Combined Protocol Community-Based Management of Acute Malnutrition - July 2021 Version
We have published a more recent version of this page. See our most recent version of this page.
Summary
- What is the program? Globally, 47 million children are estimated to have experienced moderate or severe acute malnutrition in 2019, which is hypothesized to raise their risks of developmental delays and death. Community-based management of acute malnutrition (CMAM) using a combined protocol identifies and treats cases of uncomplicated malnutrition on an outpatient basis, primarily through the provision of ready-to-use therapeutic food (RUTF). Unlike standard CMAM programs, CMAM programs using combined protocols treat children with both severe acute malnutrition (SAM) and moderate acute malnutrition (MAM) using the same food product and aim to treat more children, earlier on, before they reach the severe stage of acute malnutrition. CMAM programs also treat malnourished children with standard medications, including a short course of antibiotics (most commonly amoxicillin) for children with SAM.
- What is its evidence of effectiveness? We are not aware of any studies which estimate the effect of CMAM in comparison to a truly untreated control group. However, providing malnourished children with food and treating potential infections is a straightforward mechanism through which we believe it is highly plausible that the program would reduce mortality, our primary outcome of interest. To estimate the magnitude of the effect of CMAM on mortality, we combine data on mortality rates among children with SAM and MAM who do not receive treatment, based on historical studies, with data on rates of recovery and relapse within contemporary CMAM programs. We also find it plausible that treating malnutrition would reduce developmental delays, although direct evidence for CMAM’s effects on incomes in adulthood is also lacking.
- How cost-effective is it? Our cost-effectiveness analysis suggests that combined protocol CMAM is in the range of cost-effectiveness of programs we would consider directing funding to. We find it plausible that CMAM would substantially reduce under-5 mortality from malnutrition, which is an outcome we value highly. However, the costs of implementing CMAM, which strongly influence our cost-effectiveness estimates, vary widely depending on program contexts. In addition, we are highly uncertain about the magnitude of the primary benefits (decreased mortality) and secondary benefits (increased income in adulthood) we model.
- Does it have room for more funding? We have not yet completed a full analysis of this question, but our understanding from speaking with charities working on these programs is that there is likely to be substantial room for more funding due to a large remaining global need.
- Bottom line. We believe this intervention is plausibly cost-effective despite uncertainties about program costs and its effects on mortality. We are investigating specific charities' programs as potential giving opportunities. We expect that learning more about what treatment options are available in the absence of NGO support could give us more confidence in our assessment of the costs and benefits of implementing CMAM in specific contexts.
Published: July 2021
Previous versions of this page:
Table of Contents
What is the problem?
Acute malnutrition refers to "wasting" (low weight-for-height caused by rapid weight loss or failure to gain weight)1 and/or the presence of nutritional edema (swelling caused by excess fluid retention)2 and is associated with heightened risks of morbidity and mortality.3 Moderate acute malnutrition (MAM) is characterized by low weight-for-height or mid-upper arm circumference.4 Severe acute malnutrition (SAM) is characterized by very low weight-for-height, very low mid-upper arm circumference, and/or the presence of nutritional edema.5 If the underlying causes are left untreated, the condition of a child with MAM may become more severe and cross the threshold into SAM.6
Globally, it is estimated that about 47 million children under five experienced moderate or severe wasting in 2019, with 14.3 million of those experiencing severe wasting.7 Assessments of malnutrition’s effects on mortality draw on historical studies, and thus are uncertain (see discussion here). In addition, it is hypothesized that malnutrition can cause cognitive developmental delays that could impair functioning in adulthood among children who survive.8
What is the program?
CMAM programs using a combined treatment protocol seek to avoid some of the limitations of standard CMAM programs by using a simplified protocol and single food product to diagnose and treat children with both SAM and MAM, reducing the complexity of implementation for healthcare practitioners and preventing children with MAM from progressing to SAM.
