This is an interim intervention report. We have spent limited time to form an initial view of this program and, at this point, our views are preliminary.
Summary
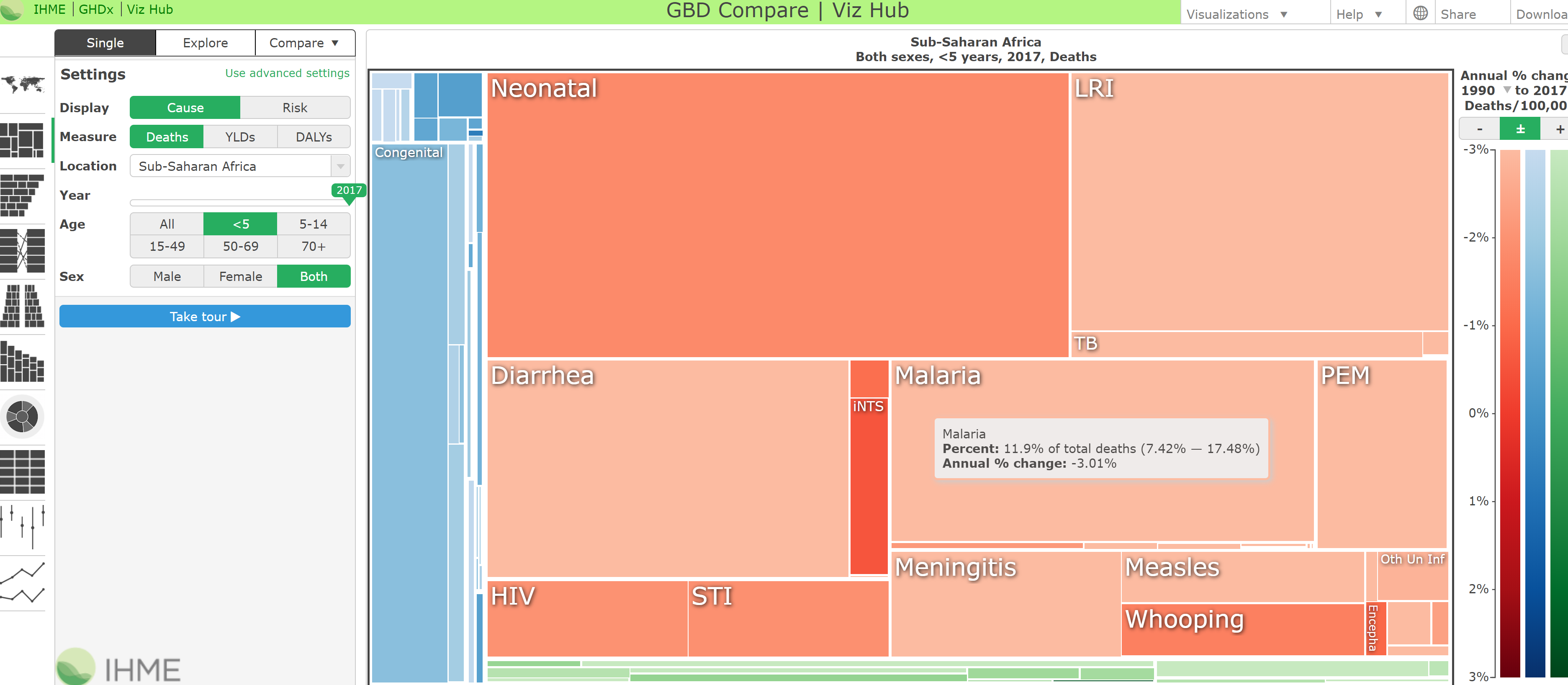
- What is the program? Malaria accounts for a large share of deaths for children under 5 in sub-Saharan Africa. Intermittent preventive treatment for infants (IPTi) is the provision of preventive antimalarial medicine to infants at routine vaccination visits.
- What is its evidence of effectiveness? There is evidence from nine randomized controlled trials (RCTs) included in a Cochrane meta-analysis that IPTi reduces cases of clinical malaria. While we view this evidence as strong, we have not thoroughly vetted the meta-analysis or component studies. In addition, the trials in the meta-analysis didn’t have the statistical power to detect an effect on mortality, which is the benefit we model in our cost-effectiveness analysis. We’re also uncertain about the extent to which findings from trials will generalize to future implementation and how much to discount effects based on concerns about resistance to antimalarial medicines.
- How cost-effective is it? Our preliminary cost-effectiveness estimate suggests that this program may be within the range of programs we would consider recommending funding. Antimalarial medicines are generally inexpensive and lead to a substantial decline in malaria, which accounts for a large share of deaths for the targeted population. This leads to high cost-effectiveness. However, we have uncertainty about program costs, differing levels of resistance across medications, the extent to which reduction in malaria incidence translates to reductions in mortality, and estimates for baseline malaria mortality rates.
- Does it have room for more funding? IPTi could be implemented in clinics throughout sub-Saharan Africa, where malaria risk is high, but to our knowledge, only one country (Sierra Leone) has a national IPTi policy, suggesting the potential for substantial room for more funding.
- Bottom line: This program appears promising, and we are investigating how we could potentially fund IPTi.
Published: August 2020; Last updated: March 2022
What is the problem?
