This page lists major causes of death (and extreme debilitation) that affect developing countries far more than wealthier countries. For each, we give a brief overview of the problem and its magnitude, then list methods we are aware of for fighting this problem and improving people's lives. We summarize the major causes of death in sub-Saharan Africa on our life expectancy page.
In constructing this page, we drew heavily on the World Bank's Disease Control Priorities Project (DCPP).
Table of Contents
Malaria
Malaria, a parasite-transmitted disease that can cause fever and in some cases death, is one of the most common causes of death in children under the age of 5 living in sub-Saharan Africa. (It largely does not affect older people: those who survive to adulthood generally build up immunity to the disease, and any malaria infection is asymptomatic - see Source 4).
- In 2001, malaria killed almost 1 million children out of a total population of 113 million (Source 1), implying an 0.88% mortality rate for children.
- The Rwandan Ministry of Health estimates that sub-Saharan Africa accounts for 90% of the 300 million annual cases of malaria, and there approximately 115 million children under 5 living in sub-Saharan Africa (Source 1), implying that each child in sub-Saharan Africa has 2-3 episodes of malaria each year (Source 2).
- The DCPP estimates the number of cases per year in Africa slightly higher, at 365 million (Source 3). Malaria can not only be fatal, but can also cause debilitation including cerebral palsy, mental retardation, blindness, and deafness (Source 5), though we don't know how often malaria leads to each of these things.
- We roughly estimate that 0.3%-0.5% of all malaria cases in children under-5 are fatal. (This is a simple mathematical estimate based on the two numbers above: 2-3 cases per year, and 0.88% chance of dying from malaria in a year.)
Sources:
- Source 1: Deaths by Cause, Sex, and Age in the Sub-Saharan Africa Region, 2001 (thousands)
- Source 2: Rwandan National Health Accounts, 2003
- Source 3: DCPP, Conquering Malaria: Population at Risk for Falciparum Malaria, Cases and Attack Rates by World Health Organization Region, 2002
- Source 4: DCPP, Conquering Malaria: Causes, Epidemiology, Manifestations, and Diagnosis
- Source 5: DCPP, Conquering Malaria: Burden of Disease
Insecticide treated nets (ITNs)
Long-lasting insecticide treated bednets (ITNs) are the accepted means for preventing deaths from malaria, according to a position statement from the World Health Organization. The net serves as a "fence" to keep mosquitoes away from the person sleeping, and the insecticide on it also kills mosquitoes who try to enter; while untreated nets provide some protection, treated nets are 50% more effective (Source 2 & 3). A literature review of studies of bednet distribution campaigns suggest that distributing nets in a region can reduce risk of infection by around 50% (Source 6 Pg 19), though we aren't sure how comparable the studied programs are to typical bednet distribution campaigns (particularly in terms of promoting use of the nets).
Components:
- Insecticide-treated nets. Nets last 3-5 years (Source 4), and generally cost $5-10 each (for example, in 2005 across all countries, PSI spent $6.58 (including marketing and distribution) per net sold - Source 5).
- Retreatment. Some types of insecticide-treated nets can remain effective for 5-7 years without retreatment; others must be retreated with insecticide every 6 months (Source 3).
- Distribution. Getting bednets into the hands of those who need them is not necessarily straightforward (anecdotally, free bednets can be diverted from their intended purpose).
- Promotion. As our PSI page details, utilization is far from given: even people who own nets often do not use them (and in the case we linked to, this is despite extensive promotion efforts).
Our applicants: PSI has a major ITN program that we discuss in detail.
Sources:
- Source 1: Lengeler, C. 2004. "Insecticide-Treated Bed Nets and Curtains for Preventing Malaria." Cochrane Database Systematic Reviews (2) CD000363.
- Source 2: Effect of large-scale social marketing of insecticide-treated nets on child survival in rural Tanzania
- Source 3: DCPP, Conquering Malaria: Interventions and their Effectiveness
- Source 4: Cost effectiveness of malaria interventions
- Source 5: Population Services International, Unit Cost Analysis Report, 2005.
