Fortify Health — General Support (2019)
Published: January 2020
Note: This page summarizes the rationale behind a GiveWell Incubation Grant to Fortify Health. Fortify Health staff reviewed this page prior to publication.
Summary
As part of GiveWell’s work to support the creation of future top charities, in August 2019, GiveWell recommended a grant of $1,005,716 from the Effective Altruism Global Health and Development Fund to Fortify Health to support its whole wheat flour iron fortification program over two years in Maharashtra and West Bengal, India. Fortify Health previously received an incubation grant in June 2018.
Table of Contents
The intervention
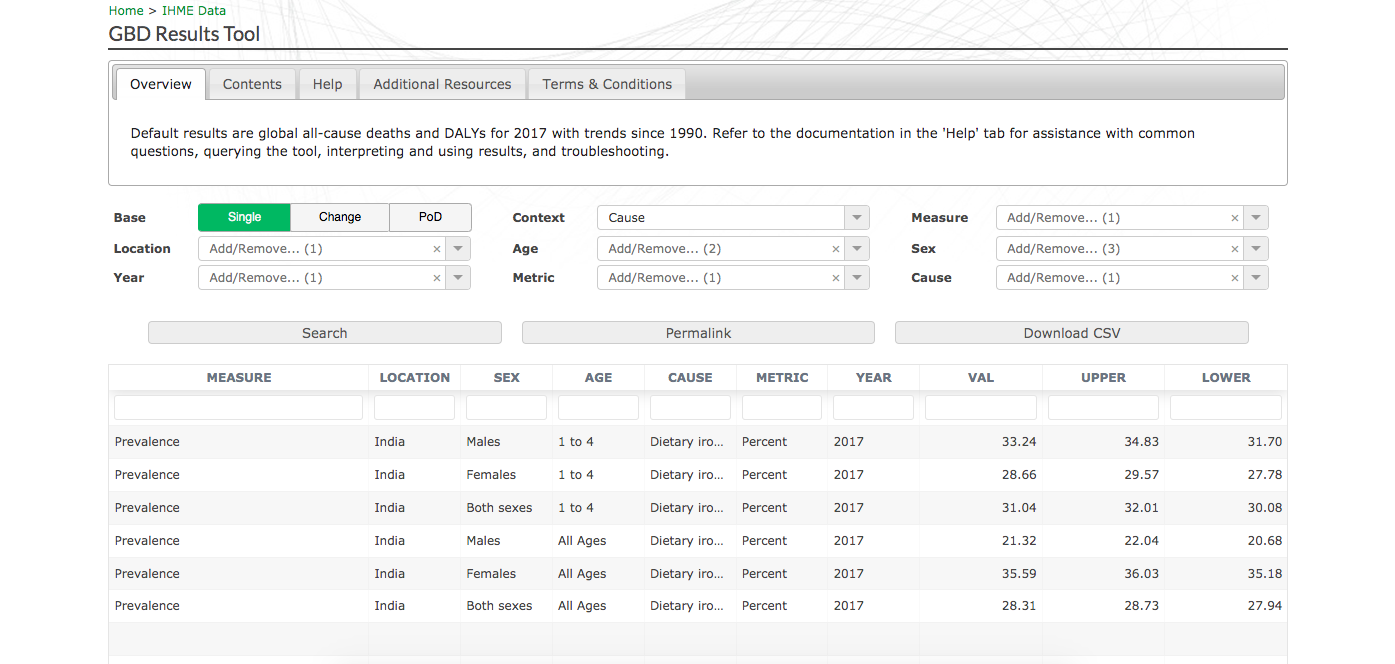
Mass fortification of wheat flour with iron involves adding iron to industrially produced flour in mills in order to decrease the prevalence of iron deficiency in the population. The World Health Organization (WHO) reports that iron deficiency is thought to be the most common cause of anemia,1 and that this can negatively affect physical and cognitive development in children, productivity, and birth weight.2 The Global Burden of Disease estimates that in India, about 31% of children under five, 36% of women, and 28% of the population in general have some degree of iron-deficiency.3
In our current cost-effectiveness model for this program (further discussion below), we model three key benefits of iron fortification:4
- Benefits from averting anemia-related morbidity (39% of the value of the program in our current model)
- Cognitive benefits for children (8% of the value of the program)
- Cognitive benefits for adults (53% of the value of the program)
We have done a preliminary review of the evidence for iron fortification and we plan to complete a report detailing the evidence on the impact and cost-effectiveness of iron fortification in the future.5 Our report on iron supplementation for school-aged children is here.