The national CMAM treatment protocols that we've seen include treatment of both MAM and SAM but recommend different treatment strategies for each. Uncomplicated cases of SAM are treated with ready-to-use therapeutic food (RUTF), an all-in-one food product that is designed to provide malnourished children with the nutrients they need to recover,9 along with a course of antibiotics.10 The MAM component of CMAM protocols relies on the use of ready-to-use supplementary food (RUSF) or enriched flours.11
There are no globally accepted guidelines for treating MAM, and in areas of scarce resources, moderately malnourished children may not receive treatment at all.12 This raises the concern that without treatment, a portion of children with MAM will progress to SAM.13 Adding to the complexity for healthcare practitioners who encounter both types of malnutrition, UNICEF supports treatment of SAM with provision of RUTF, whereas the World Food Programme supports treatment of MAM with a different product, ready-to-use supplementary food (RUSF).14
Recently developed combined protocols for CMAM treat children with both SAM and MAM using RUTF.15 These combined protocols aim to expand coverage by reducing the complexity of implementation for healthcare practitioners, as well as reducing the dosage of RUTF given to each child, which reduces treatment costs per child.16 By expanding admission criteria for CMAM programs to MUAC less than 125mm (rather than less than 115mm),17 combined protocols aim to treat more children, earlier on, before they reach the severe stage of acute malnutrition.18 CMAM programs using combined protocols treat both MAM and uncomplicated SAM in an outpatient setting.19 Currently, the World Health Organization recommends that children with uncomplicated SAM be managed as outpatients in community clinics20 (as opposed to previously used hospital-based treatment)21 and receive a seven-day course of antibiotics, due to the risk of covert infection.22
Recent and planned trials are testing slightly different combined protocols,23 but broadly these programs involve:
- Identifying SAM and MAM in the community, often by using community health worker networks or by training caregivers (usually mothers) to screen children using colored plastic strips to measure mid-upper-arm circumference (MUAC).24
- Assessment of children who meet the criteria for SAM or MAM and referrals to inpatient care for those children who are deemed too sick to treat via CMAM.25
- Providing a standardized set of medical treatments26 for SAM children, including a course of amoxicillin to reduce infections, speed up nutritional recovery, and prevent mortality.27
- Providing ready-to-use therapeutic food (RUTF), a nonperishable, calorie- and micronutrient-dense food designed for treating malnutrition until children meet criteria for discharge. The combined protocols generally provide a lower dosage of RUTF than standard protocols, in order to expand coverage while still providing enough nutrition for children to recover.28
While we focus on combined protocol CMAM in this report, there is substantial overlap in the evidence for standard and combined protocol CMAM. We model both variants in our cost-effectiveness analysis.
Does the program have strong evidence of effectiveness?
We have not found direct evidence establishing the magnitude of CMAM’s reduction in under-5 mortality, which is our primary outcome of interest.29 However, treatment of malnutrition has a highly plausible and straightforward mechanism of action. Malnutrition is hypothesized to reduce immune function, rendering children more susceptible to death from infection.30 RUTF addresses nutritional deficiencies, while antibiotics treat subclinical infections and may also work through less well-understood pathways, such as reducing inflammation.31 We also believe the standard care that is typically provided at initiation of CMAM, such as screening and treatment for malaria and preventative vaccines, is likely to be beneficial. Overall, we have a strong prior that CMAM will avert deaths among malnourished children to some extent. In addition, trial evidence shows effects of individual components of combined protocol CMAM on identification of malnourished children, improved recovery, and reduced mortality (discussed here for the sake of brevity). Therefore, we believe CMAM is promising despite substantial uncertainty about its total effects.
We estimate CMAM’s effect on mortality by combining data from:
- Pooled analyses that use historical studies to establish how malnutrition affects risk of mortality when it is untreated; and
- Reported recovery rates in contemporary CMAM programs.
We make a number of adjustments to address discrepancies between historical and contemporary conditions, as well as relapse rates following CMAM programs and eventual mortality.
We also find it plausible that treating malnutrition would reduce developmental delays, although direct evidence for CMAM’s effects on incomes in adulthood is lacking.
Counterfactual mortality in the absence of CMAM
To estimate the effect of untreated malnutrition on mortality, we draw on a pooled analysis of longitudinal studies that took place before CMAM was established practice. This analysis provides estimates (hazard ratios) of how much more likely malnourished children are to die than non-malnourished children. These estimates have a number of limitations:
- They use observational data, raising concerns of confounding factors;
- Children with complicated SAM could have been included in these samples; and
- Child mortality and the prevalence of and treatment for diseases were different in historical contexts than in contemporary program contexts.
We make adjustments to the hazard ratios to account for these factors, though we have substantial uncertainty about these adjustments. We multiply the adjusted hazard ratios by a recent estimate of annual mortality for non-malnourished children in order to calculate contemporary annual mortality for malnourished children in the absence of treatment.