- Source 6: Global Health Council Malaria Overview
- Source 7: Study of Olyset nets in Tanzania
Other solutions
The World Health Organization endorses bednets as the primary method for malaria prevention. We have not run across the alternative methods described below in our applications, but we'll cover them briefly.
- Indoor residual spraying (IRS) involves spraying pesticides (often DDT) on the insides of homes, to kill and drive away mosquitoes (Source 1). One application can last for up to 6 months (Source 1); research suggests that conducting IRS in an area can reduce malaria incidences by up to 20-30% (Source 2).
- Intermittent preventative therapy (IPT) involves treating pregnant women with medicine, designed to prevent transmission of malaria to their children. There is no clear consensus on efficacy: there are indications that SP (the common drug used) is becoming ineffective, and that doctors should try another drug, ACT (Source 1).
- Early diagnosis and treatment. When malaria is identified within 24 hours of when an individual first exhibits symptoms, even severe cases can be successfully treated (Source 1). This intervention requires a trained doctor to monitor the infection's reaction to the drugs administered (Source 1), since there are three different possible drugs and each may be ineffective for a given patient (Source 4). (PIH is an example of an organization that likely improves the quality of medical care of malaria by treating malaria in a hospital or clinic with trained doctors and health workers.)
Sources:
- Source 1: DCPP, Conquering Malaria: Interventions and Their Effectiveness
- Source 2: "Efficacy of IRS and ITNs"
- Source 3: DCPP: Conquering Malaria, Intro
- Source 4: DCPP: Conquering Malaria, Economics of Malaria Control Interventions
HIV/AIDS
People can be infected with HIV through the transmission of bodily fluids, as in sexual intercourse with an infected individual, and the use of unclean needles (Source 1). HIV can eventually lead to the development of AIDS, and if left untreated will usually lead to death within 10 years (Source 1). Between 2% and 5% of people in sub-Saharan Africa are infected with HIV, though prevalence varies widely by country, and exceeds 15% in several countries including Burkina Faso, Lesotho, Namibia, Swaziland, and Zimbabwe (Source 2).
Sources:
- Source 1: Wikipedia: HIV
- Source 2: WHO Global Atlas
Promoting abstinence, monogamy, and/or condoms
Since sex is a primary means of contracting HIV, changes in sexual behavior can reduce risk. Condoms, used properly, are nearly 100% effective at preventing HIV transmission during sex (Source 1); reducing one's sexual partners mathematically reduces the risk as well. Interventions aimed at increasing consistent condom use have successfully reduced the HIV transmission rate in the past (Source 3), but there is little data to show how effective abstinence promotion and partner reduction efforts are.
Components:
- Promotion and education. We believe that promotion and education are particularly challenging for any strategy targeting sexual behavior, whether focusing on abstinence, monogamy, condoms, or all three. Without hard evidence, we do not assume that any attempt to get people to change their sexual habits is successful.
- Condoms. These are generally extremely cheap: for example, PSI reports costs of $.01-$1.08/condom sold, with an average cost of $.10, including condoms, distribution and overhead. The condoms themelves cost PSI 1-3 cents each (Source 4).
Our applicants: PSI uses these types of strategies extensively, particularly distribution of condoms. Food for the Hungry conducts programs focused on encouraging abstinence, though we have no knowledge of their programs' effectiveness.
Sources:
- Source 1: NIH review of condom efficacy
- Source 2: DCPP, HIV/AIDS: Estimated HIV Transmission and Risk per Exposure
- Source 3: Thailand's 100% condom program
- Source 4: Population Services International, 2005 Unit Cost Analysis
- Source 5: Condom utilization study #1
- Source 6: Bentley, M. E., K. Spratt, M. E. Shepherd, R. R. Gangakhedkar, S. Thilikavathi, R. C. Bollinger, and S. M. Mehendale. 1998. “HIV Testing and Counseling among Men Attending Sexually Transmitted Disease Clinics in Pune, India: Changes in Condom Use and Sexual Behavior over Time.” AIDS 12 (14): 1869–77. Full text not available online
Antiretroviral Therapy (ART)
Antiretroviral therapy is a rigid, scheduled drug regime that strengthens the immune system and prevents the onset of the opportunistic infections that kill HIV/AIDS patients (Source 1). If offered to patients who exhibit the symptoms of an opportunistic infection, ARVs can cause more harm than good (Source 1). However, ARV therapy allows most patients to maintain a quality of life - as measured by pain, anxiety, mobility, self-care, and normal activity - similar to those without HIV/AIDS (Source 2).