The organization
Fortify Health pays for and installs the equipment needed to fortify flour and pays for premix (which contains the iron compound that is used as a fortificant) so that its partner mills can fortify flour at no additional cost.6 It partners with privately-owned mills that produce flour that is sold at market prices to consumers.7
Fortify Health was founded in September 2017.8 As of March 2019, Fortify Health had verbally agreed to partnerships with four mills;9 in April 2019, Fortify Health confirmed that it had signed formal agreements with two of the mills and had installed fortification equipment in one mill.10
Planned activities and budget
Fortify Health shared with us two potential plans for expansion:
- A "low bound" plan to partner with 8 new mills over the next year (bringing it to 12 partner mills total), and
- A "high bound" proposal to partner with 16 new mills over the next year (bringing it to 20 partner mills total).11
This grant amount is enough to cover Fortify Health's "low bound" scale-up plan, as well as serve as an exit grant which will enable Fortify Health to maintain operations at that level for an additional year (July 2020 to July 2021) in the event that we choose not to make an additional grant one year from now.
We have not placed restrictions on how quickly Fortify Health can scale up with the grant funding; if it chooses to scale-up faster over the next year than its "low bound" proposal, then it would also need to scale down faster if we do not make another grant one year from now.12
If Fortify Health chooses to pursue its low bound plan, we expect its spending of this $1,005,715, plus $100,000 in funds left over from the previous grant we recommended, to break down roughly as follows:
- $575,079 to scale up its operations to eight additional partner mills and continue working with four current partner mills.13
- $52,658 to investigate partnership opportunities with the Indian government.14
- $477,979 to enable Fortify Health to continue its operations at the low-bound scale from July 2020 to July 2021 if we decide not to recommend an additional grant in July 2020.
In general, we believe it is a good practice to offer exit grants to organizations we support, in order to:
- Enable the organization to remain operational long enough to seek out other sources of funding.
- Reduce potential harms to the staff, partners, and program beneficiaries of the organization which might result from a sudden shut down.
- Maintain a reputation as a responsible funder.
In this case, we've chosen to provide funding now which could function as an exit grant if we choose not to renew (rather than making an additional exit grant later) for a number of reasons:
- It allows us to account for the full expected costs of the grant up front, since (for the reasons described above) we expect that we would, in any event, either make an exit grant or renew funding after this year.
- It provides the charity with better visibility into its future funding situation.
- It reduces the potential for cash flow difficulties for the organization that might have arisen from the timing of exit or renewal grant disbursement.
Case for the grant
Cost-effectiveness
Our cost-effectiveness analysis (CEA) estimates that, taken together, this grant and the future incubation grants that we would need to make to get Fortify Health to the point of evaluation for top charity status, are about 13x as cost-effective as cash.15
We've estimated the total expected additional cost of grants to Fortify Health before we evaluate it as a potential top charity (including this grant) to be $4.5 million.16 About 23% of the value of these grants, in our model, is from the direct health benefits of Fortify Health's program during the period funded by the grants,17 and about 77% of the value is from the possibility that we will recommend Fortify Health as a top charity in the future18 and subsequently reallocate funds away from less cost-effective giving opportunities.19 Our cost-effectiveness model currently assigns an overall likelihood of 25% to Fortify Health becoming a top charity.20 See the next section for more detail on the expected value of Fortify Health becoming a top charity.
Cost-effectiveness of Fortify Health at scale
We modeled the cost-effectiveness of Fortify Health's program in a "steady-state" (modeled as the period from July 2021 to July 2026). We estimate the program in that period will be approximately 11x as cost-effective as cash transfers.21 Modeling lower and upper bounds for the effect of iron fortification on the risk of iron deficiency in the model gives a range of 9x to 15x cash.22 This is in line with the cost-effectiveness of our current top charities. We therefore believe that Fortify Health's program represents a promising opportunity to potentially create a future top charity.