Our starting point to estimate mortality among untreated malnourished children comes from Olofin et al. 2013, which pools results from 10 longitudinal studies, including five randomized controlled trials (RCTs) of vitamin A supplementation and five prospective cohort studies that recruited participants in the 1970s, 1980s, and 1990s.32 While children exhibiting signs of severe illness were referred for medical treatment in some of these studies,33 the studies were not designed to treat acute malnutrition. Resulting pooled estimates find that mortality rates for children with SAM are 11.6 times as high as for non-wasted children, whereas those for children with MAM are 3.4 times as high.34
We adjust the Olofin et al. 2013 estimates to account for the following factors:
Confounding. We expect that children might be malnourished as a result of causally prior risk factors that also increase their risk of mortality and that treatment for malnutrition does not address. We therefore adjust the hazard ratios (HRs) for SAM and MAM downward.
- Measured confounding
- Olofin et al. 2013 reports that adjusting for covariates using the six studies that report detailed baseline characteristics has little effect on estimated HRs.35 However, an earlier analysis (Black et al. 2008) found that including covariates in two historical studies resulted in reduced estimates of increased mortality risk due to malnutrition. Averaging across these two studies, they estimated that 15% of observed higher risk among malnourished children is actually due to socioeconomic factors.36
- Because we find it implausible that confounding would not be an issue, we follow Black et al. 2008 and decrease the HRs for SAM and MAM by 15% to account for measured socioeconomic confounding.
- Unmeasured confounding. We also adjust for factors that were not measured in baseline covariates and that we believe could bias our estimates of counterfactual mortality.
- Geographic remoteness: Living in a remote area could make malnutrition more likely (e.g., because the household lacks access to markets) and also drive mortality (e.g., because it’s difficult to get to a health facility to get treatment for other illnesses, such as malaria). Although we have not reviewed the covariates used in one of the two studies in Black et al. 2008, the other study does not include any measure of remoteness.37
- Selection into CMAM treatment or successful completion of CMAM treatment: As discussed in the next section, we model CMAM as averting deaths exclusively among children who are “discharged as recovered.” Other outcomes for treated children include defaulting, not responding to treatment, and dying.38 It seems likely that counterfactual mortality risk is not evenly distributed among these groups and that those who do not recover have higher counterfactual mortality risks. This could be the case for socioeconomic reasons (e.g., because families that cannot afford for caregivers to take time off work to bring children to treatment are more likely to default and this lack of resources also independently increases mortality risks) or because sicker children are more likely to reject RUTF, making their caregivers less likely to bring them back for treatment.39 Conversely, the recovered population likely has lower counterfactual mortality risk than the malnourished group as a whole. Failing to adjust for these differences could overestimate the benefit of CMAM.
- Other unmeasured factors: Given the relatively sparse baseline data, we think it likely that there are additional confounding factors beyond those listed here.
- We guess that bias resulting from these unmeasured factors is double the size of measured bias and thus include an additional 30% reduction to the HRs for SAM and MAM to account for unmeasured confounding.
Severity of SAM. CMAM treats children with uncomplicated severe acute malnutrition, but historical studies don’t allow us to distinguish between children with uncomplicated and medically complicated SAM. Because the inclusion of medically complicated cases might overestimate the counterfactual mortality rate, we adjust the HR for SAM downward.
- Our understanding is that one of the benefits of treating uncomplicated SAM is the opportunity to cure children before they develop a complicated illness.40 We expect that in the absence of treatment, some portion of children with uncomplicated SAM would go on to develop complications and that it is appropriate to include these cases when estimating counterfactual outcomes absent treatment.
- On the other hand, we expect that children who already had complicated cases of SAM at the time of enrollment in the study would have higher counterfactual mortality rates than children with uncomplicated SAM who are eligible to be treated in CMAM programs.
- To address this, we subtract deaths that could be attributed to complicated SAM cases under a series of simplifying assumptions. This results in a reduction of approximately 9% to our estimate of the HR for uncomplicated SAM.41
Changes in mortality rates and disease risk. We calculate counterfactual mortality rates by multiplying the adjusted hazard ratios by an estimate of the current annual mortality rate for non-malnourished children. Under-five mortality rates have dropped substantially in recent decades.42 Assuming the original HRs are accurate, then to the extent that drivers of reduced mortality are equally common and have similar effects among malnourished and non-malnourished children, simple multiplication of the current non-malnourished mortality rate by the historical HRs should generate an accurate malnourished mortality rate. We adjust the HRs upward to account for the possibility that drivers of reduced mortality are more concentrated and have larger effects in the non-malnourished population.
- Declines in particular diseases over time: Decreases in the prevalence of certain diseases have contributed to drops in mortality. All else equal, if the increased mortality risk malnourished children face from the illnesses that have declined over time is lower than the increased mortality risk they face overall, this could bias the contemporary mortality estimates downward. In addition, if the decline in diseases is concentrated among non-malnourished (as opposed to malnourished) groups, this could also bias mortality estimates downward.