Malaria is the fourth largest cause of death for children under 5 in sub-Saharan Africa, accounting for 12% of deaths.1 It is transmitted from person to person by infected mosquitoes2 and involves flu-like symptoms, including fever.3 When a case of malaria is severe, it leads to life-threatening complications, particularly in children.4 It is also believed that malaria can cause permanent disability (hearing impairment, visual impairment, epilepsy, etc.).5
Malaria is preventable with insecticide-treated nets and drugs (among other interventions), and it is treatable with drugs.6
What is the program?
According to the World Health Organization (WHO), “IPTi is a full therapeutic course of antimalarial medicine delivered to infants through routine immunization services, regardless of whether the child is infected with malaria. ... Treatment is given 3 times during the first year of life at approximately 10 weeks, 14 weeks, and 9 months of age, corresponding to the routine vaccination schedule of the Expanded Programme on Immunization (EPI).”7
IPTi is distinct from intermittent preventive treatment of children (IPTc), which provides antimalarial medicine through community volunteers outside of clinics. For more information on IPTc, which is also known as seasonal malaria chemoprevention (SMC), see our page on SMC. WHO recommends that IPTi and SMC should not be given in the same area.8
WHO recommends IPTi with sulfadoxine-pyrimethamine (SP), abbreviated as IPTi-SP, in countries in sub-Saharan Africa, in areas with moderate-to-high malaria transmission, except where parasites have too much resistance to SP.9
Other antimalarials could be used for IPTi in areas of high SP resistance, and several such drug combinations have been studied.10
Does the program have strong evidence of effectiveness?
Overall, we believe there is strong evidence that IPTi reduces clinical malaria, which gives us a moderate level of confidence that it reduces deaths due to malaria.
There is evidence from 9 trials included in Esu, Oringanje, and Meremikwu 2019, a Cochrane meta-analysis, that IPTi reduces cases of clinical malaria by 24%. We have a moderate level of confidence in this estimate; we have not thoroughly vetted the meta-analysis or reviewed component studies.
The trials in the meta-analysis were not powered to detect an effect on mortality, which is the benefit we model in our cost-effectiveness analysis, but we think it’s likely that reductions in malaria translate to reductions in mortality.
We’re also uncertain about the extent to which findings from trials will generalize to future implementation and how much to discount effects based on concerns about resistance to antimalarial medicines.
Main findings of Cochrane meta-analysis
Esu, Oringanje, and Meremikwu 2019 is a meta-analysis of 12 RCTs that compared IPTi to placebo or no intervention in malaria‐endemic areas.11 The majority of these RCTs used samples of children attending regular vaccinations.12
We have created a modified analysis of 9 trials (with 10,308 participants in total), based on analysis 1.1 in Esu, Oringanje, and Meremikwu 2019.13 Evidence from the 9 trials suggests that IPTi reduced the number of cases of clinical malaria by 24% (95% confidence interval: 17-31%).14 Among these trials, the follow-up duration for the effect size reported in the meta-analysis ranged from 6 to 15 months.15
For IPTi-SP specifically, there is evidence from 7 trials (with 8,627 participants in total) that the intervention reduced the number of cases of malaria by 22% (95% confidence interval: 16-27%).16
Internal validity
The authors of the meta-analysis believe that the large majority of studies had a low risk of bias. A summary of their judgements can be found in Figure 2, Esu, Oringanje, and Meremikwu 2019.17 Detailed explanations can be found in the ‘Characteristics of included studies’ tables.18 We have not vetted these judgements.
External validity
We have a moderate level of uncertainty about the extent to which findings from trials will generalize to future implementation, though we haven’t explored this issue in depth yet.
All studies included in our main estimate of the effect size on clinical malaria (see above) were of interventions identical or very similar to the WHO definition of IPTi.19
One study included in our analysis, Gosling 2009, provided medication that needs to be taken three days in a row. Patients were given the initial dose of medication at the vaccination visit, but field workers also visited participants on days 2 and 3 to ensure additional doses were taken.20 This additional compliance monitoring would be unlikely to be present in IPTi programs we would consider funding. (Our understanding is that in all other trials, the child was given the first dose at the clinic, and the caregiver was instructed to give the remaining doses at home, but this is not explicitly stated in Esu, Oringanje, and Meremikwu 2019.) We created a secondary modified analysis of analysis 1.1 in Esu, Oringanje, and Meremikwu 2019 that excludes Gosling 2009. Removing this study has almost no effect on the pooled effect size estimate.21
Mortality effects
Reduced mortality is the primary benefit we model in our cost-effectiveness analysis, but the trials in Esu, Oringanje, and Meremikwu 2019 were not powered to detect an effect on mortality. However, we think it’s likely that reductions in malaria translate to reductions in mortality.
In our preliminary cost-effectiveness analysis of IPTi, to estimate the effect on mortality, we assume that malaria mortality is reduced by the same fraction as malaria episodes. (We have made the same assumption in our other cost-effectiveness analyses of malaria programs. We discuss the assumption here in our analysis of seasonal malaria chemoprevention.)
We would expect that a reduction in clinical malaria from IPTi results in a similar reduction in malaria mortality, unless there was evidence that IPTi was disproportionately likely to prevent non-severe cases of malaria. There is limited evidence from Esu, Oringanje, and Meremikwu 2019 regarding the effect of IPTi on severe malaria. Only one relevant study reported effects on severe malaria.22 It found that IPTi reduced the number of severe malaria cases by 19%, but this estimate has a very wide 95% confidence interval that ranges from a 72% increase to a 62% reduction.23
Esu, Oringanje, and Meremikwu 2019 was not powered to detect effects on mortality, because deaths are a relatively rare outcome. The point estimate for the effect of IPTi on mortality was not statistically significant but was consistent with the effect on clinical malaria.24
Sulfadoxine-pyrimethamine vs other medications
WHO recommends IPTi with sulfadoxine-pyrimethamine, except where parasites have too much resistance to SP.25 It is generally believed that resistance to SP is increasing, and a significant amount of time has passed since IPTi-SP trials were conducted; the trials of IPTi-SP included in Esu, Oringanje, and Meremikwu 2019 were conducted between 1999 and 2013.26 We believe that the evidence is ambiguous about whether IPTi-SP is still likely to be effective in most areas.