Factors not included in our cost-effectiveness model
In addition to iron, Fortify Health simultaneously fortifies wheat flour with folic acid and vitamin B12. We have not included the benefits of folic acid fortification in our cost-effectiveness analysis because the levels of folic acid fortification permitted by current Indian government standards are thought to be inadequate to prevent neural tube defects.23 We also exclude the benefits of vitamin B12. Furthermore, we exclude the benefits of iron on averting maternal deaths, as we believe the effect is likely negligible.24
Our cost-effectiveness model only takes into account potential benefits from Fortify Health's core activity of partnering with mills who produce flour for the open market. We have not attempted to model the expected benefits of Fortify Health's plans to explore partnering with the government.
Operational track record
We are impressed that Fortify Health has been able to form partnerships with four private sector mills (two with signed contracts and two with verbal agreements), despite having only existed for roughly a year. When we recommended the first incubation grant to Fortify Health, we believed there was 50% chance that it would not have formed partnerships with any mills after one year.
Risks and reservations
Uncertainties about our cost-effectiveness model at the intervention level
Iron fortification is unusually difficult to model (compared to models we have previously built), and we believe there is a higher chance than for most interventions that we may revise our CEA substantially at the intervention level. In particular, we are highly uncertain about the size of cognitive benefits for adults from iron fortification; there is limited randomized controlled trial (RCT) evidence looking at adult cognitive benefits, and all such RCT evidence that we have identified is restricted to premenopausal women. In our current model, adult cognitive benefits comprise 53% of the value of Fortify Health's program.25 The assumptions in our CEA represent our current best guess, but it is possible that with further research we will adjust our estimate of the cognitive benefits for adults downward.
Uncertainty about comparing Fortify Health's program to academic studies
A key uncertainty in our cost-effectiveness analysis for this grant is how the effect size of Fortify Health's program is likely to compare to the effect size observed in the academic studies we looked at. This is difficult to predict for a number of reasons:
- The level of iron intake from fortified products consumed in academic studies might be different than the level in Fortify Health's program.
- Conditional on the quantity of iron intake, the amount of iron absorbed might differ between the studies and Fortify Health's program, for several reasons:
- Different fortification compounds and vehicles may have different absorption rates. Fortify Health uses ferric sodium EDTA (NaFeEDTA) in whole wheat flour, but the academic studies use many different fortification compounds (e.g. ferric sodium, ferrous sulfate, ferrous fumarate, ferric pyrophosphate, electrolyte irons, etc.) in many different vehicles (e.g. rice, salt, sauce, milk, etc.).
- Certain substances inhibit the absorption of iron (e.g. tannins and phytates),26 and certain substances enhance the absorption of iron (e.g. ascorbic acid).27 The beneficiaries of Fortify Health's program might consume different levels of inhibitors or enhancers alongside the fortified food compared to the recipients in the academic studies.
- The level of absorption may also depend on baseline levels of iron in the blood (i.e. our impression is that absorption rates may be higher when initial iron levels are lower, though we have not yet deeply investigated the relevant literature).28
- Conditional on the amount of iron absorbed, it is possible that iron has a greater effect on health outcomes for recipients with a lower initial iron status.
Given these considerations, our best guess is that:
- Iron intake from Fortify Health's program is approximately 67% of the average seen in the academic studies.29
- The level of iron absorbed from Fortify Health's program is approximately 167% of the average in the academic studies,30 because (unlike many of the studies) it uses the fortification compound NaFeEDTA, from which the rate of iron absorption is relatively high.
Accordingly, we expect Fortify Health's program to have a larger health impact than fortification programs in the academic studies, but still considerably less impact than iron supplementation (which delivers a much higher quantity of iron).31
Uncertainties about our cost-effectiveness model for Fortify Health's program
The cost-effectiveness of Fortify Health's program likely depends to some degree on who consumes the fortified flour, in what quantities, and alongside what other substances. For example:
- It is possible that the quantity of iron absorbed in Fortify Health's program is lower than our model currently assumes, if the participants in the academic studies32 had a lower baseline level of iron than Fortify Health's beneficiaries and if the absorption of iron is greater for individuals with a lower initial iron status. We do not have information on the baseline iron levels of the beneficiaries of Fortify Health's program, and we have not deeply investigated the relationship between iron absorption rates and initial iron status.