Components:
- Antiretroviral drugs. ARVs (antiretroviral drugs) are often very expensive (Source 1), and costs of treatment can vary by up to two orders of magnitude.
- Medical staff must screen the patient to identify whether he/she is suitable for ART (those whose immune systems are already too suppressed are not suitable); medical staff must also manage any side effects that result from ART (Source 1).
- Patient adherence to the regimen. Patients must take medicine as scheduled to receive the full benefits (Source 1). The regimen is intensive at first: weekly for the first two weeks, every 2 weeks for the first two months, and monthly thereafter (Source 2). The DCPP states: "Studies in India, Mexico, Senegal, and Uganda point to poor adherence (which for some classes of drugs can be adherence of less than 95 percent), inadequate doses and regimes, and poor monitoring as factors that contribute to more rapid development of antiretroviral therapy resistance" (Oyugi and Bangsberg 2004, Laniece and others 2004, Bautista and others 2003, Liechty and Bangsberg 2003). By contrast, experiences in Haiti and Uganda suggest that it is possible to achieve adherence rates in developing countries equal to or better than those observed in high-income countries (Farmer and others 2001; Mitty and others 2002)" (Source 1). As a note, we sometimes see adherence rates much lower than 95 percent cited for the developed world, but believe this is due to the fact that ART is generally expensive in the developed world (whereas in the developing world it is generally offered it for free).
Our applicants: PIH has a major ART component to its programming, using community health workers to encourage people to adhere to their treatment regimes.
Sources:
-
Source 1: DCPP, HIV/AIDS Prevention and Treatment: Care and Treatment
Source 2: Case study of patients on ARV in South Africa
Voluntary counseling and testing
Offering tests for HIV/AIDS and diagnosing those who have it may help encourage those who are infected to seek treatment (Source 1) - and perhaps to change their sexual behavior, though we haven't seen examples of the latter documented in practice.
Components:
- Doctors.
- Medical equipment.
Sources:
Prevention of mother-to-child transmission (PMTCT)
There is evidence that putting a pregnant mother on ART reduces the likelihood that she will transmit HIV to her child (Source 2); such programs often also discourage breastfeeding, as the virus can be transmitted through breastmilk (Source 1).
Components are largely the same as for ART, though the benefits are more concentrated (i.e., PTMCT is a relatively short regimen that can prevent an infection, whereas ART must be administered continually and indefinitely for adults). PMTCT programs also commonly offer food or formula as an alternative to breast milk (PIH's program employs this tactic).
Our applicants: PIH has a major PMTCT program.
Sources:
Pneumonia/acute respiratory infections (ARIs)
ARIs - mostly pneumonia and bronchitis - are a major source of under-5 mortality, with pneumonia alone accounting for "about one-fifth of the estimated 10.6 million deaths per year in young children" (Source 1). Virtually all deaths from ARIs are due to pneumonia (Source 2 Pg 5). 3 out of 10 children under 5 in sub-Saharan Africa contract pneumonia each year (Source 2), and 1 out of every 40 cases results in death (Source 3). Despite the severity of this issue, we have seen few projects that focus on it, possibly because there is no cheap and straightforward way to prevent these deaths (as is true for diarrhea as well, see discussion below).
Sources:
- Source 1: DCPP, Acute Respiratory Infections in Children: Abstract
- Source 2: UNICEF Pneumonia overview
- Source 3: Deaths by Cause, Sex, and Age in the Sub-Saharan Africa Region, 2001 (thousands)
Treatment
Depending on the severity of an infection, an ARI can require days of hospitalization (Source 1). UNICEF estimates that only 40% of cases in sub-Saharan Africa receive proper care (Source 2).
Components:
- Medication. Multiple drugs can be necessary, depending on the severity of the infection (Source 1).
- Medical facilities and personnel. Full hospitalization, and diagnosis by qualified doctors, can be required (Source 1).