The authors of Esu, Oringanje, and Meremikwu 2019 believe that, due to increasing SP resistance across Africa, SP may soon no longer be a useful drug in IPTi.27 The authors argue that the effect of IPTi-SP has weakened over time, pointing out that, while trials of IPTi-SP overall suggest positive effects, the most recent trials of IPTi-SP showed no effect.28 This argument is based on an informally observed trend, and we have not vetted it.
We are especially interested in the magnitude of the effect of SP resistance on the efficacy of IPTi, though we have not conducted a more systematic investigation of this effect. There is some evidence, of indirect relevance, from the literature on intermittent preventive treatment during pregnancy (IPTp) using SP. The evidence has weaknesses, and different analyses point in different directions.29
Several alternatives to sulfadoxine-pyrimethamine have been studied in IPTi.30 These alternatives are more expensive than SP (see below). We are unsure which medication would be most cost-effective in which areas for IPTi. An additional consideration regarding IPTi-SP is that WHO recommends that it only be implemented in areas where the prevalence of the dhps Lys540Glu mutation in malaria parasites is less than 50%. This requires testing for the presence of the mutation, which would make the intervention more complex and costlier.31
How cost-effective is the program?
We conducted a preliminary cost-effectiveness analysis. We found that IPTi may be highly cost-effective, and may be within the range of programs we would consider recommending funding.
Note that our cost-effectiveness analyses are simplified models that do not take into account a number of factors. There are limitations to this kind of cost-effectiveness analysis, and we believe that cost-effectiveness estimates such as these should not be taken literally due to the significant uncertainty around them. We provide these estimates (a) for comparative purposes and (b) because working on them helps us ensure that we are thinking through as many of the relevant issues as possible.
Note also that this cost-effectiveness analysis is in an early stage and therefore is not directly comparable to the cost-effectiveness analyses of our top charities. As a general rule, our estimates of a given program's cost-effectiveness tend to go down as we gain more information, and we would conduct a more thorough cost-effectiveness analysis before deciding to recommend funding to this program.
Antimalarial medicines are generally inexpensive and lead to a substantial decline in malaria, which accounts for a large share of deaths for the targeted population. This leads to high cost-effectiveness.
A sketch of the cost-effectiveness model is below:
- Deaths due to malaria: We use data from the Democratic Republic of the Congo (DRC) for illustration. It is a country with a high burden of malaria that is not eligible for seasonal malaria chemoprevention.32 Using the postneonatal malaria mortality rate for the DRC from the Institute for Health Metrics and Evaluation, GBD Results Tool, and adjusting for the targeted age range, we estimate a baseline malaria mortality rate of 654 deaths per 100,000 children in the age range covered by IPTi.33
- Effect of IPTi on malaria deaths: Our initial estimate for the effect of IPTi on the number of clinical malaria cases, a 24% reduction, is based on data from Esu, Oringanje, and Meremikwu 2019.34 We assume a 24% reduction in malaria cases translates to a 24% reduction in malaria deaths. We then adjust this estimate to account for indirect mortality reductions (malaria control interventions often have a larger effect on all-cause mortality than would be expected exclusively from declines in malaria-specific mortality35 ). We add further speculative adjustments for the internal and external validity of the study. These are highly subjective estimates which we use for the purposes of comparing the cost-effectiveness of different interventions as directly as possible to each other.
- Cost of IPTi: We would guess that the full programmatic costs of providing technical assistance to implement IPTi are considerably higher than the costs of the drugs alone. We use a preliminary guess of $4 per child receiving at least one dose of IPTi in our cost-effectiveness analysis, but we are highly uncertain about this estimate and plan to refine this estimate as we investigate specific funding opportunities.
- Cost-effectiveness: Using a guess of $4 per child treated with at least one dose of IPTi, our best guess is that IPTi averts one death for around $2,980, with the vast majority of lives saved being children under one year of age.
We have high uncertainty about program costs, differing levels of resistance across medications, the extent to which reduction in malaria incidence translates to reductions in mortality, and estimates for baseline malaria mortality rates. We believe IPTi is likely to remain cost-effective even under more pessimistic assumptions about these parameters.
- Costs. We have high uncertainty about the cost estimate that we use. Based on our guess that the costs of providing technical assistance to implement IPTi will be in the range of other technical assistance programs that involve stakeholder engagement, health provider training, monitoring, and procurement and supply chain management, we use a rough estimate for cost per child treated that is in the range of the costs of other technical assistance programs we have reviewed. Our estimate is considerably higher than estimates of cost per child treated from the academic cost-effectiveness analyses we found, which range from approximately $0.40 to $2.36 While we have not vetted these academic cost-effectiveness analyses, we would guess that they are an underestimate of the full costs of providing technical assistance to implement IPTi. We expect to be able to refine our estimates if we investigate a specific giving opportunity.
- SP resistance and choice of medication. We have high uncertainty about how much to discount effects due to the potential for higher levels of SP resistance since studies were conducted, as well as how effects vary across medications other than SP.
