Table of Contents
What do they do?
The Carter Center onchcerciasis program distributes ivermectin to control or eliminate onchocerciasis.
- Elimination: 13 endemic areas in the Americas as well as parts of Uganda and Sudan (2008 River Blindness Program Report, Pg 2)
- Control: Nigeria, Ethiopia, Cameroon, Uganda, and Sudan (2008 River Blindness Program Report, Pg 2)
The Carter Center receives ivermectin for free from Merck, and follows the community-directed treatment with ivermectin process outlined here.1
Independent evidence of effectiveness
There is no debate that ivermectin effectively reduces the prevalence of the disease as measured by various diagnostic tests. However, there is little rigorous evidence that ivermectin, alone, reduces rates of blindness or skin disease (the debilitating conditions). To read our full report on ivermectin to control onchocerciasis, click here.
Internal monitoring
The Carter Center tracks several different indicators to evaluate the presence of onchocerciasis in each region. In the Americas, The Carter Center provides consistent monitoring in all areas in which they work.
In Africa, monitoring is much less consistent. The Carter Center provides multiple data points for its programs in Uganda and Cameroon; none for either or Ethiopia or Sudan; and, a report of one survey finding that prevalence in Nigeria fell significantly (from 51% to 3%) between 1992 and 1999.2
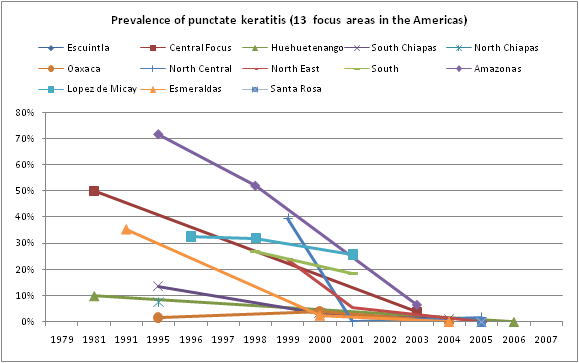
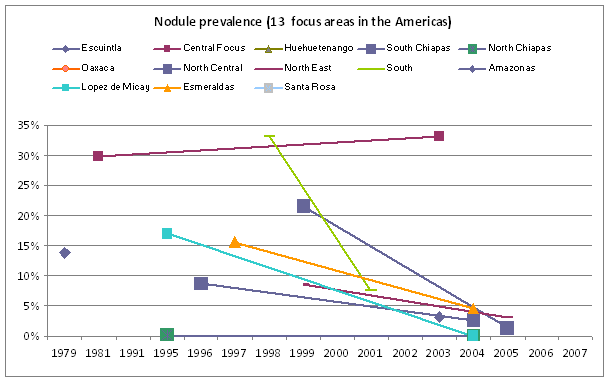
The Americas:
The charts below provides different measurements The Carter Center performed to monitor their progress in eliminating Onchocerciasis from the Americas. All show significant decreases in prevalence during the time Carter has worked in those areas.


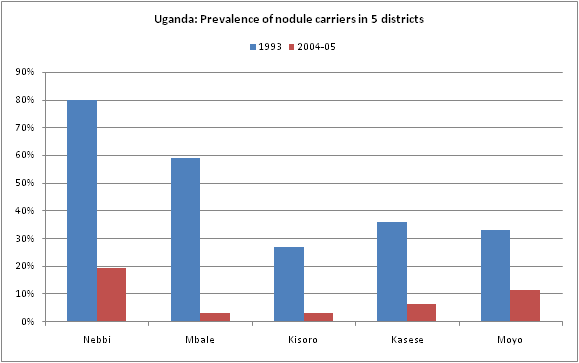
Africa
The charts below are representative of the results The Carter Center had in Cameroon and Uganda. Additional charts are available on our additional information page.

What do you get for your dollar?