- Olofin et al. 2013 reports cause-specific HRs (factors that represent the increased risk malnourished children face of dying of specific diseases) for five sets of diseases (respiratory tract infections, diarrheal disease, other infectious causes, malaria and measles). Four of these have lower cause-specific HRs than the all-cause HR (the factor that represents the increased risk malnourished children face of dying overall) and have declined substantially in incidence since the historical studies.43
Only diarrheal disease has a greater cause-specific HR for SAM than the all-cause HR.44
Incidence of diarrheal disease has decreased much less since 1990 than incidence of the other sets of diseases.45
This makes us inclined to believe that the simple multiplication method would underestimate counterfactual mortality rate, because the largest changes in incidence are for diseases with cause-specific HRs lower than the all-cause HR. But because we believe there is likely to be quite significant measurement error in attribution of cause of death in historical studies,46
we do not weigh this evidence very heavily.
- In addition, it seems likely that declines in incidence of these diseases are more concentrated among non-malnourished children. First, we expect that socioeconomic factors (e.g., resource constraints, distance from larger towns, etc.) drive both malnourishment and lack of access to disease prevention measures such as vaccines.47 Second, because of the cycle between infection and malnutrition, we expect those children who are exposed to infections without adequate treatment are more likely to become malnourished.48 Greater declines in disease incidence among the non-malnourished population would also lead to an underestimate of the counterfactual malnourished mortality rate.
- Declines in mortality due to improved treatments. Beyond preventative health measures, some of the decline in mortality rates may be due to improved treatments for illnesses.49 As with prevention, we think these gains are likely to be less concentrated among malnourished children because of socioeconomic factors (e.g., resource availability, distance from health facilities) that make it difficult to seek early and/or effective treatments for illnesses. If gains from better treatment options are concentrated among the non-malnourished population, then simple multiplication will underestimate the counterfactual malnourished mortality rate.
- Overall, we think it likely that simply multiplying an estimate of contemporary non-malnourished mortality by historical HRs is likely to underestimate the true malnourished mortality rate in the counterfactual, because we think that drivers of reduced mortality are likely to be disproportionately concentrated among non-malnourished children. We adjust for this by increasing the hazard ratios for both SAM and MAM by 10%, but this is a highly uncertain adjustment. We may revisit this adjustment if we obtain information on access to prevention and treatment care among malnourished populations served by a particular program that we are considering directing funding to.
After adjusting the HRs to account for confounding, complicated SAM cases, and reduced disease risk, our best guess is that children with SAM have mortality rates 6.9 times those of non-malnourished children, while children with MAM have mortality rates 2.2 times those of the non-malnourished group.50 Combining this with an estimated mortality rate for non-malnourished children in Niger yields an estimated annual SAM mortality rate of 13.8% in the absence of treatment. For comparison, this rate is about 83% of the average mortality rate of 16.6% in a WHO analysis using five historical studies to estimate mortality rates for children with SAM.51 We estimate a counterfactual MAM mortality rate of 4.4%. We used estimated mortality rates from Niger because it was a context in which we were considering directing funding for treatment of malnutrition. In December 2020, we recommended a grant to the Alliance for International Medical Action (ALIMA) to support its malnutrition work in Mirriah, Niger, part of which will fund combined protocol CMAM as part of an RCT.
Effects of CMAM on mortality
In order to estimate the deaths averted by CMAM, we begin with the assumption that children who are “discharged as recovered” from treatment programs face the same mortality risk as non-malnourished children.52 Stopping there would overestimate deaths averted because a subset of children relapse into malnourished states after they recover and face associated mortality risks. We adjust our estimate of deaths averted to reflect these eventual deaths after relapse.
- Rates of recovery. Our understanding is that recovery rate is a standardized CMAM program indicator that represents the proportion of program participants who are discharged as recovered out of the total number of participants discharged.53
Our understanding is that CMAM programs show significant variability in rates of recovery, usually driven primarily by variation in the rates of children defaulting from treatment.54
Trials of combined protocols are designed to test that recovery rates are non-inferior to those achieved with standard protocols;55
however, recovery rates may still differ under these protocols in operational settings. Because of these sources of variability, although we use figures reported in the literature for our current analysis, we plan to use program data for these quantities when investigating a particular giving opportunity.