- It is possible that the distribution of flour consumption across Fortify Health's beneficiaries is uneven, such that a non-negligible portion of its flour is consumed by individuals who have already consumed their optimal dose of iron and so no longer receive additional health benefits. We do not have information on the distribution of flour consumption across beneficiaries, and we have not deeply investigated the shape of the relationship between iron absorption and health benefits (e.g., whether health benefits increase linearly with iron absorption, or whether absorption past a certain level confers diminishing marginal benefits). However, our (very uncertain) best guess is that adjusting for the distribution of consumption across beneficiaries could increase our estimate of the program's cost-effectiveness (see footnote for discussion).33
- It is possible that the quantity of iron absorbed by beneficiaries of Fortify Health's program is lower than our model currently assumes, if Fortify Health's beneficiaries consume more tea alongside the fortified food than the participants in the academic studies from which we derive effect size estimates. We are aware of two studies that suggest that tea can substantially inhibit the absorption of iron from NaFeEDTA;34 we have not done a full search for research on this topic. The meta-analysis we rely on for the effect of iron fortification does not contain information on the diets of participants in the studies and we do not have information on the diets of beneficiaries of Fortify Health's program.
- It is possible that excess iron intake could have harmful side effects. Fortify Health has told us that the quantity of iron that its partner mills are fortifying with (21.25 mg of iron per kg of wheat flour) complies with Indian government standards,35 which are themselves comparable to WHO recommendations.36 Fortify Health told us that it plans to sample flour from its partner mills to determine iron levels in the flour in practice;37 we have not yet seen results. While the quantities of iron in Fortify Health's program may be less than or approximately optimal for the average consumer, it is possible that some consumers could eat a much larger amount of flour than the average, which could potentially lead to excess iron intake (see footnote for a rough examination of this possibility).38 We have not yet investigated the possible harmful side effects of excess iron intake in detail.
Organizational risks
- It is our understanding that one of Fortify Health's two co-founders, Brendan Eappan, is very likely to leave the organization to attend medical school in August 2019. While he may still play a small role in the organization moving forward, we are unsure how Fortify Health plans to replace him.39 Brendan has led Fortify Health's engagement with GiveWell, and we are somewhat concerned that his departure may reduce the speed at which Fortify Health is able to scale up its program.
- We do not have a strong understanding of Fortify Health's potential room for more funding. Our cost-effectiveness model for this grant relies heavily on the possibility that GiveWell might reallocate significant funds away from less cost-effective giving opportunities in the future if Fortify Health becomes a top charity. However, this would require that Fortify Health have significant room for more funding (we have currently assumed Fortify Health would be able to absorb $6.5 million per year, operating at scale, with a cost-effectiveness of 11x cash).40
Plans for follow up
As part of our follow-up on this grant, we plan to ask Fortify Health for the following information:
- A report on the number of mills that Fortify Health has installed equipment in or signed agreements to install equipment in.
- The quantity of iron in random samples of wheat flour from each partner mill that is fortifying, as measured through laboratory tests.
- Data on the amount of fortified flour that was sold by each partner mill that is fortifying.
