Unlimit Health: Supplementary Information
This page contains further discussion and information for our review of Unlimit Health, formerly known as the SCI Foundation, formerly known as the Schistosomiasis Control Initiative. This page is intended to provide supplementary information on topics covered in the main review and is not intended to be read independently of the main review. The information on this page is less frequently updated than our main review; there is a note at the top of each section indicating when it was last updated.
Table of Contents
Descriptions of work in selected countries
Section last updated: November 2016
In 2014, we spoke with four of SCI's program managers to better understand SCI's role in four countries. These conversations were mostly consistent with our general understanding of SCI's work. We selected Côte d'Ivoire, Ethiopia, and Mozambique because SCI has spent significant unrestricted funds, the type of funding GiveWell has recommended, in these countries (more below). SCI selected Uganda as the fourth case study. We have summarized SCI’s work in these countries below.
In addition, in 2015, SCI shared some details about its work in Sudan, where it recently began supporting a program, and in Nigeria, where it is considering supporting a program in the future. We have not yet written up summaries of this work (documents SCI shared are listed in footnote).1
In 2016, we did not attempt to update our understanding of SCI's role in mass drug administration (MDA) programs beyond reviewing spending data.
Côte d'Ivoire
- History: There was no large-scale schistosomiasis treatment program in the country prior to SCI's involvement.2 SCI began working in Côte d'Ivoire in 2010, but mapping and treatments did not begin until 2012 due to political turmoil. It has funded mapping and treatment for all qualifying districts.3 SCI expected to fund about 4.9 million treatments during its 2014-15 budget year;4 it reported delivering 3.1 million treatments in that period.5 During its 2015-16 budget year, SCI planned to deliver around 0.6 million treatments and reported delivering 1.4 million treatments.6 SCI previously told us that it spent a small amount of unrestricted funding in the country prior to 2011; we do not know what this funding was for.7
- Current plans (as of October 2016): SCI plans to deliver 2.4 million treatments in its April 2016 to March 2017 budget year8 and 2.6 million treatments in its April 2017 to March 2018 budget year.9
- Funding: SCI has used the U.K.'s Department for International Development (DFID) funding, a grant from the company Vitol, and unrestricted funding in Côte d'Ivoire.10 In the 2014-15 budget year, SCI spent about $250,000 in restricted funding and $820,000 in unrestricted funding in the country, a significant increase over 2013-14, when SCI spent $580,000 in restricted funding and $20,000 in unrestricted funding.11 In 2015-16, SCI spent around $130,000 in unrestricted funding and around $70,000 in restricted funding in Côte d'Ivoire.12
- Impact of unrestricted funds: SCI told us in 2014 that it believed that availability of unrestricted funds had allowed the program to scale up faster than it otherwise could have.13
- Partners: In the early stages of the program, SCI primarily worked with the Ministry of Health and, for mapping, the Université Félix Houphouët-Boigny. Starting in 2014, SCI began working with other partners, including Sightsavers, the END Fund, and Helen Keller International on a more integrated neglected tropical diseases (NTD) program.14
- Role of SCI staff: SCI's Program Manager for Côte d'Ivoire described her role (as of October 2014) as providing technical expertise, helping create budgets, monitoring training and MDAs, responding to problems (for example, surveying health workers to understand low coverage of non-enrolled children, and advising on how to proceed with the program during a security threat), refining the protocol for the coverage survey, and coordinating with partners for integrated MDAs.15 From November 2013 through November 2014, she traveled to Côte d'Ivoire five times and spent almost four months there in total to assist with and monitor mapping, sentinel site and coverage survey data collection, three MDAs, and budgeting.16 She also noted the role of other SCI staff in the program: the finance team checks receipts against expense reports,17 and the biostatistician analyzes monitoring data and advises government staff on data issues.18
Ethiopia
- History: There was no sustained, large-scale schistosomiasis treatment program in the country prior to SCI's involvement, only a one-off, sub-national treatment.19 SCI began conversations with the government of Ethiopia about starting a national schistosomiasis treatment program in 2012. In 2013, it funded planning for the program. It funded mapping between November 2013 and April 2014, and a first round of treatment in 2013.20 In October 2016, SCI sent us a report on the 2013-14 mapping surveys (and on a second round of mapping in 2015); we have not yet reviewed this report in depth.21 In April 2015, Ethiopia treated a reported 2.9 million children for schistosomiasis and soil-transmitted helminthiasis (STH). SCI conducted a coverage survey following this round of treatment and collected baseline data on infection rates from 22 sentinel schools prior to the treatment round (more on these data collection methods below).22 SCI sent us a report on the baseline sentinel site surveys in October 2016; we have not yet reviewed the report in depth.23 During the remainder of SCI's 2015-16 budget year, SCI reports that an additional 5.3 million children received treatments.24
- Current plans (as of October 2016): SCI plans to deliver schistosomiasis treatments to 6.5 million children (4.5 million of which will also receive STH treatments) in its 2016-17 budget year in Ethiopia,25 and plans to deliver 7.6 million schistosomiasis treatments in its April 2017 to March 2018 budget year.26
- Funding: SCI spent around $2.1 million in unrestricted funding and $0.8 million in restricted funding in Ethiopia between April 2015 and March 2016.27 The END Fund and DFID have now allocated restricted funds for treatment in the country.28
- Impact of unrestricted funds: SCI believes that availability of mapping data significantly improved the chances of securing funding from the END Fund and DFID, and that, at a minimum, the availability of unrestricted funds accelerated the program by a few years.29 Ethiopia's Neglected Tropical Diseases Program Manager told us that the government had not dedicated funding to schistosomiasis and that without SCI's involvement the program would likely not have gone forward. According to him, Ethiopia was not aware of any other potential partners for this work when it began working with SCI.30
- Partners: SCI is funding the Federal Ministry of Health (FMOH) to carry out treatments. It partnered with the Ethiopian Public Health Institute, the technical arm of the FMOH, and the Partnership for Child Development (PCD) on mapping. PCD funded mapping in part of the country and delivered treatments in a pilot program. Deworm the World Initiative is providing technical assistance to the government.31