Our applicants: About 15% of PIH's initial consultations show and about 4% of its hospitalizations are for respiratory tract infections.
Sources:
Prevention
.
There is some indication that pneumonia can be less of a risk for children who:
- Are vaccinated against other diseases (measles, diphtheria, pertussis, etc. - see Source 1).
- Have access to good sanitation (Source 1).
Sources:
Diarrhea
Diarrhea in young children living in poverty can be so severe that it results in death by dehydration (usually this only occurs in infants under five). In sub-Saharan Africa, each child under-5 has 3-5 episodes per year of diarrhea (Source 1); in 2001, 1.6 million children died from diarrhea (Source 2).
The bacteria responsible for many of these cases of lethal diarrhea are found in human feces and can reach a person in many possible ways (as shown in the UNICEF diagram below), including a contaminated water supply; speaking informally, most water-related projects we've seen focus on diarrhea prevention as their justification. However, there are also many other ways to contract diarrhea, and thus many other ways to save lives from it; moreover, what we know suggests that other methods are generally more cost-effective.

Sources:
- Source 1: Number of episodes, per-child per-year
- Source 2: Total deaths from diarrhea
Improving the quality of the water supply
Many projects focus on water infrastructure - that is drilling wells or boreholes in order to make clean water more accessible. As the diagram above shows, this eliminates only one of the many ways for people to contract diarrheal diseases (though it can also improve the efficacy of hand-washing, if hand-washing is already practiced regularly). Moreover, improving water infrastructure tends to be expensive and complex. Research suggests that improved hygiene and sanitation practices (detailed below) are more effective at reducing incidence of diarrhea than improving the quality of the water supply at its source (Source 1). We don't suppose that water infrastructure projects are never warranted, but we have yet to see a compelling demonstration of their cost-effectiveness in improving life outcomes.
Components:
- Materials and labor. Unlike most of the interventions on this page, improving the water supply requires a fairly large-scale operation.
- Maintenance to ensure the continued quality of infrastructure and water.
- Promotion. In rural areas, it is not uncommon to walk long distances for water (Source 2); making the local population aware of both the availability and importance of a clean water supply can improve quality of life by reducing the amount of time (largely) women spend collecting water.
Sources.
- Source 1: Interventions to prevent diarrheal diseases, literature review
- Source 2: DCPP, Water Supply, Sanitation, and Hygiene: Water Supply
Hygiene promotion
Since unwashed hands are responsible for a large portion of bacteria transmission, promoting improved hygiene practices (in particular, hand-washing after using the bathroom, changing a child's diaper, before eating, etc.) have proven effective at reducing the incidence of diarrhea by 33%-50% (Source 1 & 3).
Effective education and hygiene promotion are essential to actually changing peoples' hygiene habits. Convenient access to water is also vital (see above).
Our applicants. Most CSHGP programs, including those run by Food for the Hungry and Project HOPE, incorporate hygiene education.
Sources.
- Source 1: Hygiene promotion literature review #1
- Source 2: DCPP, Water Supply, Sanitation, and Hygiene: Hygiene Promotion
- Source 3: Hygiene promotion literature review #2
Oral Rehydration Therapy (ORT)
A packet of basic nutrients can be given to a child with diarrhea to prevent dehydration. This does not alleviate symptoms (Source 5), but prevents death 95% of the time (Source 4). ORT is credited with drastically reducing deaths from diarrhea at the national level (Source 2). Packets come pre-made, or parents can mix their own solution of salt, sugar, and water (Source 1).
Zinc is sometimes given as a supplement to ORT (Source 8), and can reduce the duration and severity of diarrhea (Source 9); this added benefit may increase ORT utilization among mothers.
Components.
- Packets of nutrients. These are extremely cheap. (In fact, a reasonably effective version can be made simply by mixing $.02 worth of sugar and salt.) (Source 6)
- Distribution or education.
- Distribution. ORT is widely available in much of sub-Saharan Africa - in 2000, WHO estimated that 64% of diarrhea cases were treated with ORT (Source 2), so it is not necessarily straightforward to reach uncovered areas (which are uncommon).