- SAM Recovery Rates. We estimate that approximately 79% of CMAM program participants with SAM are discharged as recovered, based on a systematic review.56
- MAM Recovery Rates. We estimate that approximately 82% of CMAM program participants with MAM are discharged as recovered, based on the average recovery rate reported in a meta-analysis of studies on treatment of children with MAM.57
- Using rates of recovery could underestimate the benefits of CMAM to the extent that caregivers “self-discharge” their children and choose not to incur the costs of returning to health clinics once they perceive their children to be well, such that some children who have recovered are recorded as having defaulted.58 While this is a theoretical possibility, we guess this is a small enough proportion of defaulters that excluding them does not meaningfully underestimate CMAM’s benefits. We might revise this assumption given data to the contrary from a particular program context.
- Risk of relapse. A subset of children treated will relapse and eventually die of malnutrition-related causes during early childhood. We extrapolate from a systematic review of studies that followed children after they received treatment from CMAM programs to estimate that 44% of those discharged as recovered will relapse into malnutrition.59 We make the simplifying assumptions that children will relapse into the same condition they were originally treated for (SAM or MAM), receive an additional round of treatment,60 and face the average treated mortality risk of that condition. This yields an assumption that about 1% and 2% of children treated for MAM and SAM respectively whose deaths were initially averted will eventually die as a result of malnutrition.61 We do not count these deaths following relapse as averted. Because mortality risk from malnutrition diminishes with age,62 we believe this assumption is likely to underestimate the benefits of treatment.
What is the evidence of effects on adult income?
We are not aware of any studies that seek to measure the effects of receiving CMAM in childhood on income in adulthood. However, there is a large body of research that is broadly consistent with the idea that early childhood growth restrictions inhibit development, which in turn negatively affects outcomes in adulthood (GiveWell reviews this literature here). A recent systematic review found small but significant pooled effects of nutrition supplementation interventions on measures of cognitive, language, motor, and social-emotional development.63 We view this evidence as consistent with CMAM (and specifically RUTF) increasing income in adulthood by improving early childhood development and include increased income in adulthood as a benefit in our cost-effectiveness analysis.
Potential adverse effects
Although sustained antibiotic resistance following administration of amoxicillin was not observed in a study following SAM children,64 we consider the potential for antibiotic resistance to be the most serious potential adverse effect of this program. Short-term side effects resulting from antibiotics or RUTF appear rare and relatively mild. Long-term side effects are potentially more serious, but we believe they are strongly outweighed by the benefits of reduced mortality.
- Antibiotic resistance. Resistance to amoxicillin has been observed to be high in Africa. Specifically, high levels of resistance to amoxicillin have been observed in the bacteria that causes pneumonia, a common cause of childhood death, making resistance to amoxicillin an urgent public health priority.65 However, in a study of children with SAM who were administered oral amoxicillin and then followed for two years, sustained antibiotic resistance was not observed.66 We believe based on this evidence that the benefits of treatment with amoxicillin in this case outweighs the substantial risks. We have included an adjustment to try to account for this in our cost-effectiveness model and will continue to investigate this question.
- Short-term side effects. A systematic review using data from three studies comparing RUTF to other foods found no difference in risk of adverse events (including cough, diarrhea and fever).67 Three out of 2,767 children treated in the Malawi study of antibiotics described above reported adverse drug reactions including rash, thrush, and bloody diarrhea.68 The trial in Niger did not report on allergic reactions or adverse drug reactions. In general, common side effects of amoxicillin, the most commonly used antibiotic for treatment of uncomplicated SAM, are diarrhea, rash, vomiting, and nausea.69
- Long-term side effects. Antibiotic exposure in childhood has been linked in observational studies to increased risk of asthma and allergies70 and overweight and obesity.71 In addition, the long-term effects of use of RUTF are not well-studied, and some hypothesize that RUTF may increase risk of obesity and associated diseases.72 We believe these risks are outweighed by potentially substantial benefits but have included an adjustment in our cost-effectiveness analyses to attempt to account for them.
How cost-effective is it?
Our cost-effectiveness analysis for a combined protocol CMAM program in which caregivers are trained to screen for malnutrition suggests that it is in the range of cost-effectiveness of programs we would consider directing funding to.73
We also model the cost-effectiveness of the standard CMAM program (which treats children with SAM but not MAM) and find it to be slightly below the range of programs we would consider directing funding to, but close enough to that range that it seems plausible additional information could change our view.74
We are highly uncertain about the number of under-5 deaths CMAM programs avert, which is the biggest driver of benefits in our model. We also expect costs per child, which strongly influence cost-effectiveness, to vary significantly across program contexts.75
Note that our cost-effectiveness analyses are simplified models that do not take into account a number of factors. There are limitations to this kind of cost-effectiveness analysis, and we believe that cost-effectiveness estimates such as these should not be taken literally due to the significant uncertainty around them. We provide these estimates (a) for comparative purposes and (b) because working on them helps us ensure that we are thinking through as many of the relevant issues as possible.