- Our main effect size estimate is a pooled estimate from IPTi studies that used different medications (however, the majority of these studies were conducted with SP, and the pooled estimate only from studies of IPTi-SP is very similar to our total pooled estimate).37
- We haven't explicitly modeled the effect of SP resistance in our cost-effectiveness analysis, but we include it in our external validity adjustment. We believe that SP resistance is higher today in many areas, but we have not investigated to what degree this is the case. There is limited evidence on the effect of SP resistance on the efficacy of IPTi-SP, which we discuss above.
- Baseline mortality. Our estimate of malaria mortality in children in the absence of IPTi uses data for the DRC from the @Institute for Health Metrics and Evaluation, GBD Results tool@ and adjusts for the age range that IPTi covers.38 However, the baseline mortality rate among children targeted by IPTi will depend on the delivery schedule (and thus the age range that IPTi will cover) and the country of implementation.
- Subjective adjustments. Our estimates of the internal and external validity of the study are highly subjective. We also apply subjective adjustments for the long-term developmental effects of reducing infant morbidity and for the effects of reducing transmission on mortality in the untreated population. We have a high level of uncertainty about the magnitude of these effects.
Does the program appear to have room for more funding?
To our knowledge, Sierra Leone is the only country that has implemented IPTi.39 The government’s policy is that IPTi should be in place at vaccination clinics throughout Sierra Leone, but we have not investigated the coverage that has actually been achieved. We expect that there is likely room for more funding for this intervention, given that WHO has recommended IPTi-SP for many areas of sub-Saharan Africa, and no countries except Sierra Leone have a national IPTi policy.
We are aware of a Unitaid call for grant proposals for IPTi. We are uncertain about whether IPTi could productively absorb more funding in the short term after Unitaid makes its grants, but we plan to investigate opportunities to give such funding.
Organizations that implement this program
We are investigating potential charities that could implement IPTi. We are aware that ICAP at Columbia University, a research and technical assistance organization, provided technical assistance to the government of Sierra Leone for its scale-up of IPTi.40
Potential negative impacts of the program
We are aware of some potential negative impacts of IPTi. Based on a cursory investigation, they did not seem likely to significantly offset the programs’ positive impacts, so we have not prioritized looking into them further at this stage, though we may conduct additional research on these issues. (More information is available here, where we have considered similar issues in the context of SMC.)
- Resistance. IPTi could increase rates of drug resistance that would make the drug less effective or ineffective at treating malaria for people living in the program region (see discussion of resistance above). SP is rarely used as a first-line treatment for malaria,41 so for IPTi-SP, the main risk would be to the efficacy of IPTi-SP itself.
- Possible rebound effects. Some researchers have hypothesized that after IPTi treatment ends, malaria may rebound to a higher level than would have occurred without treatment, due to the fact that the treated children are less able to develop immunity to malaria.42 In Esu, Oringanje, and Meremikwu 2019, 6 RCTs of IPTi had a post-intervention follow-up, none of which find evidence of a rebound effect.43 We have a moderate level of confidence in these findings, but have not vetted the individual studies.
- Serious adverse drug reactions. Esu, Oringanje, and Meremikwu 2019 found evidence that IPTi did not lead to serious adverse events for SP and dihydroartemisinin‐piperaquine (DHAP).44
Focus of further investigation
Our priority is to talk with potential IPTi implementers. Once we start investigating specific funding opportunities, we plan to refine our estimates of the most uncertain inputs into our cost-effectiveness analysis.
Our process
Esu, Oringanje, and Meremikwu 2019, a Cochrane Collaboration meta-analysis, is the source of our effect size estimate. Because the meta-analysis is relatively up to date, and because we believe that Cochrane Collaboration meta-analyses are generally of high quality, we did not consider other meta-analyses or studies.
Sources
{kind=link}
- 1
2017 figures from Institute for Health Metrics and Evaluation, GBD Compare Data Visualization, 2018 (using search parameters for under-5 deaths in sub-Saharan Africa).
- 2
"Human infection begins when the malaria vector, a female anopheline mosquito, inoculates plasmodial sporozoites from its salivary gland into humans during a blood meal. The sporozoites mature in the liver and are released into the bloodstream as merozoites. These invade red blood cells, causing malaria fevers. Some forms of the parasites (gametocytes) are ingested by anopheline mosquitoes during feeding and develop into sporozoites, restarting the cycle." Jamison et al., Disease Control Priorities in Developing Countries, 2006, Pg 413.
- 3
"In the early stages, malaria symptoms are sometimes similar to those of many other infections caused by bacteria, viruses, or parasites. It can start with flu-like symptoms. Symptoms may include:
- Fever. This is the most common symptom.
- Chills.
- Headache.
- Sweats.
- Fatigue.
- Nausea and vomiting.
- Body aches.
- Generally feeling sick.”
- 4
“Many children who are admitted will be suffering from life-threatening complications of Plasmodium falciparum malaria, such as coma and convulsions (cerebral malaria), severe anemia (requiring urgent lifesaving transfusion), and rapid breathing (due to severe metabolic acidosis). Approximately 90% of the world’s falciparum infections and deaths occur in sub-Saharan Africa, the latter almost entirely in children younger than 5 years of age.” Maitland 2016.
- 5
- “CM [cerebral malaria] is associated with hemiparesis, quadriparesis, hearing and visual impairments, speech and language difficulties, behavioral problems, epilepsy, and other problems (table 21.3).” Jamison et al., Disease Control Priorities in Developing Countries, 2006, Pg 417.