- Education. Because caregivers can mix ORT at home, educating them on when and how to mix it also works and alleviates the need for distribution of pre-made packets. This type of program was successfully implemented in Brazil in the 1980s (Source 2).
Our applicants. PSI sells and promotes ORT. Most CSHGP programs, including those run by Food for the Hungry and Project HOPE, include education on preparation of ORT.
Sources.
- Source 1: Description of ORT
- Source 2: ORT background paper
- Source 3: ORT utilization
- Source 4: ORT cost and effectiveness
- Source 5: ORT and symptoms
- Source 6: Cost of ORT home remedy
- Source 7: Number of episodes per-child, per-year
- Source 8: WHO/UNICEF Joint Statement on Clinical Management of Acute Diarrhoea
- Source 9: Literature review on zinc supplementation
Sanitation infrastructure (i.e., latrines)
In areas with poor sanitation infrastructure, people often defecate in the open. As a result, children more easily come into contact with fecal matter, and flies pick up the bacteria and transfer it to people or food. Improved sanitation infrastructure (latrines, toilets, septic tanks, etc.) reduces the likelihood of transmission by containing fecal matter (Source 2). In fact, past measurements have suggested that sanitation projects may reduce diarrhea rates by 30-40% (Source 1).
Components.
- Materials and labor. Unlike most of the interventions on this page, improving sanitation infrastructure requires a fairly large-scale operation.
- Maintenance to ensure the continued quality of the infrastructure.
- Promotion: convincing people to use latrines, once constructed, involves getting them to change their habits. For this reason, we are wary of any sanitation project that does not include a measurement of changed local attitudes or behavior.
Sources:
- Source 1: Water Supply and Sanitaion Literature review #1
- Source 2: Water Supply and Sanitaion Literature review #2
- Source 3: DCPP: Water Supply, Sanitation, and Hygiene Promotion: Excreta Disposal
Breastfeeding promotion
Maternal breastfeeding (feeding children solely through breast milk) for the first 6 months after birth may reduce a child's vulnerability to diarrhea (Source 1).
The major component of this strategy is effective education and promotion, aimed at behavior modification. In general, though, breastfeeding is already heavily practiced in Africa (Source 2), so we're not sure of the degree to which additional promotion is warranted or necessary. Another concern is that mothers who choose to breastfeed can transmit HIV to their children through breastmilk.
Our applicants. Most CSHGP programs, including those run by Food for the Hungry and Project HOPE, incorporate education on breastfeeding-related issues.
Sources:
- Source 1: Lancet article
- Source 2: DCPP, HIV/AIDS Prevention and Treatment: Action Under Uncertainty
Measles
Although a vaccine exists that is more than 98% effective with two doses (Source 1), measles is still a leading cause of death among children in sub-Saharan Africa; it kills more than 350 thousand children annually (Source 2). For those infected, the mortality rate is between .5% and 10% (Source 1).
Sources:
Vaccination
Currently, vaccine coverage is estimated at 77% (Source 1), and additional interventions generally focus on increasing coverage - often through discrete "campaigns" that attempt to reach as many people as possible within a country or region (Source 2).
Components:
- Vaccinations. These appear cheap: the Measles Initiative claims that they cost less than a dollar per child.
- Distribution. Due to the already high level of coverage, the main challenge is presumably the logistical challenge of getting vaccinations to areas that have not yet been reached. Source 2 gives some analysis of how this might be accomplished.
Sources:
Tuberculosis
Tuberculosis, an infectious disease that attacks the lungs and nervous system, is a major cause of death for people of all ages. 0.75% of all people in sub-Saharan Africa contract TB each year (Source 1). Untreated cases have a 50% mortality rate (Source 3), but with standard DOTS treatment (see immediately below) the mortality rate can fall to 20-30% (Source 2).
Sources:
- Source 1: WHO Tuberculosis Overview
- Source 2: WHO Global Health Atlas
- Source 3: Tuberculosis in developing countries
Directly Observed Treatment, Short-course (DOTS)
DOTS is the World Health Organization's recommended approach to fighting tuberculosis (Source 3), and includes not just to the medical treatment for tuberculosis but also to a set of practices for collecting data, managing the drug supply, etc. (Source 3). DOTS involves diagnosis using appropriate technology, followed by a 6-8 month chemotherapy and drug treatment regimen conducted under medical supervision (Source 1 and 2). As stated above, this treatment can significantly reduce the risk of death from tuberculosis - from around 50% to around 20-30%.
