A note on this page's publication date
The content on this page has not been recently updated. This content is likely to be no longer fully accurate, both with respect to the research it presents and with respect to what it implies about our views and positions.
Click here for this overview in PDF format.
In our first year, we evaluated charities that work in the poorest parts of the world, aiming to save lives and otherwise improve living conditions. We found that:
- Opportunities for a donor to help people are enormous, given the vast numbers of people who die (and otherwise suffer) from conditions that are relatively simple and inexpensive to correct. We believe that donors can accomplish far more donating to the developing-world organizations we recommend than they can through any developed-world program we know of.
- However, different programs and delivery methods vary widely in effectiveness and cost, and the most popular and marketable programs are not necessarily the best (or even effective at all).
- Population Services International stands out for its commitment to thorough, consistent self-monitoring and evaluation; by marketing life-saving and –improving materials such as condoms, bednets, and water purification kits, PSI appears to be improving quality of life with great cost-effectiveness.
- Partners in Health is another standout organization that builds comprehensive community health programs, staffing full-service hospitals and health centers with trained local staff. Unlike many international charities, which focus on a particular disease or problem at a time, PIH is notable for its emphasis on serving people's needs holistically and turning no one away.
- Our first round of research has also made us aware of many approaches to developing-world aid that we consider high-potential, but need to research more carefully to have confidence in. We plan to research them more in the coming year.
Below are the highlights of what we learned. For more detail, see our reports on individual causes:
The problem
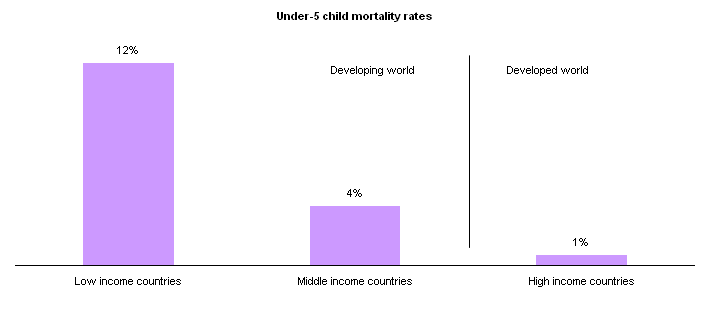
Every year, over 6 million people die of preventable causes in sub-Saharan Africa. The vast majority of them are children under the age of 5.
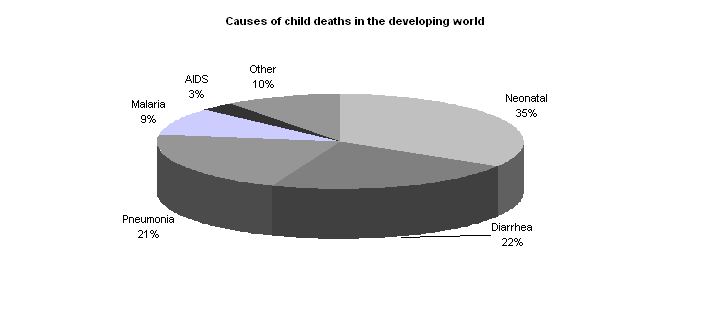
(The data in the charts below comes from The Lancet's Global Health Network's series on child survival. All papers are available here. Data in the first chart below comes from Victora et al. 2003 and data for the second comes from Black et al. 2003.)