- Role of SCI staff: SCI's Program Manager for Ethiopia described his role (as of October 2014) as assisting with initial program set up and funder agreements, drafting detailed plans for the next 12 months and general plans for the next 5 years, and providing technical assistance for mapping and some guidance on MDA implementation. At the time, he lived in the country32 and worked closely with the government NTD team.33
Mozambique
- History: There was no large-scale schistosomiasis treatment program in the country prior to the involvement of SCI and Filarial Programmes Support Unit (FPSU; formerly the Centre for Neglected Tropical Diseases) (FPSU). SCI had previously funded a small-scale treatment program in Mozambique with unrestricted funding.34 SCI's grant from DFID, which started in 2010, includes funding for a sub-grant to FPSU to run schistosomiasis treatment programs in three countries, one of which is Mozambique.35 SCI and FPSU decided on this arrangement because SCI believed it would increase the chances of DFID awarding the grant.36 From April 2015 to March 2016, SCI reports delivering 4.4 million treatments, out of a targeted 5.8 million.37
- Current plans (as of October 2016): SCI reports that it plans to deliver 8.8 million treatments in Mozambique between April 2016 and March 201738 and 7.3 million treatments between April 2017 and March 2018.39 SCI told us that one of the rounds of MDA originally scheduled for 2016-17 is now scheduled for 2017-18.40
- Funding: SCI has spent both restricted funding from DFID and unrestricted funding in Mozambique. We believe the information on SCI's spending in Mozambique before the 2015-16 budget year may not be fully accurate (see footnote).41 In its 2015-16 budget year, SCI spent around $0.6 million in restricted funding and no unrestricted funds in Mozambique.42
- Impact of unrestricted funds: SCI told us that unrestricted funds have helped the program scale, but perhaps not as much as it might appear, since SCI has shifted DFID funding to other countries with the expectation of using unrestricted funds in Mozambique.43
- Partners: The Ministry of Health implements the program. SCI/FPSU also collaborate with RTI International, which is working on trachoma in Mozambique and has staff in-country. RTI helps to keep SCI/FPSU informed about program progress.44
- Role of SCI staff: FPSU manages the program day-to-day. SCI has provided some assistance with monitoring and evaluation. We do not have more detail on SCI/FPSU's role in the country.45
Uganda
- History: SCI has worked in Uganda since 2003 and has received funding for this work from each of its large grants: Gates Foundation, USAID, and DFID. There was a gap in SCI's work between the USAID and DFID funding.46 SCI reported that it delivered 23,000 treatments in April 2014 to March 2015.47 It had planned to fund 400,000 treatments this period;48 we haven't discussed with SCI why significantly fewer treatments were delivered than planned. Between April 2015 and March 2016, SCI reports that it delivered 890,000 treatments in Uganda; 1.2 million treatments were planned.49
- Current plans (as of October 2016): SCI plans to deliver 1.1 million treatments in Uganda between April 2016 and March 201750 and 2.0 million treatments between April 2017 and March 2018.51
- Funding: In recent years, SCI has primarily used DFID funding in Uganda (about $280,000 in the fiscal year covering 2013-14, $50,000 in 2014-15, and $380,000 in 2015-16).52 In 2014, SCI allocated a small amount of unrestricted funding to Uganda to increase the number of sentinel sites for operational research purposes.53 SCI also spent about $50,000 in unrestricted funds in Uganda in 2014-15;54 we do not know what these funds were used for. SCI spent around $176,000 in unrestricted funding in Uganda in its 2015-16 budget year, substantially more than previous years.55
- Partners: RTI International, funded by USAID, works in Uganda on an integrated mass NTD treatment program. SCI provides schistosomiasis treatment in those areas where RTI does not.56
- Role of SCI staff: SCI told us that, due to strong in-country capacity, SCI provides only limited technical assistance for MDA. Instead, SCI's technical assistance in the country is focused on operational research on how best to move toward elimination of schistosomiasis.57 SCI's program manager for Uganda describes her role as (as of October 2014) assisting with budgets and plans, talking to the government regularly (largely through email) leading up to an MDA to make sure all the components are prepared, traveling to the country to oversee collection of prevalence and intensity data prior to an MDA, following up with the government after an MDA to get the data needed for reporting to DFID, and participating in activity reviews after each stage of the program (for example, after an MDA and after monitoring and evaluation activities).58
Major funding sources for SCI's work
Section last updated: November 2016
Large grants
SCI's work has historically been driven by a number of large grants, each with somewhat different program designs and geographic coverage. SCI's major grants:
- Initial Gates Foundation grant: SCI was founded in 2002 through a $32 million grant from the Bill and Melinda Gates Foundation.59 This grant was used to create national treatment programs for schistosomiasis and STH in six countries.60
- Grants for integrated NTD control: In 2006, SCI received large grants from USAID and the Gates Foundation to support integrated NTD programs in eight countries for five years to treat lymphatic filariasis, onchocerciasis, and trachoma, in addition to schistosomiasis and STH.61 It received a grant in 2007 to expand its work to Rwanda and Burundi.62 All of these grants were completed in 2011.63
- DFID grants: In 2010, SCI received £10.5 million64 (plus separate funding for drugs) from DFID for treating schistosomiasis and STH65 in eight countries over five years.66 Other NTDs are not covered by the grant, though DFID also provided funding to the FPSU to integrate treatment for lymphatic filariasis with SCI-funded schistosomiasis and STH programs in six countries.67 In 2014, DFID awarded SCI an additional £16.6 million over four and a half years (June 2014 to December 2018) to extend the program and expand it to an additional two countries.68
Unrestricted funding
Prior to 2011, unrestricted funds accounted for a very small portion of SCI's total funding.69 SCI told us that this funding was primarily used to fund treatments in regions of Côte d'Ivoire and Mozambique.70
In part due to GiveWell's recommendation, since November 2011, SCI has received significantly more unrestricted funds: through September 2016, GiveWell had tracked about $14.6 million in donations to SCI due to our research.71 We estimate that around 63% of the unrestricted funds that SCI raised in April 2013 to March 2016 (the period for which we have seen data) were due to GiveWell's recommendation.72
Unrestricted funds now make up a large portion of SCI's revenue. For April 2015 to March 2016, SCI reports that 48% of its revenue was unrestricted.73
Additional academic evidence
Section last updated: November 2016
To provide additional information on SCI's track record, in 2014, we conducted a search for published papers on treatment coverage rates and schistosomiasis and STH prevalence and intensity in countries where SCI has worked. (We revisited this project in 2016 to review a recent paper from Melissa Parker and Tim Allen [Allen and Parker 2016]; we have not yet written up our conclusions. In short, our work in 2016 is largely consistent with the conclusions presented below.)