Components:
- Medical facilities and personnel. Both diagnosis and treatment appear relatively complex, so adequate health facilities and staff are needed.
- Patient adherence. The World Health Organization recommends direct supervision due to the complexity of the treatment.
Our applicants: PIH has a major tuberculosis treatment component which includes the use of community health workers to supervise patients' adherence.
Sources:
- Source 1: DCPP, Tuberculsis: Interventions against Tuberculosis
- Source 2: WHO DOTS Primer
- Source 3: WHO homepage for DOTS
Maternal and perinatal deaths
Perinatal deaths (deaths of the infant in childbirth) and maternal death (death of the mother in childbirth) together account for about 800,000 deaths annually in sub-Saharan Africa (Source 3). Researchers estimate that between 0.5% and 1.5% of all live births in sub-Saharan Africa end in the mother's death (Source 1), generally from hemorrhage, sepsis, or obstructed labor; 10% of live births end in the child's death (Source 2), generally from birth asphyxia and low birthweight (Source 3).
Sources:
- Source 1: Maternal mortality estimates 2005
- Source 2: Neonatal mortality rate, 0-28 days after birth.
- Source 3: Deaths by Cause, Sex, and Age in the Sub-Saharan Africa Region, 2001 (thousands)
Preventing unwanted pregnancies
According to the DCP, "a significant unmet need for contraception persists in many developing countries, with high levels of unsafe abortion as a proxy indicator of that need" (Source 1). Improving access to birth prevention can therefore save lives both by reducing the number of both unsafe abortions and deaths that occur in childbirth.
Components:
- Contraception supplies. Condoms and oral contraception are the most common methods.
- Distribution. Contraception materials generally must be replaced with more frequency than many of the other materials on this page (bednets, vaccines, vitamin A supplements, etc.) This creates something of an additional challenge in distribution.
- Promotion. We would guess that promoting condoms is more difficult than promoting other contraception methods, partly because the woman has more direct control over other methods, and partly because condoms affect sexual pleasure. On the other hand, condoms have the additional benefit of protecting people from sexually transmitted diseases including HIV.
Our applicants. PSI has a significant focus on contraception, both condoms and other methods.
Sources:
- Source 1: DCPP, Maternal and Perinatal Conditions, Interventions
- Source 2: NIH review of condom efficacy
- Source 3: DCPP, Contraception: Interventions
Improved medical care
Deaths in childbirth can largely be averted through the use of strong medical care and facilities (Source 1); facilities must not only exist, but people must be encourage to use them when giving birth.
Components:
- Medical facilities and personnel, particularly staff who can identify, prevent and address complications (Source 1).
- Access. In rural areas, women cannot necessarily reach a facility when giving birth. Some efforts therefore include the use of birth attendants (Source 1) who arrange a transfer to a facility if necessary.
- Promotion. Women are not necessarily aware of the (potentially life-saving) benefits of giving birth in an appropriate setting.
Our applicants. PIH focuses on improving medical facilities; these efforts presumably include improving the quality of maternal care.
Sources:
Improved nutrition
The link between nutrition and childbirth complications is not well understood, and it is not clear whether targetting pregnant women for short-term, timed interventions are effective (Source 1). However, there is a link between malnutrition and maternal survival (Source 1), so improving nutrition may lead to fewer deaths.
Malnutrition
Malnutrition accounts for a large portion of the disease burden in developing countries (Source 1 Pg 1). UNICEF estimates that 50% of child mortality worldwide is partially caused by malnutrition (Source 2 Pg 5). Unlike the other problems mentioned above, malnutrition generally works in conjunction with other diseases and increases mortality insofar as malnutrition weakens immune systems and renders people more vulnerable (Source 1 Pg 1). According to Source 1 (Pg 1), the nutritional deficiencies that account for the majority of malnutrition's impact on the global burden of disease are:
- Iron deficiency, which can lead to anemia - a deficiency of red blood cells that can cause general weakness and fatigue (see Wikipedia for more information), and affects 40-55% of women in developing countries (Source 1 Pg 1). Research suggests that eliminating anemia among pregnant women would reduce maternal mortality by 13% (Source 1 Pg 1).