As we consider particular funding opportunities, we anticipate substantial change to our cost-effectiveness model because we expect to use (i) a counterfactual of government-only treatment (without NGO support) as opposed to the counterfactual of no treatment currently used in the model and (ii) costs from a particular program.
A sketch of the key components of the cost-effectiveness model is below. Throughout, we use baseline data from Niger, a country to which we have previously directed funding to treatment of malnutrition programming76 and in which we see potential for directing additional funding to CMAM programs. If necessary, we will update these components of the model when we consider directing funding to particular programs.
- Costs: We estimate a program cost of about $900,000 for every 100,000 caregivers trained. This cost includes the cost of training caregivers to identify MAM and SAM and bring their children in for treatment ($0.40 annually per caregiver), as well as a portion of the costs of CMAM itself. This excludes the cost of RUTF which we estimate to be about $430,000 and which we expect would be financed by UNICEF.
- Number of children brought in for treatment: We estimate that for every 100,000 caregivers trained, roughly 6,200 children with MAM and 2,700 children with SAM would be brought in for treatment.
- Probability of death: We estimate that 4.4% of those with MAM and 13.8% of those with SAM would die without treatment.
- Efficacy of treatment: We estimate treatment would lower the probability of death by about 46% for children with SAM and 25% for children with MAM, once we account for deaths following relapse and internal and external validity concerns.
- Additional benefits from immediate consumption and development effects and other adjustments: We estimate consumption and development benefits add 35% and downside adjustments, inclusion/exclusion, and leverage/funging reduce benefits by 20%.
Overall, we estimate that combined protocol CMAM is within the range of cost-effectiveness of programs we would consider recommending funding.
However, we have high uncertainty about program costs, mortality reductions, and developmental effects.
- Cost of the program. Costs per child treated strongly influence cost-effectiveness, and we believe costs of CMAM programs vary widely. We expect to have access to more accurate program cost data when investigating particular giving opportunities.
- Mortality reductions from CMAM. There exists very limited evidence on the effect of CMAM on mortality. We expect we could gather reliable data about recovery rates given treatment within a particular program context. However, because of ethical restrictions on studying untreated malnourished children, we expect that counterfactual mortality rates will remain an area of persistent uncertainty for us.
- Increase in consumption resulting from increased early-life growth. Our model assumes that increases in child growth will cause increases in adult consumption/income. The data that underlie this assumption are from studies of birth weight differences between identical twins and are highly uncertain in this context.
- Less influential uncertainties. We also have uncertainties about mortality rates among those who relapse and adjustments for excluded effects, but in sensitivity analyses, these factors have a smaller influence on overall cost-effectiveness.
Does the program have room for more funding?
We have not yet completed a full analysis of this question, but our understanding is that there is likely to be substantial room for more funding due to a large remaining global need.77
In January 2021, ALIMA received a GiveWell Incubation Grant of roughly $1 million to support its work on treatment of malnutrition and pediatric emergencies, which we anticipate will allow us to learn more about CMAM as a program and ALIMA’s room for more funding.
Key questions for further investigation
Questions we plan to ask as part of further investigation include the following:
Counterfactuals and mortality estimates
- What are coverage and recovery rates for CMAM programs run exclusively by governments versus those that also have support from NGOs?
- How does the combined protocol change the number and risk profile of hospitalized children with SAM? How can we best incorporate inpatient care (including transfers from CMAM) into our cost-effectiveness analysis?
- Is there any other evidence that can help us to triangulate a narrower range of plausible values for the effect of CMAM on mortality?
- What can we learn from a deeper investigation of the historical studies used to estimate mortality from malnutrition, such as whether those estimates are sensitive to the inclusion of additional studies and/or the set of covariates included to adjust for confounding?
- What proportion of recovered children relapse and ultimately die of malnutrition?
Costs
- What are the costs of a scaled-up combined protocol CMAM program in a particular charity's setting?
- What proportion of malnourished children require more than one round of CMAM, and how many additional rounds of treatment do they require on average?
- How much funding do governments typically contribute to malnutrition treatment and how would this funding scale with increased coverage?
Other areas for investigation
- Do the two combined protocols78 currently being tested perform equivalently or is one superior to the other in terms of child outcomes and/or cost-effectiveness?