In 2014, we focused on papers by Melissa Parker and Tim Allen, who were funded by the Bill and Melinda Gates Foundation to provide an anthropological perspective on SCI's work,74 papers cited in papers by Melissa Parker and Tim Allen, and other papers we identified on this topic from a Google Scholar search.75
The papers we identified were all from Tanzania, Uganda, and Zanzibar, perhaps because these are places that Melissa Parker and Tim Allen's work has focused on.
This spreadsheet summarizes the papers we considered. We have not fully vetted these studies. The studies were generally designed for purposes other than to evaluate SCI's programs, so in many cases there is uncertainty about SCI's role in the areas studied. In the discussion below, we have excluded studies that we do not believe were conducted soon after treatment programs in areas targeted by SCI-funded programs. SCI staff and/or SCI funding were involved in many of the studies.76
It is difficult to draw any conclusions from these studies because of small sample sizes and lack of clarity on SCI's role in each location. In summary:77
- Tanzania (excluding Zanzibar): Two studies at the district level, Stothard et al. 2013 and Chaula and Tarimo 2014, show relatively low schistosomiasis prevalence after treatment (4% and 15% respectively; the latter claims that prevalence pre-MDA was 30%). SCI was working in Tanzania at the time of both studies, but it is not clear if SCI was working in the specific areas studied. Chaula and Tarimo 2014 also shows low treatment coverage (around 40%), though the researchers asked in 2013 about treatment provided in 2011 and 2012.
- Zanzibar: All studies were conducted on Unguja, "the largest and most populated island of Zanzibar."78 Two studies, Stothard et al. 2009 and Rudge et al. 2008, each in a single school, found high prevalence of schistosomiasis in areas that had received treatment (65% and 50% prevalence, respectively). However, the sample sizes were small, it is not clear why these particular schools were selected, and, while SCI was working in Zanzibar at the time of both studies, it is not clear if SCI was working in the specific areas studied. Another study, Knopp et al. 2009, in two schools in an area that had received treatment (but perhaps not from SCI) found moderate prevalence of various STHs (e.g., 22% prevalence for hookworm and low infection intensity). The schools were selected because they had been surveyed in 1994, when prevalence was found to be much higher.
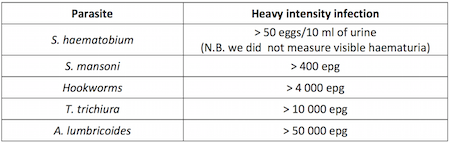
- Uganda: We reviewed three studies of schistosomiasis prevalence. Muhumuza et al. 2013 was conducted in part of a district that seems to have received several rounds of treatment (but perhaps not from SCI). Brooker et al. 2005 was conducted across a district that had its first MDA the year before, which was funded by SCI. Standley et al. 2009 was conducted across six districts: one district that had never been treated (but from which only one school, which had low prevalence, was included in the analysis), two districts that seem to have been treated only once, and three districts that seem to have been treated for many years by SCI. Standley et al. 2009 explicitly aimed to "ambush" schools that might not have been reached by treatment programs.79 Each study found moderate to high prevalence of schistosomiasis (Muhumuza et al. 2013: 35%, Brooker et al. 2005: 26%, and Standley et al. 2009: 42%). Muhumuza et al. 2013 and Standley et al. 2009 found fairly high infection intensity (116 and 634 average eggs per gram respectively among positive cases; the WHO threshold for "high intensity" is 400 eggs per gram80 ). Muhumuza et al. 2013 found 28% coverage in the most recent round of treatment. The coverage survey in Muhumuza et al. 2013 seems to have been six months after treatment.
All sources for SCI review
Section last updated: November 2016
{kind=link}
- 1
Sudan
- Sudan NTD concept paper (2015-2018)
- Sudan PZQ and ALB treatments by locality (2015)
- Sudan annual workplan (April 2015 to March 2016)
- Sudan cash book
- Sudan campaign photos
- Sudan annual workplan for WHO (2015)
- Sudan joint request for selected PC medicines
Nigeria
- 2
"Prior to SCI’s work in Côte d'Ivoire, there were no large-scale schistosomiasis (SCH) treatment programs." GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014.
- 3
"SCI first contacted the government and started to discuss a SCH/STH program in 2010. A civil war delayed progress because there was political turmoil, a weakened health system, and dangerous conditions. In 2012 conditions improved, and the contracts between SCI and the Ministry of Health were set up. [...]
Treatments started in December 2012:- In 2012: 649,859 school-aged children (SAC) received treatments in 12 districts, some of which had been mapped prior to SCI’s involvement.
- In November 2013: 853,708 SAC received treatments in the areas that SCI mapped first, with the help of the Ministry of Health.
- In May 2014: 1,425,461 SAC received treatment in the remaining areas of the first phase of mapping.
- In November 2014: 3.5 million SAC are targeted for the next treatment, which would correspond to the second phase of mapping.
The aim is that by the end of 2014, all SAC in the SCH-endemic districts will have been treated at least once. Some areas that were treated in 2012 were also treated again in May." GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014.