To evaluate the success of this grant over the course of the next year, we plan to mainly look at how well Fortify Health is able to:
- Form new partnerships (i.e. install equipment or sign agreements to do so) with the number of mills that it intends to (i.e. with 8 new mills if it spends funds in line with its low bound scale-up proposal, or with 16 new mills if it spends funds in line with its high bound proposal)
- Maintain its partnerships with its four current partner mills
- Demonstrate that its partner mills consistently meet their targets for iron quantity in their fortified flour (i.e. 21.25 mg of iron per kilogram)
Beyond July 2020, we might ask for a more intense level of monitoring in order to evaluate Fortify Health for top charity status, which might include:
- A representative consumer survey to help us understand, e.g., consumption quantities, plate wastage, the consumption of inhibitors in beneficiaries' diets, and changes in the bioavailability of iron in flour stored in the household
- The collection of biomarkers (to directly monitor iron status in the blood), potentially as part of an RCT
- Information on the number of mills in the states that Fortify Health works in, and more detailed information about those mills' characteristics and activities (e.g. the proportion that are already fortifying flour)
Internal forecasts
For this grant, we are recording the following forecasts:
| Confidence | Prediction | By time |
|---|---|---|
| 25% | Fortify Health becomes a top charity. | November 2022 |
| 75% | Fortify Health has successfully signed agreements to install equipment with at least an additional 8 mills. | July 2020 |
| 25% | Fortify Health has successfully signed agreements to install equipment with at least an additional 16 mills. | July 2020 |
| 33% | Fortify Health has successfully installed equipment in at least 8 additional partner mills. | July 2020 |
| 10% | Fortify Health has successfully installed equipment in at least 16 additional partner mills. | July 2020 |
| 90% | Fortify Health successfully maintains its four existing miller partnerships. | July 2020 |
| 60% | Laboratory tests from random samples of atta produced by Fortify Health's partner mills do not fall more than 1mg below the target (21.25 mg of iron per kilogram of wheat flour) in more than 25% of cases. | July 2020 |
Our process
We previously investigated Fortify Health for our June 2018 incubation grant. As part of that investigation process, we had a number of conversations with Fortify Health. Since then, we have had five phone calls with Fortify Health to track the progress made on that grant.41 We created a CEA for iron fortification at the intervention level (focused on sub-Saharan Africa) and used that to create program-specific CEAs evaluating Fortify Health's program in Maharashtra and West Bengal. We had five phone calls and exchanged emails with Fortify Health to clarify various relevant points for these CEAs.
Sources
{kind=link}
- 1
"Iron deficiency is thought to be the most common cause of anaemia globally, although other conditions, such as folate, vitamin B12 and vitamin A deficiencies, chronic inflammation, parasitic infections, and inherited disorders can all cause anaemia." WHO, Health topics, anaemia
- 2
"Anaemia resulting from iron deficiency adversely affects cognitive and motor development, causes fatigue and low productivity and, when it occurs in pregnancy, may be associated with low birth weight and increased risk of maternal and perinatal mortality. In developing regions, maternal and neonatal mortality were responsible for 3.0 million deaths in 2013 and are important contributors to overall global mortality. It has been further estimated that 90 000 deaths in both sexes and all age groups are due to iron deficiency anaemia alone." WHO, The global prevalence of anaemia in 2011, pg. 1
- 3
IHME Global Burden of Disease tool, Dietary iron deficiency prevalence, 2017
- 4
See GiveWell, Steady-state Fortify Health iron fortification CEA, "FH (India) iron fortification" sheet, cells B64-B66.
- 5
See this page for a list of the intervention reports we have completed.
- 6
"Fortify Health is funding the premix and equipment provided to millers for cost-neutral fortification." Fortify Health, Branched activities of Fortify Health, pg. 3
- 7
"[Fortify Health is] working directly with millers to fortify wheat flour (atta) that will be sold on the open market." Fortify Health, Branched activities of Fortify Health, pg. 2
- 8
See Fortify Health, Blog, Introducing Fortify Health from October 2017.
- 9
"Fortify Health has secured partnerships with four industrial atta (wholewheat flour) mills in Maharashtra, all of which are relatively small and cater to a relatively more affluent consumer base. It is still in the process of establishing memorandums of understanding (MOUs) with the mills, although Fortify Health has already received verbal commitments and believes it is unlikely that any of the mills would not move forward." GiveWell's non-verbatim summary of a conversation with Fortify Health, March 13, 2019, pg. 2
- 10
"Since our last call, we have installed the microdoser in the [MH001] mill and signed an MOU with them. [MH001] staff have been inducted on the use of the equipment and produced the first batch of fortified flour for testing. They are now conducting lab tests and acquiring consumer feedback of the atta they have fortified. Once we have received these, we can roll out the fortified atta more widely. We anticipate a gradual phase-in of fortification to their products. [...] We have signed an MOU with the [MH002] miller, whose equipment will be installed in the next few weeks. He has agreed to launch a new product, which will be the atta we fortify. Once confidence is built in the product, we aim to expand fortification efforts into the rest of this mill’s products." Fortify Health, Update for GiveWell, April 15, pg. 2
- 11
See the Fortify Health, Miller scale up plan, sheet “Consensus Summary,” totals for columns “New mill partners (low bound)” and “New mill partners (high bound).”