Potential solutions
Proven, effective interventions to prevent save lives in the developing world are often simple and inexpensive (Jones et al. 2003).
| Cause of death | Interventions |
|---|---|
| Neonatal | - Breastfeeding - Protective nets - Clean delivery |
| Diarrhea | - Breastfeeding - Complementary feeding - Water, sanitation, and hygiene - Zinc and Vitamin A supplements - Oral rehydration therapy |
| Pneumonia | - Breastfeeding - Complementary feeding - Zinc supplements - Antibiotics |
| Measles | - Measles vaccine - Complementary feeding - Vitamin A supplements |
| Malaria | - Protective nets - Complementary feeding - Antimalarial drugs |
| HIV/AIDS | - Replacement feeding |
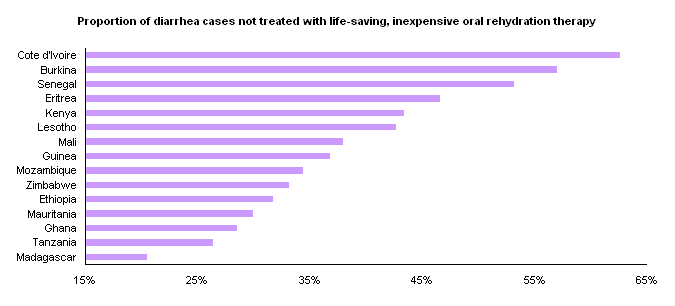
In many cases, these proven interventions are only sparsely implemented and could be expanded with well-directed donations.
(Data in the chart below comes from USAID's Demographic and Health Surveys.)
The importance of strategic giving
The developing world presents enormous opportunities to help people, but also major challenges for charities and for donors. Cost-effectiveness of different approaches varies wildly, and the most popular and “marketable” interventions are not necessarily the most effective. The first chart on this page gives an example of this: projects to build wells, latrines, and other sanitation infrastructure have been estimated to be significantly more costly than other methods of improving hygiene and reducing hygiene-related deaths.
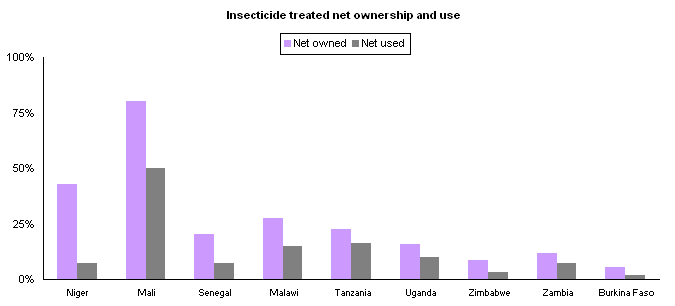
And even for fundamentally sound interventions, effectiveness can vary widely by area and approach (see, for example, the variations in bednet utilization seen in the second chart). For this reason, we find thorough and consistent monitoring to be essential.
(Data in the chart below comes from Varley et al. 1998.)

(Data in the chart below comes from USAID's Demographic and Health Surveys.)
The difficulty of finding a well-documented organization
From our first year of research, one of our main findings is that most aid organizations conduct a huge variety of activities, and are unwilling or unable to share information about what they're funding and whether it's working. In evaluating large, household-name organizations, we were rarely able to get summaries of how much was being spent in each country (and on what activities), and we were even more rarely given information on how activities are progressing and what the impact on the nearby populations has been. We were generally told that information of this kind is sometimes available for specific projects, but that no organization-wide aggregation exists.

Two standout organizations
We've identified two organizations that stand out for their dedication to consistent, well-monitored, cost-effective activities that we can confidently say are improving health and saving lives. We feel they represent much better options for a donor than typical large-scale, diverse charities whose projects range all over the map.
Population Services International (PSI) sells and promotes products aimed at improving health and quality of life for people in the developing world. Rather than distributing these products for free, it charges below-market prices, reasoning that this practice improves the likelihood that its products will get to people who value them and are likely to use them.