- 4
"In May 2014: 1,425,461 SAC received treatment in the remaining areas of the first phase of mapping. In November 2014: 3.5 million SAC are targeted for the next treatment, which would correspond to the second phase of mapping." GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014.
- 5
Alan Fenwick, email to GiveWell, November 3, 2015. Note this is slightly higher than we previously reported in our August 2015 update on SCI.
- 6
- SCI treatment data 2014-16, cell E5.
- SCI Global treatment numbers 2015-16, cell C7.
- 7
"For the smaller donor, we have two or three projects, which we have been supporting and which will hopefully lead to pilot projects in their respective countries.
- In Côte d'Ivoire, we now have funding from the U.K. Department for International Development (DFID). There will eventually be a national program.
- In Mozambique, we have a doctor running a practice for 70,000 people. We have been funding her to test people, do surveys and give drugs to treat people. Up until now, that has taken all the individual funding that comes in."
Alan Fenwick, SCI Director, phone conversation with GiveWell, February 16, 2011.
- 8
SCI allocation table 2016-2017, "Implementation" sheet, cell B6.
- 9
SCI budget 3 options October 2016 Redacted, "Implementation" sheet, cell B5.
- 10
- Vitol: Côte d'Ivoire mapping; £102,152; grant period: 01/10/2012 to 31/12/2013. (pg. 3). SCI advisory board financial report (June 2014).
- DFID ICOSA £177,000 in 2013-14. SCI advisory board financial report (June 2013).
- DFID ICOSA: £200,000 in year 5 of the grant (pg. 9). (The grant is "A six year contract from October 2010 to March 2016," (pg. 7) and DFID's fiscal year is from April 1 to March (DFID glossary), so year 5 is April 2014 to March 2015.) SCI advisory board financial report (June 2014).
- SCI has reported $525,264 in spending in Côte d'Ivoire from unrestricted funds between November 2011 and September 2014. GiveWell summary of SCI finances (October 2014), Sheet Combined with previous updates.
As of November 4, 2014, Google states that £1 is worth $1.6.
- 11
- SCI financial statement 2013/14 and 2014/15 (revised October 2015)
- Note that SCI told us, "SCI used unrestricted funds to conduct a community health questionnaire in areas with low coverage. [...] This questionnaire was the main use of unrestricted funding in Cote d’Ivoire in 2014." GiveWell's non-verbatim summary of a conversation with Alan Fenwick and Najwa Al Abdallah, September 14, 2015.
- 12
GiveWell's analysis of SCI budget vs. actuals 2015-16 Redacted, "BVA in USD" sheet, cells I11 and K11.
- 13
"If the 2014 targets are met, it will be an impressive achievement to have treated all SCH-endemic areas at least once since 2012. With just the funding allocated by DFID, the program could not have scaled up as quickly. In this scenario, it probably would have completed the mapping but delivered fewer treatments." GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014.
- 14
- "SCI conducted national mapping since late 2012, finishing in March 2014. In total, all 82 districts in Côte d'Ivoire were mapped. This was done in two phases because of limited funding. The first phase was done by the Ministry of Health with support from SCI. The second phase was led by Professor Eliézer N’Goran from the Université Félix Houphouët-Boigny with both technical and financial support from SCI. […]
The country will start an integrated treatment program for several diseases in November 2014 […]
Other neglected tropical disease (NTD) organizations have benefitted from the work SCI has done to build a SCH program. SCI has provided cars and developed staff capacity. Organizations have worked to coordinate when sharing these resources and operating an integrated program should make that easier." GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014. - "Cote d’Ivoire is working toward creating an integrated program for the treatment of lymphatic filariasis, onchocerciasis, schistosomiasis, and STH. This will involve collaboration and integration of tools and training, but drugs for all four diseases will not be administered simultaneously. So far, lymphatic filariasis and onchocerciasis treatments have been integrated, and schistosomiasis and STH treatments are administered together but currently delivered separately from lymphatic filariasis and onchocerciasis. [...] SCI's partners in Cote d'Ivoire include Sightsavers, the END Fund, and Helen Keller International." GiveWell's non-verbatim summary of a conversation with Alan Fenwick and Najwa Al Abdallah, September 14, 2015.
- "SCI conducted national mapping since late 2012, finishing in March 2014. In total, all 82 districts in Côte d'Ivoire were mapped. This was done in two phases because of limited funding. The first phase was done by the Ministry of Health with support from SCI. The second phase was led by Professor Eliézer N’Goran from the Université Félix Houphouët-Boigny with both technical and financial support from SCI. […]
- 15
GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014.
- 16
"Dr. Nogaro has visited Côte d'Ivoire several times over the last year, often dealing with multiple activities on each trip:
- One month last November to oversee the sentinel sites activity and obtain baseline information for both prevalence and intensity of infection, help with the MDA, and oversee the start of the second phase of mapping,
- One month in January to work on the coverage survey, work on financial reporting, oversee mapping, and help with drafting the annual work plan and budget (alongside the Ministry of Health),
- Three weeks in May for another MDA,
- One week in June to work with WHO and other partners for the integrated MDA plan and budget work, and
- Three weeks this month to follow up with CHWs in low coverage areas, oversee the sentinel sites activity, and oversee the first integrated MDA and training."
GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014.
- 17
"Program staff in each country create annual budgets in collaboration with SCI. The budget ensures money is being spent well and on activities defined in the annual work plan, which is submitted by the country to SCI. Generally, receipts are used to document expenses. In some cases, it takes a long time to get the receipts or receipts are not available at all. SCI hired an accountant and an auditor to better monitor finances." GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014.
- 18
"Data is entered at the country level. For example, data from mapping and sentinel sites can be handled by students at a local university. The data is double entered to ensure accuracy. The original forms stay in the country and the database is sent to SCI, which can then run analyses. SCI is planning to expand its data analysis team. In the spring, SCI’s biostatistician will teach a data cleaning session to program staff in Côte d'Ivoire. In the future, SCI will consider doing more advanced data analysis training in all the countries it supports." GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014.