- What are the longer-term outcomes for children who recover from malnutrition? Are there any permanent impacts of a temporary period of malnutrition on later-life outcomes? Should we account for incomplete nutritional recovery in our model?79
- What are the costs associated with antibiotic resistance?
- Does cost-effectiveness vary between settings where children are chronically malnourished as opposed to malnourished due to a temporary crisis?80
Our process
We performed an in-depth literature review of studies related to mortality from malnutrition with and without treatment. We performed a medium-depth literature review to find studies related to individual components of CMAM and published estimates of costs of CMAM programs. We have had initial research calls with approximately seven organizations that implement CMAM programs.
Sources
{kind=link}
- 1"Wasting refers to a child who is too thin for his or her height. Wasting is the result of recent rapid weight loss or the failure to gain weight." UNICEF, WHO, World Bank, "Joint child malnutrition estimates — levels and trends," 2020, pg. 2.
- 2“Acute malnutrition is a major public health issue in low-income countries. It includes both wasting and edematous malnutrition, but the terms wasting and acute malnutrition are often used interchangeably." Frison, Checchi, and Kerac 2015, Abstract.
- 3
- "Restricted growth as a result of inadequate nutrition and infections is an important cause of morbidity and mortality in infants and children worldwide. . . . Several prospective studies have shown associations of undernutrition with increased risk of various disease outcomes, and reduced survival, in children." Olofin et al. 2013, Introduction.
- "All degrees of underweight, stunting and wasting were associated with significantly higher mortality. The strength of association increased monotonically as Z scores decreased. Pooled mortality HR was 1.52 (95% Confidence Interval 1.28, 1.81) for mild underweight; 2.63 (2.20, 3.14) for moderate underweight; and 9.40 (8.02, 11.03) for severe underweight. Wasting was a stronger determinant of mortality than stunting or underweight." Olofin et al. 2013, Abstract.
- 4"In children aged 6–59 months, moderate acute malnutrition is defined as moderate wasting (i.e. weight-for-height between –3 and –2 Z-scores of the WHO Child Growth Standards median) and/or mid-upper-arm circumference (MUAC) greater or equal to 115 mm and less than 125 mm." WHO, "Supplementary foods for the management of moderate acute malnutrition in children aged 6–59 months," 2019.
- 5
- "Severe acute malnutrition (SAM) is defined as a weight-for-height measurement of 70% or more below the median, or three SD [standard deviations] or more below the mean National Centre for Health Statistics reference values (that will likely be replaced by new WHO growth curves), which is called "wasted"; the presence of bilateral pitting oedema of nutritional origin, which is called "oedematous malnutrition" or a mid-upper-arm circumference of less than 110 mm in children age 1–5 years." Collins et al. 2006, pg. 1.
- In 2009, WHO recommended increasing the MUAC cut-off point for defining SAM from 110 mm to 115 mm. "WHO standards for mid-upper arm circumference (MUAC)-for-age show that in a well nourished population there are very few children aged 6–60 months with a MUAC less than 115 mm. Children with a MUAC less than 115 mm have a highly elevated risk of death compared to those who are above. Thus it is recommended to increase the cut-off point from 110 to 115 mm to define SAM with MUAC." WHO and UNICEF, WHO child growth standards and the identification of severe acute malnutrition in infants and children, 2009, Pg. 2.
- 6Our understanding is that reliable data about children who do not receive treatment is scarce.
- "The assessment of the risk of death associated with different degrees of wasting can be carried out only by community based longitudinal studies with a follow up of untreated malnourished children. This can be analysed only from a limited number of existing studies. For ethical reasons, these observational studies cannot be repeated, as an effective community-based treatment of severe acute malnutrition is now possible." WHO and UNICEF, WHO child growth standards and the identification of severe acute malnutrition in infants and children, 2009, Pg. 4.
However, one study in Ethiopia tracked children identified as MAM whose home districts were ineligible for food supplementation programs and found that only slightly over half of the children recovered without experiencing an episode of SAM during the 28 week tracking period:
- “We prospectively surveyed 884 children aged 6–59 months living with MAM in a rural area of Ethiopia not eligible for a supplementary feeding programme. Weekly home visits were made for seven months (28 weeks), covering the end of peak malnutrition through to the post-harvest period (the most food secure window), collecting anthropometric, socio-demographic and food security data...only 54.2% of the children recovered with no episode of SAM by the end of the study.” James et al. 2016, Abstract
- 7
UNICEF, WHO, World Bank, "Joint child malnutrition estimates — levels and trends," 2020, “Number (MIllions) Affected Tables,” pg. 13.