- Iodine deficiency, which may contribute to lower productivity and lower intelligence (Source 1 Pg 11) and can also lead to goiters, a swelling in the neck that affects 600 million people worldwide. Research suggests that reducing iodine deficiency would reduce child mortality by 8% (Source 1 Pg 1).
- Vitamin A deficiency, which may contribute to several causes of child mortality. Source 3 below is a literature review of studies that test the impact that Vitamin A supplementation has on child mortality in general and on child mortality associated with diarrhea, pneumonia, and measles in particular; the summary on Pgs 367-368 implies that were Vitamin A supplemenation universal, under-5 mortality would likely fall by 20-30%.
Note that we do not have high confidence in this 20-30% number, which we examined thoroughly since many of our applicants (particularly HKI) focus on Vitamin A deficiency. The studies cited generally compare children given Vitamin A supplements to other children, but are not specific about (a) the profiles of these populations in terms of their existing levels of Vitamin A deficiency or their risk of death from other causes; (b) what types of early death were found to be lower in those receiving Vitamin A supplements; or (c) whether other factors may be at play - such as the fact that those receiving Vitamin A were generally more intensely observed, and thus may have received improved general healthcare.
Sources:
- Source 1: Malnutrition working paper through the DCPP
- Source 2: UNICEF Pneumonia overview
- Source 3: Glasziou PP, Mackerras DEM. Vitamin A supplementation and infectious diseases: a meta-analysis. BMJ 1993;306:366–70. (Available through Pubmed).
Distributing medical supplements
Medical supplements can directly address the deficiencies listed above.
Components:
- Medical supplements. These are generally inexpensive. HKI delivered Vitamin A doses at $.19/dose (see Source 1 Pg 5).
- Distribution and promotion. Some programs, like HKI, administer the supplements directly to children; others, including some CSHGP programs, distribute the supplements to households. In either case, the program must ensure that pills are not only taken, but also taken on the appropriate schedule. For example, Vitamin A supplements should be taken twice per year. (Source 1 Pg 3)
Our applicants. HKI is involved in a major Vitamin A supplement program; our CSHGP generally include distribution of Vitamin A supplements; PSI has a program for marketing multivitamins.
Sources:
- Source 1: HKI VAS Annual Progress Report, 2006
Distributing food
Distributing nutrient-rich food may also help to address malnutrition, although not necessarily simply or reliably. While medical supplementation can address specific malnutrition issues with an occasional dose (for example, two Vitamin A supplements per year), this method presumably requires a constant change in diet.
Components:
- Food.
- Distribution. We would guess that distribution is particularly challenging for food, since (a) it presumably requires constant (rather than periodic) distribution, and (b) it seems easy for less-needy people to take advantage of the aid.
Our applicants. PIH gives food packages to many of its patients; other than this, we haven't seen many programs focused specifically on food distribution.
Neglected tropical diseases (NTDs)
"NTDs" is a term sometimes used (for example, by the Global Network for Neglected Tropical Disease Control (GNNTDC)) for diseases that are common in the developing world, have large impacts on quality of life (ranging from malnutrition to blindness and distortion of limbs), and generally receive insufficient attention in the world of charity. Our understanding of these diseases is limited to the information in papers GNNTDC sent us (and other papers that these papers referenced), and it is far more limited than our understanding of the issues above.
- Intestinal parasites (ascariasis, trichuriasis, hookworm, and schistosomiasis) are all worm infections that can lead to malnutrition and anemia (see Source 1 Pg 548, and Source 2).
- Onchocerciasis can lead to both skin disease and blindness/severe visual impairment; the latter happens in about 4.2% of onchocerciasis cases (Source 3), though we have no information on how severe and frequent skin disease is.
- Trachoma can cause blindness or severe visual impairment (about 10% of trachoma cases lead to this - see Source 4).
