 2017, Pg 3. - 178
- For details, see Sightsavers, Deworming wishlist, Cameroon 2018-19, explanatory narrative and Sightsavers, Cameroon Annex 1.
- "The NTD MOU between Sightsavers and the Cameroon government is a general overarching framework agreement between the MoH and all the NGDOs [non-governmental development organizations] working within the NTDs programme. As such it does not legally bind us to any specific support level given the generic nature of framework agreements. However, Sightsavers is committed to contribute funds towards currently supported activities and indeed there are expectations from the government since we are the main NGDO partner for the South West, West and North West regions. This has been the case over the years and we have been contributing funds towards the Schisto/STH deworming campaigns even with USAID funding. As such, Sightsavers is committed to making all efforts to leverage the appropriate level of funding for [...]:
- Deworming MDAs (2018)
- STH, SCH, onchocerciasis and LF MDAs (2019)
- The expansion / strengthening of PZQ access to adults and non-enrolled school age children (SAC) (both 2018 and 2019)
It can be challenging to raise unrestricted funds and if GiveWell are able to commit funding support for all or part of this work in Cameroon it would make a significant difference to the program." Sightsavers, Responses to GiveWell questions, October 2017, Pg 3.
- 179
Due to rounding, the above values do not add up to exactly $6.5 million. For more detail, see this spreadsheet.
- 180
See this spreadsheet.
- 181
- Sightsavers staff, conversation with GiveWell, October 2, 2016
- Sightsavers lists projects in which it supports deworming in Sightsavers, Schistosomiasis (SCH) and STH program activity (non-GiveWell funded), 2016 and 2017. Sightsavers may be using unrestricted funds to support the integrated NTD program in Sierra Leone which include schistosomiasis and STH. Sightsavers also contributes 10% of the budget in Cameroon from unrestricted funding, as a condition of its grant for that program (see Sightsavers, Deworming wishlist, Cameroon 2018-19, explanatory narrative).
- 182
WHO, Summary of global update on preventive chemotherapy implementation in 2016, Pg 590, Table 1.
WHO, Summary of global update on preventive chemotherapy implementation in 2015, Pg 456, Table 1.
WHO Weekly epidemiological record, 18 December 2015, Pg 707, Table 1.