- 19
"In 2007, prior to SCI’s involvement, Save the Children ran a one-time treatment for about 1 million children for schistosomiasis (SCH) and soil-transmitted helminths (STH)." GiveWell's non-verbatim summary of a conversation with Michael French, October 15, 2014.
- 20
"In mid-2012, the University of Gondar invited SCI to an international symposium on SCH, which served as an introduction for SCI to Ethiopia. After this, Dr. Fenwick, Director of SCI, and other senior SCI staff established a relationship with senior Federal Ministry of Health (FMOH) officials.
In 2013, SCI moved into more serious conversations with the Ministry of Health. In July 2013 SCI provided support for the launch of the FMOH’s National NTD Master Plan at an international symposium in Addis Ababa. Around the same time, SCI collaborated with the Ethiopian Health and Nutrition Research Institute (EHNRI; now renamed as the Ethiopian Public Health Institute), the technical arm of the FMOH, to plan and fund nationwide mapping. […]
Last year (2013) SCI funded 1.4 million combined SCH/STH treatments. […]
The mapping took longer than planned. Teams were trained in November 2013, and the mapping was completed in April 2014." GiveWell's non-verbatim summary of a conversation with Michael French, October 15, 2014. - 21
SCI Ethiopia mapping surveys 2013-15
- 22
SCI Ethiopia treatment campaign summary report (April 2015).
- "In total 2.9 million school-aged children received treatment against both schistosomiasis and STH (coverage of 74.0%), comprised of 2.3m enrolled SAC and 571,000 non-enrolled. These numbers are currently being validated using coverage validation surveys in representative districts. These results will be presented as soon as the data is analysed." pg. 1.
- "Demographic and parasitological data were collected from 22 sentinel sites prior to the April 2015 campaign. Each sentinel site comprised of a school, with 125 children recruited from each school. Each child provided stool and urine samples on two consecutive days in order to estimate the level of parasite prevalence and average intensity of infection. These 22 sentinel sites will be supplemented by a further 15 sites prior to the October 2015 round of treatment to complete the picture on the baseline level of infection. These schools will be followed up annually, just prior to treatment, to understand changes in infection across the course of the programme." pg. 4.
- 23
SCI Ethiopia impact survey baseline report 2015-16
- 24
- ~8.2 million total treatments in Ethiopia between April 2015 and March 2016. SCI Global treatment numbers 2015-16, cell C9.
- ~8.2 million minus 2.9 million equals ~5.3 million
- 25
- SCI Ethiopia annual treatments 2016, Cells H9:J9.
- The figure reported in SCI allocation table 2016-2017, "Implementation" sheet is 13.2 million, the total number of children expected to receive schistosomiasis and/or soil-transmitted helminthiasis treatments.
- 26
SCI budget 3 options October 2016 Redacted, "Implementation" sheet, cell B7.
- 27
- GiveWell's analysis of SCI budget vs. actuals 2015-16 Redacted, "BVA in USD" sheet, cells I13 and K13.
- We discuss SCI's work in Ethiopia in our November 2012, October 2013, and June 2014 updates on SCI.
- 28
Alan Fenwick, email to GiveWell, September 28, 2015. First transfers from END Fund and DFID funds occurred in 2015. Also:
- "Getting sufficient funding from SCI this year was straightforward because it was primarily restricted funding from the END Fund. The first year of this 3-year grant ends in February 2015." GiveWell's non-verbatim summary of a conversation with Michael French, October 15, 2014.
- We note in our June 2014 update on SCI that, as of April 2014, SCI was in the final stages of negotiating the grant from DFID that includes funding for Ethiopia.
- 29
"He does not know if The END Fund/DFID would have gotten involved without the mapping data. At a minimum, the mapping effort significantly increased the probability of attracting external funding and accelerated the program by a few years." GiveWell's non-verbatim summary of a conversation with Michael French, October 15, 2014.
- 30
"FMOH [Federal Ministry of Health] began working with SCI about 2.5 years ago. Mr. Shafi's predecessor began speaking to SCI about the possibility of working together on a schistosomiasis program. SCI was the only organization that the government spoke to about this, as it wasn't aware of any other organizations working on schistosomiasis. [...]
Without SCI's involvement, the program would likely not have gone forward. With the exception of filling small funding gaps on an ad hoc basis, the government has not been able to allocate funding to NTDs. It was interested in doing disease mapping but did not have the funding to do so, and it likely would not have received drug donations without the mapping data." GiveWell's non-verbatim summary of a conversation with Oumer Shafi, November 4, 2014. - 31
"In July 2013 SCI provided support for the launch of the FMOH’s National NTD Master Plan at an international symposium in Addis Ababa. Around the same time, SCI collaborated with the Ethiopian Health and Nutrition Research Institute (EHNRI; now renamed as the Ethiopian Public Health Institute), the technical arm of the FMOH, to plan and fund nationwide mapping. […]
The Deworm the World Initiative (DtWI) will be providing technical advice to Ethiopia, based on its experience in Kenya. […]
With funding from Dubai Cares, the Partnership for Child Development (PCD) implemented a small pilot program in 30 schools in the southern region (SNNPR) to look at feasibility of a comprehensive school health and nutrition program, which includes deworming, nutrition, and WASH [water, sanitation, and hygiene] interventions and home-grown school-feeding. Related to this, the grant included funding for a region-wide situational analysis, covering an area with about 17 million people. Therefore, the decision for this to be included in the broader national mapping and to include the distribution of SCH, STH, WASH facilities, and school-feeding needs. SCI and PCD partnered on the design, implementation, and analysis of this national mapping. Overall, PCD provided both technical assistance and about 20%-25% of the funding for the national mapping." GiveWell's non-verbatim summary of a conversation with Michael French, October 15, 2014. - 32
"Examples of Dr. French's work to assist the Ethiopia program:
- Initial program setup activities: creating processes and scheduling meetings to lay groundwork for future activities; developing and finalizing contracts between funders, Imperial Collage [sic] and implementers (the contracts are more complicated than normal because there are 2 funders and 2 implementing agencies).