- 12
- Fortify Health has about $100,000 in available funds left from the previous incubation grant it received. Fortify Health, second year budget draft (redacted), "2019-2020 Proposed Budget" sheet, row 54.
- The low bound scale-up would require an additional $475,079 (i.e. $575,079 total) in funding for one year. Fortify Health, second year budget draft (redacted), "2019-2020 Proposed Budget" sheet, Grand Total for column “Budget for Govt partnerships & Low Bound Plan Budget ($).”
- The high bound scale-up would require $830,780 (in total) for one year. Fortify Health, second year budget draft (redacted), "2019-2020 Proposed Budget" sheet, Grand Total for column “Budget for Govt partnerships & High Bound Plan Budget ($).” If Fortify Health chooses to pursue its high bound plan, the additional funding needed would be drawn from the funding we've allocated as an exit grant for the low bound scenario.
- 13
Fortify Health, second year budget draft (redacted), "2019-2020 Proposed Budget" sheet, Grand Total for column “Budget for Govt partnerships & Low Bound Plan Budget ($).”
- 14
- See Fortify Health, second year budget draft (redacted), "2019-2020 Proposed Budget" sheet, Grand Total for column “Govt Partnerships ($),” ($9,870 + $19,005 + $23,783 = $52,658).
- Potential government partnership opportunities include:
- providing fortified flour to ashram schools in two divisions of Maharashtra (ashram schools are government-managed residential schools for tribal communities),
- providing fortified flour for a safety net program in the public sector in a division of Maharashtra, and
- testing the quantity of iron in flour to provide diagnostic support to the public distribution system in West Bengal.
See GiveWell's non-verbatim summary of a conversation with Fortify Health, March 13, 2019. In this conversation in March 2019, Fortify Health told us it was considering working with millers to provide fortified flour to ashram schools in one division of Maharashtra. In their comments on a draft of this page, Fortify Health staff updated us that they were considering working in two divisions of Maharashtra.
- These funds largely comprise staff costs to investigate these opportunities; see Fortify Health, second year budget draft (redacted), "2019-2020 Proposed Budget" sheet, column “Govt Partnerships ($),” rows “Staff Salary” and “Staff Travel.”
- 15
GiveWell, Fortify Health Value of Incubation Grants, "FH (India) Iron fortification" sheet, cell B73.
- 16
See GiveWell, Fortify Health Value of Incubation Grants, "VoI Inputs" sheet, cell B14.
- 17
See GiveWell, Fortify Health Value of Incubation Grants, "FH (India) Iron fortification" sheet, cells B78.
- 18
See GiveWell, Fortify Health Value of Incubation Grants, "FH (India) Iron fortification" sheet, cell B77.
- 19
We have a high level of uncertainty about how much reallocated funding Fortify Health would be able to absorb effectively if it became a top charity; see below.
- 20
See GiveWell, Fortify Health Value of Incubation Grants, "VoI Inputs" sheet, cell B8.
- 21
- GiveWell, Steady-state Fortify Health iron fortification CEA, "Results - fortification" sheet, cell B4
- This analysis was done using the version of our cost-effectiveness model that was published in March 2019. Changes in our moral weights at the end of 2019 resulted in significant increases in many of our top charities' cost-effectiveness compared to cash transfers. See the cost-effectiveness figures for our top charities that are comparable with this estimate of Fortify Health's cost-effectiveness here.
- 22
This range of cost-effectiveness estimates is based only on what we believe to be the lower and upper bounds for the effect of iron fortification on the risk of iron deficiency (i.e. these bounds do not reflect uncertainties around other determinants of cost-effectiveness):
- For the lower bound, we assume that Fortify Health's program is no more effective than the average program in the Gera et al. 2012 meta-analysis. This is equivalent to inputting a value of 48% in cell B6 of GiveWell, Steady-state Fortify Health iron fortification CEA, "FH (India) Iron fortification" sheet.
- For the upper bound, we assume that Fortify Health's program is as effective as the average program in the Low et al. 2013 meta-analysis of iron supplementation programs. This is equivalent to inputting a value of 21% in cell B6 of GiveWell, Steady-state Fortify Health iron fortification CEA, "FH (India) Iron fortification" sheet (since in Low et al. 2013 the relative risk of iron deficiency with iron supplementation is 21%).