- See Jamison et al., Disease Control Priorities in Developing Countries, 2006, Pg 416, Table 21.3 for estimates of cases of hearing impairment, visual impairment, epilepsy, etc. caused by malaria.
- 6
- “Preventive chemotherapies are key elements of the comprehensive package of malaria prevention and control measures recommended by WHO. ... The objective of these interventions is to prevent malarial illness by maintaining therapeutic drug levels in the blood throughout the period of greatest malarial risk.” World Health Organization, “Malaria: Preventive therapies”.
- “The 2 core interventions for malaria vector control are insecticide-treated nets (ITNs) and indoor residual spraying (IRS).” World Health Organization, “Malaria: Entomology and vector control”.
- “Malaria is a preventable and treatable disease. ... WHO recommends artemisinin-based combination therapies (ACTs) for the treatment of uncomplicated malaria caused by the P. falciparum parasite. By combining 2 active ingredients with different mechanisms of action, ACTs are the most effective antimalarial medicines available today.” World Health Organization, “Malaria: Overview of malaria treatment”, 2018
- 7
World Health Organization, “Malaria: Intermittent preventive treatment in infants (IPTi)”
- 8
“In areas where SMC is implemented, intermittent preventive treatment in infants (IPTi) should not be deployed.” World Health Organization, “Malaria: Seasonal Malaria Chemoprevention”, 2017.
- 9
“WHO recommends the co-administration of SP-IPTi with DTP2/Penta2, DTP3/Penta3 and measles immunization to infants, through routine EPI in countries in Sub-Saharan Africa, in areas
- a. with moderate-to-high malaria transmission (Annual Entomological Inoculation Rates ≥ 10), and
- b. where parasite resistance to SP is not high - defined as a prevalence of the Pfdhps 540 mutation of ≤ 50%.”
- 10
“Alternative drug combinations to SP evaluated in the included trials were amodiaquine (AQ) (Massaga 2003 TZA), chlorproguanil‐dapsone (CD) (Gosling 2009 TZA; Odhiambo 2010 KEN), dihydroartemisinin‐piperaquine (DHAP) (Bigira 2014 UGA), and mefloquine (MQ) (Gosling 2009 TZA). One trial evaluated drug combinations that included SP; SP+ artesunate (AS) (Odhiambo 2010 KEN). Another drug combination evaluated was AQ+AS (Odhiambo 2010 KEN).” Esu, Oringanje, and Meremikwu 2019, Pg 15.
- 11
- ”Selection criteria: We included randomized controlled trials (RCTs) that compared IPT to placebo or no intervention in infants (defined as young children aged between 1 to 12 months) in malaria-endemic areas. … Main results: We included 12 trials that enrolled 19,098 infants.” Esu, Oringanje, and Meremikwu 2019, Pg 1.
- The meta-analysis, which includes studies published until December 3, 2018, is relatively up to date. We have not looked for studies published after December 3, 2018.
- ”All eligible published studies found in the last search (3 Dec, 2018) were included” Esu, Oringanje, and Meremikwu 2019, Pg 2.
- 12"Ten trials co-administered IPT with routine EPI vaccinations (Armstrong Schellenberg 2010 TZA;
Chandramohan 2005 GHA; Dicko 2012MLI; Gosling 2009 TZA; Kobbe 2007 GHA; Macete 2006 MOZ; Massaga 2003 TZA; Mockenhaupt 2007 GHA; Odhiambo 2010 KEN; Schellenberg 2001 TZA)." Esu, Oringanje, and Meremikwu 2019, Pg 15. - 13
- See analysis 1.1 in Esu, Oringanje, and Meremikwu 2019, Pgs 44-45.
- See our modification of analysis 1.1 for total participant count (adding together IPTi and Control participant totals)
- 14
- See our modification of analysis 1.1 from Esu, Oringanje, and Meremikwu 2019.
- We calculate the reduction in number of cases and the 95% confidence interval by subtracting the total rate ratio from 1.
- Armstrong Schellenberg 2010 and Dicko 2012 did not report clinical malaria as an outcome and are not included in analysis 1.1 in Esu, Oringanje, and Meremikwu 2019.
- See Esu, Oringanje, and Meremikwu 2019, Pgs 25-41, Characteristics of included studies (all other studies list “Clinical malaria” among “Outcomes included in the review”) and Pgs 44-45, Analysis 1.1.
- We excluded one trial, Bigira 2014, because it studied an intervention that is significantly different from what WHO defines as IPTi, and we believe it’s significantly different from what charities we might consider funding would understand by IPTi.
- Bigira 2014 studied an intervention that provided “dihydroartemisinin‐piperaquine (DHAP) ... once daily for three consecutive days each month given monthly from 6 months to 24 months of age. Each drug was provided for administration at home [by the child’s parents]” Esu, Oringanje, and Meremikwu 2019, Pg 27.
- Note that, for two of the studies, we were not able to find the source of the effect size reported in the meta-analysis. These studies are Grobusch 2007, where the meta-analysis gives a rate ratio for clinical malaria of 0.88, and Schellenberg 2001, where the meta-analysis gives a rate ratio of 0.62. (Esu, Oringanje, and Meremikwu 2019. Pgs 44-45, Analysis 1.1).
- See our modification of analysis 1.1 from Esu, Oringanje, and Meremikwu 2019.
- 15
See Esu, Oringanje, and Meremikwu 2019, Pgs 25-41, Characteristics of included studies. The duration of the effect is discussed in more detail in another footnote below.