- SCH/STH action plan: This will provide a detailed plan for next 12 months and more general plan for 5 years. The FMOH have tasked Dr. French and SCI to drive this this forward, e.g providing an outline that can be adapted by the country.
- Mapping plan: Dr. French was the main technical advisor from SCI. He worked very closely with people from EHNRI to a) write the research protocol, b) advise on the recruitment of trainers, and c) train technicians, d) supervise activities, e) help with data collection and analysis.
- Last year’s mass drug administration (MDA): Dr. French was less involved with the MDA than with the mapping but was involved in developing the plans. The Ministry of Health was responsible for running the program and delegating work to regional governments. It had experience from other mass distribution programs. For technical training, it worked with health workers who already had extensive general experience and then provided NTD expertise largely from WHO guidelines, though SCI provided some technical guidance.
Dr. French has been living in Ethiopia, which has helped him build relationships, enabled him to hear more activity details, and allowed him to provide timely advice. For example, he has stronger relationships with the officials in Ethiopia and a clearer sense of whom to go to for various requests. Also, by being close to the activities, some problems with data flowing back to central level have been clearer, which makes it easier for him to help develop solutions." GiveWell's non-verbatim summary of a conversation with Michael French, October 15, 2014.
- 33
"Mike French, SCI's program manager for Ethiopia, works in the same office as the government NTD program." GiveWell's non-verbatim summary of a conversation with Oumer Shafi, November 4, 2014. In June 2016 when we sent a draft of this review to SCI, SCI edited this to "works closely with."
- 34
"Prior to SCI’s involvement in 2010, there was a mapping project in 2008. Dr. Blair does not think there were any schistosomiasis (SCH) treatment programs (other than a small program funded by SCI). If there were, they would have been small-scale." GiveWell's non-verbatim summary of a conversation with Lynsey Blair, October 16, 2014.
- 35
"The SCH program in Mozambique is run by the Center for Neglected Tropical Diseases (CNTD). Funding for the program is provided to SCI by DFID, and SCI funds CNTD as part of its agreement with DFID." GiveWell's non-verbatim summary of a conversation with Lynsey Blair, October 16, 2014.
- 36
“When we bid for the DFID grant, I was advised that DFID favored grants that involved partnerships. CNTD does a lot of the work on lymphatic filariasis. DFID was providing 20 million pounds for lymphatic filariasis and 20 million for schistosomiasis. Working with CNTD demonstrated a degree of integration. CNTD does both lymphatic filariasis and schistosomiasis in Mozambique." Alan Fenwick, SCI Director, conversation with GiveWell, October 14, 2014.
- 37
SCI treatment data 2014-16, cells E12:F12.
- 38
- SCI allocation table 2016-2017, "Implementation" sheet, cell B13.
- In September 2016, SCI told us that it now planned to deliver an additional 3 million treatments beyond the amount it had originally planned at the start of the budget year. Najwa Al Abdallah, Dr. Lynsey Blair, and Dr. Wendy Harrison, conversation with GiveWell, September 27, 2016
- 39
SCI budget 3 options October 2016 Redacted, "Implementation" sheet, cell B12.
- 40
Dr. Wendy Harrison, Najwa Al Abdallah, and Dr. Lynsey Blair, conversation with GiveWell, April 6, 2016
- 41
- DFID funds:
- DFID ICOSA £649,514 in 2013-14. SCI advisory board financial report (June 2013), pg. 7, “Overseas country budgets - FY4.”
- DFID ICOSA: £150,000 in year 5 of the grant (pg. 9). (The grant is "A six year contract from October 2010 to March 2016," (pg. 7) and DFID's fiscal year is from April 1 to March, so year 5 is April 2014 to March 2015.) SCI advisory board financial report (June 2014), pg. 9.
- Unrestricted funds:
- SCI draft financial statements for 2013/14 and 2014/15 reported that the unrestricted funds SCI spent in Mozambique summed to £595,421 in 2013-14 and £596,588 in 2014-15. SCI later told us that this document may not be accurate. SCI responses to GiveWell questions on financial statements (October 2015).
- DFID funds:
- 42
SCI did not spend any unrestricted funding on the program in Mozambique in its 2015-2016 budget year and spent $573,281 in restricted funding. GiveWell's analysis of SCI budget vs. actuals 2015-16 Redacted, "BVA in USD" sheet, cells I18:K18.
- 43
See our June 2014 update on SCI.
- 44
"SCI and CNTD are working closely with RTI International in Mozambique. This has been a great working relationship. RTI is funding some capacity development around drug logistics. It is working on trachoma; currently, this work is focused on mapping, but it will likely fund treatment when mapping is finished. RTI has staff in-country and reports to SCI and CNTD on issues, which can provide some verification that the program is progressing as expected. The organizations coordinate to ensure multiple sources of funding aren't allocated for the same purpose. For example, RTI emailed SCI and CNTD saying that the government had indicated that it was going to drop the SCH program; the staff from the organizations communicated quickly to sort out the confusion." GiveWell's non-verbatim summary of a conversation with Lynsey Blair, October 16, 2014.
- 45
"The SCH program in Mozambique is run by the Center for Neglected Tropical Diseases (CNTD). Funding for the program is provided to SCI by DFID, and SCI funds CNTD as part of its agreement with DFID. [...] CNTD will continue to run the mass drug administration (MDA), but SCI has become more directly involved with the M&E as it has the technical expertise to manage these activities." GiveWell's non-verbatim summary of a conversation with Lynsey Blair, October 16, 2014.
- 46
"SCI’s program in Uganda is fully funded by DFID (other than one use of unrestricted funding, discussed below). SCI had previously worked in Uganda with funding from the Bill & Melinda Gates Foundation. After this funding ended, USAID funded work by RTI International in Uganda. Around 2006, Uganda started an integrated NTD program in districts endemic with more than one NTD. Districts with only schistosomiasis (SCH) were not treated.