- 23
"The new standards lower the dose by an order of magnitude. This is not seen by experts to be an adequate dose to prevent neural tube defects." Fortify Health, responses to GiveWell questions, May 2019, pg. 4
- 24
See our very rough estimate of iron fortification's impact on perinatal maternal mortality here.
- 25
See GiveWell, Steady-state Fortify Health iron fortification CEA, "FH (India) iron fortification" sheet, cell B66.
- 26
"Antinutritional factors such as tannins and phytates in cereals have been found to negatively affect the bioavailability of minerals such as iron when consumed in large quantities." Delimont et al. 2017, pg. 2
- 27
"Ascorbic acid… is the most efficient enhancer of non-heme iron absorption when its stability in the food vehicle is ensured." Teucher et al. 2004, Abstract
- 28
"The factors that determine the proportion of iron absorbed from food... include the iron status of an individual." National Health and Medical Research Council, Nutrient Reference Values, Iron
- 29
GiveWell, Comparative level of iron consumption adjusted for absorption, "Comparative intake adjusted for absorption" sheet, cell B42.
- 30
GiveWell, Comparative level of iron consumption adjusted for absorption, "Comparative intake adjusted for absorption" sheet, cell B43.
- 31
See our intervention report on iron supplementation for school-age children.
- 32
We note that the meta-analysis that we rely on for the effect of iron fortification does not report baseline iron levels in each underlying study. We briefly looked at the studies included in the meta-analysis and our impression was that baseline iron levels were not reported in a consistent way across those studies, for example, some reported baseline serum ferritin levels, others baseline iron stores, and others baseline proportion who are iron deficient.
- 33
In brief:
- Our cost-effectiveness model currently assumes an even distribution of fortified flour consumption across beneficiaries; we think this is quite unlikely to be literally true (i.e. we believe some consumers likely consume significantly more or less than the average).
- If the relationship between iron intake and health benefits is linear, an uneven distribution of consumption across beneficiaries will not affect aggregate health benefits (as the loss in health benefits for one person is offset by the gain to another).
- Our understanding is that, in the absence of direct evidence, some academics tend to assume by default that the relationship between nutrient status and health effects is not linear and that, more specifically, severely deficient consumers generally receive more health benefits from their first incremental increase in nutrient level than their last. For instance, see Stein et al. 2005, pg. 22: "[I]f two individuals consume the same amount (dose) of a bioavailable micronutrient, the individual with the higher level of deficiency is expected to show a relatively bigger, positive response with regard to his or her health status than the individual with the lower level of deficiency."
- If the relationship between iron intake and health benefits is indeed concave in this way, it seems possible that some initially iron deficient people might consume a sufficiently large amount of iron that they are receiving limited (or no) benefits beyond a certain point, which would justify a downwards adjustment to our cost-effectiveness estimate.
- However, a concave relationship between iron intake and health benefits would also lead us to expect disproportionately larger health benefits (per unit of iron intake) for individuals who are consuming less than the average quantity of iron. This would suggest an upwards adjustment to our cost-effectiveness estimate. Determining how a) the drop-off in health benefits for people consuming more iron than average compares to b) the disproportionately greater health benefits for people consuming less iron than average, would require more detailed modeling than we've yet done of the actual distribution of fortified flour consumption and of the shape of the relationship between iron intake and health benefits.
- Additionally, it seems possible that consumers do not purchase and consume all their flour as fortified (if, e.g. they purchase from multiple markets, some of which may not stock fortified flour). This would mean that the average consumption per person is less than our model assumes, but that a proportionally larger number of beneficiaries are reached. Given a concave relationship between consumption and health benefits, this factor would also lead us to expect greater net health benefits overall.