- 16
- See our modification of analysis 1.1 from Esu, Oringanje, and Meremikwu 2019.
- We calculate the reduction in number of cases and the 95% confidence interval by subtracting the total rate ratio from 1.
- For total participant count, we added together IPTi and Control participant totals.
- 17
- 18
Esu, Oringanje, and Meremikwu 2019, Pgs 25-41.
- 19
Details on all twelve interventions included in Esu, Oringanje, and Meremikwu 2019 are available here:
Name Intervention Notes Armstrong Schellenberg 2010 TZA “sulfadoxine‐pyrimethamine (SP) delivered in intervention divisions through existing government health centres when children presented for their routine EPI vaccine doses of DPT2, DPT3, and measles (given at 2, 3, and 9 months of age, respectively” Pg 26 Not included in our analysis because it did not report on clinical malaria. Bigira 2014 UGA “dihydroartemisinin‐piperaquine (DHAP) ... once daily for three consecutive days each month given monthly from 6 months to 24 months of age. Each drug was provided for administration at home according to weight‐based guidelines. Participants did not receive routine immunization along with IPTi” Pg 27 Not included in our analysis because the intervention is different from what is commonly understood as IPTi Chandramohan 2005 GHA “SP (500 mg sulfadoxine and 25 mg pyrimethamine) first dose given at 2 months, second dose at 3 months, third at 9 months, and fourth dose at 12 months. 1/2 tablet at time of DPT‐2 and DPT3 vaccines; 1 tablet at time of measles vaccine and at 12 months” Pg 29 Included in our analysis. Dicko 2012 MLI “SP (500 mg sulfadoxine and 25 mg pyrimethamine) first dose given at 3 months, second dose at 4 months, and third at 9 months of age. 1/2 tablet at time of DPT‐2 and DPT3 vaccines and measles/yellow fever vaccine” Pg 30 Not included in our analysis because it did not report on clinical malaria. Gosling 2009 TZA - Complicated combination of antimalarials at 2, 3, and 9 months of age (details on Pgs 31-32).
- “All treatments at the health facility were observed and administered with routine immunizations. Field workers visited participants on days 2 and 3 to ensure doses were taken.” Pg 32
Included in our analysis. Additional compliance monitoring would be unlikely to be present in IPTi programs we would consider funding. Grobusch 2007 GAB “SP (500 mg sulfadoxine and 25 mg pyrimethamine) given at 3, 9, and 15 months of age” Pg 33 Included in our analysis. Kobbe 2007 GHA “Intervention: SP (250 mg sulfadoxine and 12.5 mg pyrimethamine) given at 3, 9, and 15 months of age: One tablet at 3, 9, and 15 months of age” Pg 34 Included in our analysis. Macete 2006 MOZ “SP given at age 3, 4, and 9 months of age and administered according to weight” Pg 35 Included in our analysis. Massaga 2003 TZA Starting at 12 to 16 weeks, every 2 months for 6 months, i.e., at approximately 3, 5, and 7 months (details on Pg 37) Included in our analysis. Mockenhaupt 2007 GHA “SP at approximately 3, 9, and 15 months of age” Pg 38 Included in our analysis. Odhiambo 2010 KEN One of three medications, administered at routine EPI visits ‐10 weeks, 14 weeks and 9 months (details on Pg 39) Included in our analysis. Schellenberg 2001 TZA “SP (25 mg/kg sulfadoxine and 1.25 mg/kg pyrimethamine) first dose at 2 months, second dose at 3 months, and third at 9 months” Pg 40 Included in our analysis. - 20
“All treatments at the health facility were observed and administered with routine immunizations. Field workers visited participants on days 2 and 3 to ensure doses were taken.” Esu, Oringanje, and Meremikwu 2019, Pg 32
- 21
Compare the total rate ratio from our primary modified analysis to that of our secondary modified analysis.
- 22
- Only two studies reported effects on severe malaria: Bigira 2014 and Mockenhaupt 2007. (Esu, Oringanje, and Meremikwu 2019, Pg 45, Analysis 1.2).
- We excluded Bigira 2014 from our analysis because the intervention studied was dissimilar to IPTi. See footnotes above for additional explanation of why this study was excluded.
- 23
- Esu, Oringanje, and Meremikwu 2019, Pg 45, Analysis 1.2.
- We calculate the reduction in severe malaria cases (and 95% confidence interval) by subtracting the rate ratio (and 95% CI) for Mockenhaupt 2007 GHA from 1.
- 24
- See Esu, Oringanje, and Meremikwu 2019, Analysis 1.3, Pgs 45-46.
- The all-cause mortality risk ratio for IPTi-SP was 0.93 [95% confidence interval 0.74-1.15].
- The all-cause mortality risk ratio for IPTi with any drug combination was 0.94 [95% confidence interval 0.77-1.14].
- Neither all-cause mortality risk ratio is statistically significant because the 95% confidence interval crosses 1.
- See Esu, Oringanje, and Meremikwu 2019, Analysis 1.3, Pgs 45-46.
- 25
“WHO recommends the co-administration of SP-IPTi with DTP2/Penta2, DTP3/Penta3 and measles immunization to infants, through routine EPI in countries in Sub-Saharan Africa, in areas
- a. with moderate-to-high malaria transmission (Annual Entomological Inoculation Rates ≥ 10), and
- b. where parasite resistance to SP is not high - defined as a prevalence of the Pfdhps 540 mutation of ≤ 50%.”