When SCI re-entered Uganda, it started SCH programs in the districts not receiving treatment." GiveWell's non-verbatim summary of a conversation with Yolisa Nalule, October 14, 2014. - 47
See our August 2015 update on SCI.
- 48
SCI report to GiveWell (September 2014), Annex 1.
- 49
SCI treatment data 2014-16, cells E18:F18.
- 50
SCI allocation table 2016-2017, "Implementation" sheet, cell B20.
- 51
SCI budget 3 options October 2016 Redacted, "Implementation" sheet, cell B19.
- 52
- SCI spent 176,060 GBP in restricted funding in 2013/14 and 29,831 GBP in 2104/15. SCI draft financial statements for 2013/14 and 2014/15.
- As of November 4, 2014, Google states that £1 is worth $1.6.
- 176,060 * 1.6 = $281,696
- 29,831 * 1.6 = $47,730.
- GiveWell's analysis of SCI budget vs. actuals 2015-16 Redacted, "BVA in USD" sheet, cell I25.
- 53
"SCI’s program in Uganda is fully funded by DFID (other than one use of unrestricted funding, discussed below)...
In deciding on the budget, there might be some disagreement around whether impact M&E (having sentinel sites) is worth the expense. The government might prefer to provide more treatments. Mrs. Nalule and other researchers argue for the value of M&E.
Last year, M&E funding was augmented by £23,000 from SCI unrestricted funding. Without this, there likely would have been cuts in the number of sentinel schools. This M&E is enabling research to compare different treatment strategies in areas where prevalence is low. DFID was not interested in funding this research." GiveWell's non-verbatim summary of a conversation with Yolisa Nalule, October 14, 2014.
Note that SCI has only reported $2,220 in unrestricted spending to us in financial reports. GiveWell summary of SCI finances (October 2014), Sheet Combined with previous updates. - 54
- SCI draft financial statements for 2013/14 and 2014/15
- As of November 4, 2014, Google states that £1 is worth $1.6.
- 29,914 * 1.6 = $47,862.
- 55
GiveWell's analysis of SCI budget vs. actuals 2015-16 Redacted, "BVA in USD" sheet, cell K25.
- 56
"When SCI re-entered Uganda, it started SCH programs in the districts not receiving treatment. Also, in about 30 districts, USAID stopped treating SCH because prevalence dropped below 20%, so SCI supported the continuation of these treatments with an aim towards elimination. […]
Also, SCI is taking over treatment from RTI in a 15 districts that have higher prevalence, and, in these districts, it will treat adults. Since prevalence is over 50%, WHO guidelines say to treat children and high risk adults (e.g. fisherman), though usually programs will just try to treat all adults." GiveWell's non-verbatim summary of a conversation with Yolisa Nalule, October 14, 2014. - 57
"In some cases (for example, Uganda and Niger), the government program manager understands SCH well and does not require a lot of technical guidance. [...] Uganda is an interesting example. The program had been relatively straightforward to manage. It is now focusing on elimination, which is unknown territory so will require much more guidance. There is a lot of research to do to determine guidelines for how often to treat." GiveWell's non-verbatim summary of a conversation with Lynsey Blair, October 16, 2014.
- 58
GiveWell's non-verbatim summary of a conversation with Yolisa Nalule, October 14, 2014.
- 59
"The move towards national control programmes in sub-Saharan Africa was facilitated by an award from the Bill and Melinda Gates Foundation (BMGF; http://www.gatesfoundation.org) Global Health Program in 2002, to the SCI for the implementation and evaluation of control of schistosomiasis." Fenwick et al. 2009, pg. 2. Amount at Gates Foundation, Imperial College London (June 2002).
- 60
"Six countries were selected by October 2003 for full support: Burkina Faso, Mali, Niger, Uganda, Tanzania and Zambia. The countries each proposed a different implementation approach and management structure for their large-scale schistosomiasis control. This was readily accepted because the BMGF required SCI to test the ‘proof-of-principle’ of national scale, Ministry of Health (MoH)-led schistosomiasis control programmes. SCI is based in Imperial College London and operated with the principle that all programmes were country owned and run, with SCI staff offering technical and other assistance, but not as expatriates living in-country. Programmes were based in the MoH in the respective country, and SCI offered support to improve the national health system." Fenwick et al. 2009, pg. 2.
Between 2003 and 2008, SCI provided treatment for schistosomiasis and soil-transmitted helminthiasis to the following number of people (Fenwick et al. 2009, pg. 3, Table 1).
Number treated by country (millions) Year Uganda Burkina Faso Niger Mali Tanzania Zambia 2003 0.43 - - - 0.10 - 2004 1.23 1.03 0.67 - 0.44 - 2005 2.99 2.30 2.01 2.60 2.95 - 2006 1.51 2.82 1.56 2.18 0.38 0.56 2007 1.81 0.75 2.07 0.65 2.65 0.25 2008 1.50 2.70 5.28 - 1.24 - - 61
- "Current and future rounds of treatment in all six countries are being delivered in an integrated manner to include schistosomiasis, STH, lymphatic filariasis, onchocerciasis and trachoma." Fenwick et al. 2009, pg. 10.
- The "six countries" refers to the six countries funded by SCI's first Gates Foundation grant.
- Countries and dates from SCI Board management accounts (April 2010)
- 62
SCI Burundi: Impact
SCI Rwanda: Strategy
SCI Board management accounts (April 2010) - 63
- 64
- 65
"A team from Imperial College London has been awarded £25 million funding from the UK Government to continue its fight against neglected tropical diseases, it was announced this week. The money will enable the Schistosomiasis Control Initiative (SCI) to provide 75 million treatments to protect some of the world’s poorest children against schistosomiasis – an illness caused by parasitic worms – and soil-transmitted helminths (STH). £15 million of the funding will be spent directly on procuring drug treatments, through an organisation called Crown Agents. The rest will be administered by SCI." SCI Imperial initiative to protect children from tropical disease awarded ₤25m government backing.