- 34
"Some direct evidence of the ability of NaFeEDTA to prevent [phytates] action was obtained in an experiment where bran, a rich source of phytates, was shown to reduce the absorption of iron from ferrous sulphate eleven-fold. In contrast, no such inhibition occurred when bran was fed with NaFeEDTA…In contrast, when NaFeEDTA was given with tea, a seven-fold reduction in iron absorption was noted in one study, while in another tea reduce [sic] iron absorption from 11.5% to 1.86% when it was drunk with a low-extraction wheat roll fortified with NaFeEDTA", Bothwell and MacPhail 2004, pg. 423
- 35
See Food Safety and Standards Authority of India, Wheat Flour, "Standards" tab:
- "Atta, when fortified, shall contain added iron, folic acid and Vitamin B12 at the level given in the table below:"
- "Nutrient: Sodium Iron (III) Ethylene diamine tetra Acetate Trihydrate (Sodium feredetate-Na Fe EDTA): Level of fortification per Kg: 14mg - 21.25 mg"
- 36
- The WHO recommends 20 mg of iron per kg wheat flour when fortifying with the NaFeEDTA compound if a person is consuming 150-300 g of flour per day, and 40 mg of iron per kg of wheat flour if a person is consuming 149 g of flour per day or less. See WHO, Recommendations on Wheat and Maize Flour Fortification, pg. 2, Table 1.
- Fortify Health told us its best guess is that consumers in Maharashtra (where all four of Fortify Health’s current partner mills are located) consume on average 164 g of flour per day. Brendan Eappen, Fortify Health Executive Director, email to GiveWell, June 17, 2019
- In West Bengal, Fortify Health told us its best guess is that consumers consume an average of 49 g of flour per day (Fortify Health, Wheat Flour Fortification Programme in West Bengal). Our understanding is that Fortify Health bases this figure on the 2011-2012 Indian National Sample Survey of household consumption; we have not yet vetted this source ourselves.
- 37
"MP [Milling Partner] will provide a sample of fortified atta upon request and send it to an accredited laboratory selected by FH [Fortify Health] for testing at FH’s expense. The test results of the sample should show appropriate content of micronutrients." Fortify Health, Revised Miller MoU, pg. 6
- 38
A very rough model of the potential for excess iron intake might be:
- Fortify Health guesses that consumers in Maharashtra consume an average of 164 g of atta flour per day (Brendan Eappen, Fortify Health Executive Director, email to GiveWell, June 17, 2019).
- One website reports that there are about 339 calories in 100 g of wheat flour. 164 g * (339/100) = 556 calories in 164 g of wheat flour.
- A lean, physically-active adult male might consume 2500 calories per day, 4.5 times the calories in 164 g of atta (2500/556 ≈ 4.5).
- Assuming an upper limit of 2/3 of total dietary calories coming from atta, the rough upper bound intake would be (4.5 * 2/3) = 3x the average atta intake, or 492 g of atta (164 g * 3).
- Consuming 492 g of atta per day, fortified at 21.25 mg per kg of atta, would provide 10.46 mg (492 * 21.25/1000) of iron per day from the atta.
- 10.46 mg of iron is 1.74 times the 6 mg estimated average requirement (EAR) for iron intake for a young man. See National Health and Medical Research Council, Nutrient Reference Values, Iron, "Adults" table (under "Recommendations by life stage and gender").
- This calculation assumes that all of a consumer's flour intake is fortified. Additionally, our understanding is that the EAR is based on nutrient intake, not absorption, and we believe there may be higher than average absorption from NaFeEDTA.
- This calculation also doesn't take into account any additional iron intake from foods other than atta.
- 39
- "In 2018, Mr. Eappen deferred acceptance into medical school for one year in order to continue working for Fortify Health. He plans to continue working full-time through May of 2019. Although Mr. Eappen will likely no longer be involved in daily management and operations, he will continue to be involved in strategy and will remain in weekly contact with Ms. Patel and Dr. Bhattacharya." GiveWell's non-verbatim summary of a conversation with Fortify Health, March 13, 2019, pg. 2
- Our impression is that Urmi Bhattacharya, Fortify Health's current Country Director, will take on additional responsibility, but we are unsure of the details.
- 40
See GiveWell, Fortify Health Value of Incubation Grants, "VoI Inputs" sheet, cell B20.
- 41
- GiveWell's non-verbatim summary of a conversation with Fortify Health, September 18, 2018
- GiveWell's non-verbatim summary of a conversation with Fortify Health, December 14, 2018
- GiveWell's non-verbatim summary of a conversation with Fortify Health, March 13, 2019
- GiveWell's non-verbatim summary of conversations with Fortify Health, April 19 and 25, 2019