- Lymphatic filariasis is a disease that can lead to elephantiasis, a debilitating condition that renders limbs or other body parts useless. A third of lymphatic filariasis cases lead to some degree of elephantiasis (Source 5), though we don't know how often this elephantiasis is severe vs. minor.
Sources:
- Source 1: de Silva, N.R. et al. (2003) Soil-transmitted helminth infections: updating the global picture. Trends Parasitol. 19. (Available through PubMed)
- Source 2: Guyatt, HL, S Brooker, CM Kihamia, A Hall and DA Bundy. “Evaluation of efficacy of school-based anthelmintic treatments against anaemia in children in the United Republic of Tanzania,” Bull World Health Organ, 2001, 79(8): 695-703.
- Source 3: : Basáñez MG, Pion SDS, Churcher TS, Breitling LP, Little MP, et al. (2006) River Blindness: A Success Story under Threat? PLoS Med 3(9): e371
- Source 4: : WHO Vision2020 initiative
- Source 5: WHO, “Global programme to eliminate lymphatic filiariasis: Annual report on lymphatic filiarsis” Weekly Epidemiological Record, 2006, 81: 221-232.
Drug treatments
GNNTDC lays out a plan for a Rapid Impact Package to treat all of the diseases mentioned above with a variety of drugs, administered 1-3 times per year.
Deformities requiring surgery
Congenital defects and burn scars that would be quickly corrected in the developed world can significantly affect quality of life in the developing world if qualified surgeons are not available. Here we focus on the types of surgeries addressed by Interplast, one of our finalists.
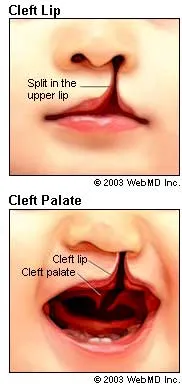
- Cleft lip or palate. A split in the lip or the roof of the mouth (palate) leads to an extreme facial deformity (see diagram, from Source 1). Source 1 specifies that if treated correctly, a child with a cleft lip or palate can live a normal life. However, if surgery and speech therapy are not available, it a child with a cleft lip or palate will be severely deformed in face and speech, and possibly encounter malnutrition issues as well.
- Ptosis. A drooping eyelid that, if severe and left untreated, can lead to serious vision impairment. Even without treatment it can also be a relatively minor facial deformity (Source 2).
- Hand deformities. Interplast treats significant numbers of people with hand deformities; see examples from its blog here and here We would guess that a hand deformity does not impact quality of life nearly as much as a significant facial deformity.
- Burn scars. Correcting burn scars is a major focus of Interplast's activities (see its review page for details). We have no way of knowing how common severe vs. minor burn scars are; the examples we found on the Interplast blog range from extremely severe deformity and debilitation to less severe cases that seem restricted to a limb or other area of the body.
It is easy for us to see how, especially in a developing-world setting, a facial deformity could lead to ostracization. Source 3 states that 3% of disabled children attend school in developing countries, though we don't know where this claim is sourced or what is meant by "disabled." It seems possible that a hand injury could have a real impact on productivity and life outcomes as well. However, we have little context for truly understanding the extent of this debilitation, especially because we have no data on how common severe vs. minor deformities are.
Sources:
- Source 1: WebMD: Cleft Lip and Palate.
- Source 2: eMedicine: discussion of congenital ptosis
- Source 3: Interplast fact sheet on burns
Surgical missions
Since correcting deformities can require significant skill, the problem is sometimes approached by sending teams of developed-world medical personnel (volunteers) overseas for a defined period of time, to treat all comers. See our writeup on Interplast for an example.
Components.
- Volunteer medical personnel. Without volunteers, this sort of operation becomes extremely expensive, due to the high market value of skilled developed-world medical personnel.
- Transportation and accommodation to house the personnel.
- Medical facilities: a local facility is required with enough basic equipment to facilitate surgeries.
Training local personnel
As our writeup on Interplast shows, it appears that significant money can be saved by training local personnel to perform certain surgical operations (particularly for clefts and burn scars).
Components.
- Skilled medical trainers to teach operations.
- Transportation and accommodations for the trainers.
- Reasonably skilled local medical personnel who can be trained to perform such operations.