- 26
“IPTi with sulfadoxine-pyrimethamine (SP) was evaluated in 10 trials from 1999 to 2013 (n = 15,256).” Esu, Oringanje, and Meremikwu 2019, Pg 1.
- 27
“Levels of parasite drug resistance to SP across Africa have increased and have led most countries to abandon SP as a monotherapy in first‐line treatment. ... Current levels of SP resistance in Africa, suggest that the period over which SP remains useful as the drug of choice for IPTi may be very limited.” Esu, Oringanje, and Meremikwu 2019, Pg 20.
- 28
“although the review shows that IPTi with SP probably had a protective effect against clinical malaria ... the finding is based on trials conducted over a 14‐year period. A close look at the meta‐analysis shows an attenuation of the effect of IPTi‐SP over time with the most recent trials showing no effect.” Esu, Oringanje, and Meremikwu 2019, Pg 20.
- 29
- ter Kuile, van Eijk, and Filler 2007 matched IPTp studies by year and location with treatment studies of SP among symptomatic children, and measured SP resistance as the proportion of total treatment failures in symptomatic children by day 14. They find that the effect of IPTp did not vary by SP resistance levels.
- ”An eligible treatment study in children was considered a match with a trial
of IPT with sulfadoxine-pyrimethamine during pregnancy if it was conducted within the same country and during the same period (maximum of 2 years difference).” Pg 2604-2605 - Resistance to “Sulfadoxine-Pyrimethamine is: “Defined as the proportion of total treatment failure in symptomatic children by day 14.” Table 1, Pg 2606.
- ”The IPT reduced placental malaria (relative risk [RR], 0.48; 95% CI, 0.35-0.68), low birth weight (RR, 0.71; 95% CI, 0.55-0.92), and anemia (RR, 0.90; 95% CI, 0.81-0.99). The effect did not vary by sulfadoxine-pyrimethamine resistance levels (range, 19%-26%).” Pg 2603.
- ”An eligible treatment study in children was considered a match with a trial
- However, this study:
- is from 2007, and SP resistance is likely to have increased since then,
- matches treatment studies in children with IPTp studies if both were conducted in the same country, whereas SP resistance could vary at the subnational level.
- van Eijk et al. 2019 is a meta-analysis of the effect of molecular markers of SP resistance on the efficacy of IPTp at reducing birth weight. Greater prevalence of the dhps Lys540Glu molecular marker of SP resistance was correlated with a weaker effect of IPTp on low birth weight.
- ”Background: Resistance of Plasmodium falciparum to sulfadoxine-pyrimethamine threatens the antimalarial effectiveness of intermittent preventive treatment during pregnancy (IPTp) in sub-Saharan Africa. We aimed to assess the associations between markers of sulfadoxine-pyrimethamine resistance in P falciparum and the effectiveness of sulfadoxine-pyrimethamine IPTp for malaria-associated outcomes.” Pg 546.
- ”In our meta-analysis of aggregated data from 57 clinical studies, increases in the prevalence of two molecular markers of sulfadoxine resistance were associated with clear reductions in the effectiveness of sulfadoxine-pyrimethamine IPTp to avert low birthweight. … In our parallel analysis of individual participant data from nationally representative surveys, sulfadoxine-pyrimethamine IPTp was associated with a significant but modest protective effect against low birthweight in areas where the P falciparum dhps Lys540Glu mutation prevalence was 90% or higher and the prevalence of sextuple-mutant parasites was less than 10%.16 However, these surveys also showed that, in areas where sextuple-mutant parasites are common (pooled prevalence estimate 37%), sulfadoxine-pyrimethamine IPTp did not protect against low birthweight. These findings are consistent with our understanding of the incremental increase in resistance to sulfadoxine-pyrimethamine with successive mutations in the dhfr and dhps genes” Pg 553.
- Furthermore, Esu, Oringanje, and Meremikwu 2019 wrote that “studies in pregnant women have demonstrated that SP could still be effective even in the presence of high levels of SP resistance (Desai et al. 2015; Likwela et al. 2012).” Pg 20.
- We have only taken a cursory look at ter Kuile, van Eijk, and Filler 2007 and van Eijk et al. 2019.We have not looked at Desai et al. 2015 and Likwela et al. 2012.
- ter Kuile, van Eijk, and Filler 2007 matched IPTp studies by year and location with treatment studies of SP among symptomatic children, and measured SP resistance as the proportion of total treatment failures in symptomatic children by day 14. They find that the effect of IPTp did not vary by SP resistance levels.
- 30
“Alternative drug combinations to SP evaluated in the included trials were amodiaquine (AQ) (Massaga 2003 TZA), chlorproguanil‐dapsone (CD) (Gosling 2009 TZA; Odhiambo 2010 KEN), dihydroartemisinin‐piperaquine (DHAP) (Bigira 2014 UGA), and mefloquine (MQ) (Gosling 2009 TZA). One trial evaluated drug combinations that included SP; SP+ artesunate (AS) (Odhiambo 2010 KEN). Another drug combination evaluated was AQ+AS (Odhiambo 2010 KEN).” Esu, Oringanje, and Meremikwu 2019, Pg 15.
- 31
- “The WHO recommends IPTi with sulfadoxine-pyrimethamine (SP) in areas with moderate-to-high malaria transmission in sub-Saharan Africa where the prevalence of the pfdhps-540E allele of the P falciparum parasite is less than 50% (WHO 2010; WHO 2011).” Esu, Oringanje, and Meremikwu 2019, Pg 10.
