This page is part of our report on The Carter Center.
Published: 2009
Table of Contents
What do they do?
The Carter Center Schistosomiasis Control Program is part of its integrated program in two states in Nigeria; the integrated program simultaneously combats schistosomiasis and soil-transmitted helminths (discussed on this page), river blindness, trachoma, malaria, and lymphatic filariasis.
The program has previously consisted of mass administration of praziquantel to treat schistosomiasis, but is now also incorporating albendazole to treat soil-transmitted helminths.1 Both schistosomiasis and soil-transmitted helminths are parasite infections that can cause chronic malnutrition, pain, and anemia (and in some cases death). More on schistosomiasis; more on soil-transmitted helminths.
Evidence of effectiveness
General evidence on this program type
There is strong evidence from repeated, well-controlled clinical studies that praziquantel effectively reduces prevalence of schistosomiasis, which is further detailed at our report on schistosomiasis control. Evidence from the combination program (addressing both schistosomiasis and soil-transmitted helminths) is also encouraging, which is further detailed at our report on combined schistosomiasis and soil-transmitted helminths control.
Monitoring provided by The Carter Center
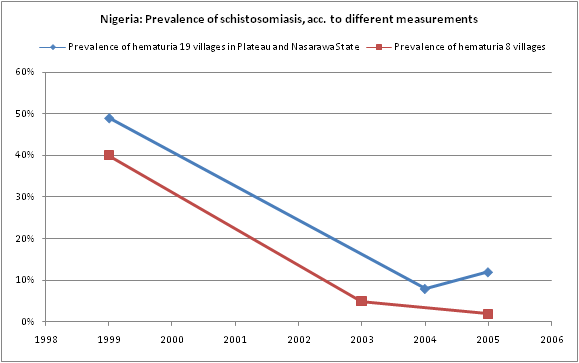
This chart below shows the decline in schistosomiasis since The Carter Center began its program.2 For explanations of the terms used in the chart below, see our glossary of terms. Data is not available for soil-transmitted helminths; it appears that drugs for this condition are only now being introduced into the program (see above).
What do you get for your dollar?
The Carter Center does not appear to make information available on how much this program spends. In general, independent estimates imply very strong cost-effectiveness for this type of program: $0.91-$5.14 to avert a schistosomiasis infection and, in the case of combination deworming (incorporating drugs targeting soil-transmitted helminths, which the Carter Center plans to do3 ), $3.50 for every additional year of schooling it brings about. In terms of disability-adjusted life-years (DALYs), cost-effectiveness is estimated at $3.36-$19 per DALY. Details on cost-effectiveness estimates can be found at our report on schistosomiasis control (schistosomiasis only) and at our report on combination deworming; see also, our discussion of the the DALY metric.
Sources
- Carter Center. Trachoma prevalence surveys determine need in Nigeria (PDF).
- Carter Center. Program Review for The Lions-Carter Center SightFirst River Blindness Programs (2007) (PDF).
- Carter Center. Website:
- How is The Carter Center involved? http://cartercenter.org/health/schistosomiasis/center.html (accessed April 19, 2010). Archived by WebCite® at http://www.webcitation.org/5p752K64F.
- 1
For Nigeria: "The components of SAFE, including azithromycin will be integrated with other ongoing community-based programs such as mass drug distribution for lymphatic filariasis, schistosomiasis, onchocerciasis, soil-transmitted helminths; and distribution of vitamin A and long-lasting insecticide-treated nets." Carter Center, "Trachoma Prevalence Surveys Determine Need in Nigeria," Pg 8.
- 2
Data is sourced as follows:
- Prevalence of hematuria in 19 villages: Carter Center, "Program Review for The Lions-Carter Center SightFirst River Blindness Programs (2007)," Pg 72.
- Prevalence of hematuria in 8 villages: Carter Center, "Program Review for The Lions-Carter Center SightFirst River Blindness Programs (2007)," Pg 115.
- 3
For Nigeria: "The components of SAFE, including azithromycin will be integrated with other ongoing community-based programs such as mass drug distribution for lymphatic filariasis, schistosomiasis, onchocerciasis, soil-transmitted helminths; and distribution of vitamin A and long-lasting insecticide-treated nets." Carter Center, "Trachoma Prevalence Surveys Determine Need in Nigeria," Pg 8.