The table below provides the number of cases of onchocerciasis worldwide that manifest with either blindness, low vision, or severe skin disease.
| Disease | Population ('000s): Africa | Population ('000s): Carter target area | Prevalence ('000s): Worldwide (Mathers 07) | Prevalence ('000s): Worldwide (Global Burden of Disease) | Prevalence ('000s): Africa (GBD) | Prevalence ('000s): Carter target area () | Incidence ('000s): Worldwide (Mathers 07) | New cases prevented in Carter area |
|---|---|---|---|---|---|---|---|---|
| Onchocerciasis, Africa | 700,000 | 10,800 | 2,296 | 910 | 891 | 14 | 141 | 2.2 |
Data sources:
- Mathers 07 is available online here, at PLoS NTDs
- The website for the 2004 update (published in 2008) of the Global Burden of Disease Project is here; we used the Excel file available here.
- Data for population served in The Carter Center's Onchocerciasis program comes from their 2008 River Blindness Program Report, Pg 8.
- Population of WHO Africa region comes from [[need source]]
This table provides our estimates of impacts and cost per dollar for Carter Center programs, assuming optimistically that they succesfully control all cases of onchocerciasis in Africa and eliminate onchocerciasis in the Americas. (We recognize these estimates are optimistic, but we don't have information to use regarding expected inefficacy.)
| Program | Estimated total cases averted per year | Estimated debilatating cases averted per year | Total cost | Cost per any case averted | Cost per debilitating averted | Long-term potential | Data sources and calculations |
|---|---|---|---|---|---|---|---|
| Onchocerciasis control | 1,000-4,200 | 500-2,100 (blindnesses, low visions, and severe skin diseases) | $1-2.5m/yr | $900-$2,250 | $1,800-$4,500 | None, control program | Source and calculation info |
| Onchocerciasis eliminitation, Americas | 850-3,400 | 425-1,700 | $42k - 420k per year | $12-500 | $25-1000 | Aim is elimination from the continent, making reintroduction unlikely. If this is successful, cost effectiveness would be substantially higher. | Source and calculation info |
| Onchocerciasis eliminitation, Uganda and Sudan | 66-260 | 33-130 | 67k-670k | $250-10,100 | $500-20,300 | Aim is elimination from the continent, making reintroduction unlikely. If this is successful, cost effectiveness would be substantially higher. | Source and calculation info |
We reached these conclusions as follows:
Control in Africa
- Estimated impact:
- Africa accounts for 98% of the onchocerciasis global burden of disease (Table 1).
- There are 141,000 new cases of blindness, low vision, and severe skin disease due to Onchocerciasis each year. (Table 1)
- Given that 98% of the burden is in Africa, there are 138,000 new cases in Africa.
- The Carter Center serves a population of 10.8 million people (2008 River Blindness Report, Pg 8), approximately 1.5% of the population of Africa (10.8m/700m).
- Given that The Carter Center serves 1.5% of the population of Africa, it seeks to prevent approximately 2,070 cases of River Blindness annually.
- While there's strong evidence that providing ivermectin once per year reduces onchocerciasis infection we don't know either a) what portion of expected future cases it averts (i.e., whether it averts 50% or 100% of cases) or b) whether reducing infection rates ultimately leads to reduced incidence of debilitating conditions. (For more information, see our detailed review of the effectiveness of this intervention here.) Given these unknowns we use a wide effectiveness range of 25% to 100% effectiveness.
- Cost:
- Carter Center data: The 2008 River Blindness Program Report publishes the total cost (including contributions by The Carter Center, local ministries of health, and the African Program for Onchocerciasis Control (APOC)) in Nigeria (Pg 76), Uganda (Pg 39), and Cameroon (Pg 60). No cost data is provided for Sudan or Ethiopia. Total annual costs from the three countries that do provide data are approximately $1.25 million. Ethiopia accounts for close to 25% of the total program and Sudan's is around 1% (in terms of treatments distributed -- see 2008 River Blindness Program Report, Pg 8). Assuming that Ethiopia and Sudan account for 25% of the total cost means that the total cost for the Onchocerciasis control program in Africa is approximately $1.66 million.