- “The research capacity to obtain and monitor relevant resistance data is often inadequate in endemic countries of sub‐Saharan Africa. The complexity of the IPTi policy may have also affected the uptake”. Esu, Oringanje, and Meremikwu 2019, Pg 10.
- 32
- According to our page on seasonal malaria chemoprevention, “SMC is recommended for deployment in areas: where more than 60% of the annual incidence of malaria occurs within 4 months …”
- According to USAID, “Approximately 97 percent of the population [of DRC] lives in zones with stable malaria transmission lasting 8 to 12 months per year.” USAID, "U.S. President’s Malaria Initiative Democratic Republic of the Congo Malaria Operational Plan FY 2020", Pg 9.
- 33
See our preliminary cost-effectiveness analysis, “Results” sheet, “Baseline mortality rates” section.
- 34
See our modification of analysis 1.1 from Esu, Oringanje, and Meremikwu 2019.
- 35
"During randomized controlled intervention trials aimed at reducing the incidence of infection (but not 100 percent protective), the all-cause mortality of children is often reduced more than would be attributed by [verbal autopsy] diagnosis of malaria." Jamison et al., Disease and Mortality in Sub-Saharan Africa, 2006, p. 204
- 36
- We referenced two sources, Conteh et al. 2010 (specifically Conteh et al. 2010, Supporting Information, Table S4) and Hutton et al. 2009.
- Conteh et al. 2010 estimates costs for “policy change; community sensitization; behaviour change and communication; drug purchase and distribution; training; administration of IPTi in health facilities and management.” Pg 2.
- Hutton et al. 2009 “took into account all costs involved in implementing [the intervention], including the costs of planning, delivery and monitoring. [They] also included all costs associated with policy change (strategy definition), sensitization (meetings with health sector stakeholders and district level health managers), behaviour change (communication to the population, staff training, intervention monitoring), the IPTi drug SP (import, purchase, storage and distribution), and drug administration (drug delivery, mothers’ education, and filling out the health card).” Pg 124.
- We referenced two sources, Conteh et al. 2010 (specifically Conteh et al. 2010, Supporting Information, Table S4) and Hutton et al. 2009.
- 37
- See our modified analysis of analysis 1.1 in Esu, Oringanje, and Meremikwu 2019.
- The pooled estimate for studies of IPTi-SP is 0.22 (1 minus the rate ratio, 0.78).
- The total pooled estimate is 0.24 (1 minus the rate ratio, 0.76).
- Individual effect size estimates for each medication would provide us with cost-effectiveness estimates that were somewhat more accurate, though it is unclear how much so. We have not prioritized calculating individual effect size estimates.
- 38
We obtained malaria mortality estimates for the Democratic Republic of the Congo and Nigeria in 2017 from @Institute for Health Metrics and Evaluation, GBD Results tool@ (Context = Cause; Metric = Rate).
- 39
“To date, NMCPs have not prioritized IPTi in any country except Sierra Leone. Sierra Leone, after piloting IPTi in four districts in 2017, scaled up IPTi nationally to all 14 districts in mid-2018.” USAID, "U.S. President’s Malaria Initiative FY 2020 Guidance", 2019, Pg 91.
- 40
“The NMCP endorsed a pilot study of IPTi activities in four districts (Kambia, Pujehun, Kenema, and Western Area Rural) which commenced in 2017, and findings from the pilot informed the national scale-up that was completed in 2018. CDC Sierra Leone supported ICAP to conduct an external evaluation of the IPTi pilot in Kambia district and final results are expected in early 2019. The IPTi pilot study and scale-up received technical and financial contributions including SP procurement from non-PMI partners and donors.” USAID, "Sierra Leone: Malaria Operational Plan FY 2018 & FY 2019", Pg 18.
- 41
“Levels of parasite drug resistance to SP across Africa have increased and have led most countries to abandon SP as a monotherapy in first‐line treatment” Esu, Oringanje, and Meremikwu 2019, Pg 20.
- 42
“Of concern is whether administering anti-malarial drugs interrupts development of immunity and leads to decreased malaria-specific immunity and/or a rebound of increased morbidity and mortality after termination of treatment.” O’Meara, Breman, and McKenzie 2005, “Immunity and Rebound” section.
- 43
- “We evaluated post‐intervention follow‐up effects of IPTi to determine if the effects were sustained beyond the intervention period. We found no evidence of an effect of IPTi on the risk of clinical malaria (Analysis 3.1), risk of death from any cause (Analysis 3.2), in the period after the discontinuation of the intervention. Similarly, IPTi had no effect on the risk of hospital admission (Analysis 3.3) and the risk of anaemia (Analysis 3.4) in the period after the discontinuation of the intervention. This lack of a sustained effect of IPTi in the period after the discontinuation of the intervention was consistent across all medicines.” Esu, Oringanje, and Meremikwu 2019, Pg 19.
- In particular, the rate ratios for clinical malaria in the post-intervention phase were 1 (Mefloquine, 95% CI 0.8,1.26), 1 (SP, 95% CI 0.93,1.07), 0.99 (amodiaquine-artesunate, 95% CI 0.82,1.2), and 0.99 (SP-Artesunate, 0.81,1.2). Esu, Oringanje, and Meremikwu 2019, Pg 52, Analysis 3.1.
- 44
The adverse events reported are shown in Analysis 4.1 and Analysis 4.2 (Esu, Oringanje, and Meremikwu 2019, Pgs 55-56).