PSI thoroughly tracks its activities, costs, and results throughout the world. The below table gives a sample of just how inexpensively its activities can make a real difference; for more detail, see our full report here.
| Problem | Activity | Cost per significant life change (estimate) | Other benefits |
|---|---|---|---|
| HIV/AIDS | Condoms; promoting safe sexual behavior | $700 per HIV infection averted | Averting unwanted pregnancies; slowing spread of STDs |
| Malaria | Protective bednets | $750 per life saved from malaria | Averting non-fatal malaria cases |
| Diarrhea | Water purification kits and simple medication | $250 per life saved from diarrhea | Averting non-fatal diarrhea cases |
Partners in Health takes a different approach: it runs comprehensive community health programs, staffing full-service hospitals and health centers with trained local staff. While we don't believe this approach is as “cost-effective” as mass distribution of materials, we still think it could be saving a human life for every ~$3500, with the added benefit of training local staff and thereby improving an area's long-term health care capacity. We also believe that this approach stands out from other programs because of its emphasis on serving people's needs holistically, rather than narrowly targeting specific diseases. For more detail, see our full report here.
More to come
In our first year of research, we have found that the developing world presents enormous opportunities for a donor, and thoroughly evaluated two standout organizations; but we have also raised more questions than we've answered about the diverse problems people face, and the diverse solutions that different charities offer. In the coming year, we hope to research the following issues, which we covered only superficially in our first year:
- Vaccination programs, particularly those of the Measles Initiative and the GAVI Alliance. Preliminary evidence suggests that these programs could be significantly more cost-effective (and scalable) ways to save lives than those of our current strongest applicants.
- Programs focusing on neglected tropical diseases (NTDs), which cause extreme debilitation including severe skin disease and permanent blindness and can be treated relatively simply and cheaply, but generally receive little attention from donors and the media. Preliminary evidence suggests that these programs could be significantly more cost-effective (and scalable) ways to bring about significant life change than those of our current strongest applicants.
- Malnutrition-centered programs. We believe that malnutrition is extremely widespread in the developing world, and is strongly connected to other health and economic problems, but that many food aid programs could be doing more harm than good. A good malnutrition program could make enormous and highly cost-effective differences in quality of life.
- Other health related programs, including sanitation and water facilities, interventions focused on the major causes of child mortality: diarrhea, pneumonia, malaria, and more.
- Microfinance and economic empowerment programs. Intuitively (and according to very limited and preliminary evidence), we believe that microfinance programs may be uniquely cost-effective ways of accomplishing a goal that our current recommended charities do not: helping people escape poverty and permanently raise their standard of living. Our initial research focused on large international organizations, but we now believe there is more potential – for this particular cause – in smaller organizations with a more direct relationship to their population served.
- Comprehensive aid programs. We will be sure to seek out programs, such as the Millennium Villages Project (which we were not able to assess in 2007), that take a by-region rather than by-problem approach; we believe such programs are promising in terms of their potential economies of scale (addressing as many problems as possible after having dealt with the fixed cost of setting up offices) and in terms of their ability to adjust quickly to changing conditions.
Conclusion
We recommend Population Services International and Partners in Health to donors interested in helping people extremely cost-effectively. We believe that further research will reveal many more excellent opportunities for donors; because of the extreme poverty of the developing world, the same funds can likely have a much larger impact when spent in this area.
References
- Victora, C. G., Wagstaff, A., Schellenberg, J. A., Gwatkin, D., Claeson, M. & Habicht, J. 2003, ”˜Applying an equity lens to child health and mortality: more of the same is not enough', The Lancet, vol. 362, pp. 233-41. (Available online)
- Black, R. E., Morris, S. S. & Bryce, J. 2003. ”˜Where and why are 10 million children dying every year?', The Lancet, vol. 361, pp. 2226-34. (Available online)
- Jones, G., Steketee, R., Black R., Zulfiqar, A., Morris, S. & the Bellagio Child Survival Study
Group. 2003, ”˜How many child deaths can we prevent this year?', The Lancet, vol. 362, pp. 65-71. (Available online) - Varley, R. C. G., Tarvid, J. & Chao, D. N. W. 1998, ”˜A reassessment of the cost-effectiveness of water and sanitation interventions in programmes for controlling childhood diarrhoea', Bulletin of the World Health Organization, vol. 76, no. 6, pp. 617-31. (Available online)