- 66
”DFID has allocated 50 million GBP for control of neglected tropical diseases over 5 years, of which £25 million is going through SCI for schistosomiasis control in 8 countries (including Malawi) over five years.” GiveWell's notes from visit to Malawi on October 17-19, 2011, pg. 1.
- 67
"SCI will be assisted in their drug delivery by the Centre for Neglected Tropical Diseases at Liverpool School of Tropical Medicine via a sub contract through LATH (Liverpool Associates in Tropical Health). In six countries, this will lead to treatment for lymphatic filariasis – another worm disease – becoming integrated with schistosomiasis and STH treatment." SCI Imperial initiative to protect children from tropical disease awarded ₤25m government backing.
- 68
- 69
- As of July 2011, it had received about $580,000 in unrestricted funding (SCI IC Trust summary (September 2011), "2010-2011" sheet, cell K14) and $108 million overall (SCI Gates Foundation final report (January 2011) Pg. 20).
- As of July 1, 2011, Google states that £1 is worth about $1.607.
- £361,061 * 1.607 = $580,225
- 70
"For the smaller donor, we have two or three projects, which we have been supporting and which will hopefully lead to pilot project in their respective countries.
- In Côte d'Ivoire, we now have funding from the U.K. Department for International Development (DFID). There will eventually be a national program.
- In Mozambique, we have a doctor running a practice for 70,000 people. We have been funding her to test people, do surveys and give drugs to treat people. Up until now, that has taken all the individual funding that comes in."
Alan Fenwick, SCI Director, phone conversation with GiveWell, February 16, 2011.
- 71
Donations to SCI due to GiveWell's research through January 2016 are listed here and total about $14.2 million. GiveWell tracked an additional $400k to SCI between February and September 2016 (internal data).
- 72
- We estimate that SCI received about $11.2 million due to GiveWell's recommendation between April 2013 and March 2016 (internal data). Over that period, SCI reports $17.8 million in unrestricted revenue. SCI's total for April 2013 to March 2015 may include some restricted funds. More details here.
- March 2013 to April 2015 SCI unrestricted funding, $12.4 million: SCI financial statement 2013/14 and 2014/15 (revised October 2015) ($4,591,396 + $7,828,759 = $12,420,155).
- Between April 2015 and March 2016, we estimate that SCI received around $5.4 million in total unrestricted revenue. Internal calculations based on:
- SCI L-account 2016
- SCI IC Trust statement July 2016 Redacted
- $12.4 million plus $5.4 million is $17.8 million. $11.2 million / $17.8 million = 63%
- 73
SCI allocation table 2016-2017, "Income analysis" sheet:
- Unrestricted funding total: Income balance at IC Trust at 31 March 2016 (2,133,898 GBP) plus Income balance at L-account at 31 March 2016 (3,428,676 GBP) = 5,562,574 GBP. Cells B2 and B3.
- Restricted funding total: "Committed from DFID" (4,285,439 GBP) plus "Committed from UBS" (257,753 GBP) plus "Committed from CIFF' (261,645 GBP) plus "Committed from END Fund" (908,860 GBP) plus "Committed from Score" (95,000 GBP) plus "Committed from Gates" (79,105 GBP) plus "Committed from MRC" (45,461 GBP) = 5,933,263 GBP. Cells B5:B11.
- 5,562,574 /(5,562,574 + 5,933,263) = 48%
- 74
"The research summarised in this paper is based upon field-work funded by the Schistosomiasis Control Initiative (SCI), Imperial College, under the auspices of the Bill and Melinda Gates Foundation. [...] We are grateful to Professor Alan Fenwick, director of SCI, for his unfailing support, and his encouragement of our work, even when our findings made uncomfortable reading. We are also grateful to other staff from SCI, some of whom have disagreed with our analysis, but who have continued to provide assistance, including Lynsey Blair, Fiona Fleming and Artemis Koukounari." Allen and Parker 2011, pg. 114.
- 75
We examined the references from Parker, Allen, and Hastings 2007, Allen and Parker 2011, Parker and Allen 2011, Allen and Parker 2012, and Parker and Allen 2014, Muhumuza et al. 2013 and Standley et al. 2009. We searched on Google Scholar for "niger schistosomiasis prevalence," “niger deworming uptake," "niger praziquantel uptake," "Burundi schistosomiasis prevalence," "Burundi deworming uptake," "Burundi praziquantel uptake," "schistosomiasis prevalence Africa," "deworming uptake Africa," "praziquantel coverage Africa," "Uganda schistosomiasis prevalence," and "Uganda praziquantel uptake."
- 76
For example:- SCI Director Alan Fenwick and SCI-affiliated researcher Narcis Kabatereine were coauthors on Brooker et al. 2005 and Standley et al. 2010.
- Narcis Kabatereine, SCI Africa Capacity Building Adviser, was a co-author on Standley et al. 2009.
- Lynsey Blair, SCI Senior Project Manager, was a coauthor on Stothard et al. 2013.
- Knopp et al. 2009 was funded in part by SCI: "Financial support: This study received funding from the Swiss National Science Foundation (projects PPOOB–102883 and PPOOB– 119129), the Natural History Museum (supported through The Health Foundation,United Kingdom),the World Health Organization (OD/TS- 07-00331), the European Union (FP6 STREP CONTRAST project, contract 032203), and the Schistosomiasis Control Initiative." pg. 1077.
- 77
See the spreadsheet for details and citations.
- 78
Wikipedia entry for Unguja - 79
"The study was designed specifically to target schools on an ad hoc basis as an 'ambush' strategy, to prevent visiting only schools which are commonly surveyed or well-known by local health officers. By doing so, some of the more overlooked schools may have been sampled here, which correspondingly had lower incidences of treatment, irrespective of their prevalence levels." Standley et al. 2009, pg. 50.
- 80
SCI Côte d'Ivoire panel study baseline report, pg. 7.
- We estimate that SCI received about $11.2 million due to GiveWell's recommendation between April 2013 and March 2016 (internal data). Over that period, SCI reports $17.8 million in unrestricted revenue. SCI's total for April 2013 to March 2015 may include some restricted funds. More details here.