- Other data: Estimates of the cost per person treated of MDA programs in Africa, assuming donated drugs which this Carter Center program has, tends to $.06-.54 per person treated (see our review of costs for lymphatic filariasis here for more information.) The DCP estimates that the cost per person treated for the combination deworming package of PZQ and albendazole costs $.25 per person treated (see our report on schistosimiasis here). In 2007, The Carter Center treated approximately 5 million people in this program (2008 River Blindness Report, Pg 8). Given this cost per person treated, that yields a total cost range of $300,000-2.7 million.
- It's also worth noting that this Carter Center program shares distribution and likely organizational oversight with other MDA programs, particularly in Nigeria. This likely reduces the cost for each relative to what they would be alone.
- Cost per impact: With costs of $1-2.5m annually, we estimate that this program averts one case of debilating blindness, low vision or skin disease for every $1,838-4,596 spent.
Elimination program in the Americas
We use the approximately the same cost and impact estimates for this program as we for Africa control. We double costs ($.10-$1.00 vs $.05-$.50) because elimination requires 2 doses, rather than 1, each year.
Elimination program in the Americas
- Impact:
- Change in prevalence: The 2008 River Blindness Program Report, Pg 22 provides baseline and current prevalence rates of Onchocerciasis in The Carter Center's focus areas where Carter reduces prevalence rates from 65,000 to 8,000 over 13 years (1995-2008).
- Total population served: 2007 River Blindness Program Report, Pg 21. These figures, along with the % change in prevalence, let us compute the approximate change in the total number of cases.
- Assuming that the same incidence:prevalence ratio holds in the Americas as Africa (6%), we can estimate that The Carter Center is now preventing 3,400 cases of onchocerciasis per year.
- The data we have worldwide only presents the number of debilitating cases of onchocerciasis, while the data from The Carter Center for the Americas presents the total number of cases. We use a basic population interpolation to estimate the number of debilitating cases. In Carter Center focus regions in Africa, there are 10.8m people and approximately 900,000 debilitating cases of onchocerciasis (8%). Assuming the same ratio holds in the Americas, there would have been approximately 33k debilitating cases pre-treatment (roughly half of those infected). This means that the Carter Center aims to avert 1,700 cases per year. Given that we don't have strong evidence regarding what portion of cases this program will avert (see above), we use a range of 25-100%, giving us a range of 425-1700 cases averted annually.
- Elimination: The Carter Center is aiming to eliminate this program which could mean that the long-term effects of the program could be much higher.
- Cost:
- Assuming a similar cost-effectiveness range to other MDA (see above discussion in the section on onchocerciasis control in Africa), the cost per person treated would be approximately $.10-1.00. (We double costs because elimination requires 2 doses, rather than 1, each year.)
- In 2007, The Carter Center treated approximately 420,000 people in the Americas. (2008 River Blindness Program Report, Pg 8)
- That would present a total cost of $42-420k.
- Cost per impact: With expenses of $42-420k and severe cases averted of 425-1700, we estimate that The Carter Center averts a severe case of river blindness for $25-1000. [[This is way lower than the Africa estimate. That's because prevalence of oncho in this region was way higher: 33k/420k (25%) as opposed to 890k/700m (.1%). That means I must've done something insane. Not sure what. If the particular areas of Africa here TCC works are more prevalent than average for Africa -- quite likely -- my TCC Africa estimate would be too high.]]
- 1
See 2008 River Blindness Program Report, Figure G. The Carter Center plays a role in training the community directed distributors. The report is available online at http://cartercenter.org/resources/pdfs/news/health_publications/river_b…, accessed 2/20/09.
- 2
See 2005 River Blindness Report, Pg 37. Available online at http://cartercenter.org/documents/2250.pdf, accessed 2/20/09.