- 8
“Children suffering from wasting have weakened immunity, are susceptible to long term developmental delays, and face an increased risk of death, particularly when wasting is severe.” UNICEF, WHO, World Bank, "Joint child malnutrition estimates — levels and trends," 2020, pg. 2.
- 9
"Ready-to-use Therapeutic Food (RUTF) has revolutionized the treatment of severe malnutrition – providing foods that are safe to use at home and ensure rapid weight gain in severely malnourished children. The advantage of RUTF is that it is a ready-to-use paste which does not need to be mixed with water, thereby avoiding the risk of bacterial proliferation in case of accidental contamination. The product, which is based on peanut butter mixed with dried skimmed milk and vitamins and minerals, can be consumed directly by the child and provides sufficient nutrient intake for complete recovery." WHO, "Malnutrition"
- 10
- "Children with uncomplicated severe acute malnutrition, not requiring to be admitted and who are managed as outpatients, should be given a course of oral antibiotic such as amoxicillin." WHO, "Guideline: updates on the management of severe acute malnutrition in infants and children," 2013, Pg. 29.
- Table 1, Pg. 37 of Chad's national protocol for management of acute malnutrition displays the differences between SAM and MAM treatment:
- The "Produits [Products]" row for the "Traitement MAS [SAM treatment]" column states, "Différent produits Aliment Thérapeutique Prêt à l’Emploi (ATPE) – F75 – F100," which translates in English to "Different Ready-to-Use Therapeutic Food (RUTF) products - F75 - F100." The "Antibiothérapie systématique [Systematic antibiotic therapy]" row for the SAM column states "Oui" or "Yes" in English.
- The "Produits [Products]" row for the "Traitement MAM [MAM treatment]" column states, "Différents produits : Farines fortifiées (ex.CSB), Aliment de Supplément Prêt àl’Emploi (ASPE)," which translates in English to "Different products: Fortified flour (e.g. CSB), Ready-to-use supplementary food (RUSF)." The "Antibiothérapie systématique [Systematic antibiotic therapy]" row for the MAM column states "Non," or "No" in English.
- Republic of Chad, Ministry of Public Health, Social Action, and National Solidarity, National protocol for management of acute malnutrition, 2014
-
Mali's national CMAM protocol indicates that RUTF and systematic antibiotic therapy should be used to treat SAM:
- "L’Aliment Thérapeutique Prêt à l’Emploi (ATPE) est un composant essentiel des URENAS, permettant le traitement à domicile." Pg. 200.
- English translation from original French: "Ready-to-Use Therapeutic Food (RUTF) is an essential component of URENAS, allowing treatment at home."
- "Les antibiotiques doivent être donnés aux patients souffrant de MAS systématiquement, même si le patient ne présente pas de signes cliniques d’infections généralisées." Pg. 72.
- English translation from original French: "Antibiotics should be routinely given to patients suffering from SAM, even if the patient does not show clinical signs of general infection."
- Republic of Mali, Ministry of Health, Protocol for integrated management of acute malnutrition, 2011
- "L’Aliment Thérapeutique Prêt à l’Emploi (ATPE) est un composant essentiel des URENAS, permettant le traitement à domicile." Pg. 200.
- 11
- Table 1, Pg. 37 of Chad's national protocol for management of acute malnutrition displays the differences between SAM and MAM treatment:
- The "Produits [Products]" row for the "Traitement MAS [SAM treatment]" column states, "Différent produits Aliment Thérapeutique Prêt à l’Emploi (ATPE) – F75 – F100," which translates in English to "Different Ready-to-Use Therapeutic Food (RUTF) products - F75 - F100." The "Antibiothérapie systématique [Systematic antibiotic therapy]" row for the SAM column states "Oui" or "Yes" in English.
- The "Produits [Products]" row for the "Traitement MAM [MAM treatment]" column states, "Différents produits : Farines fortifiées (ex.CSB), Aliment de Supplément Prêt àl’Emploi (ASPE)," which translates in English to "Different products: Fortified flour (e.g. CSB), Ready-to-use supplementary food (RUSF)." The "Antibiothérapie systématique [Systematic antibiotic therapy]" row for the MAM column states "Non," or "No" in English.
- Republic of Chad, Ministry of Public Health, Social Action, and National Solidarity, National protocol for management of acute malnutrition, 2014
- Section IV, Pg. 118 of Mali's national CMAM protocol, which discusses management of MAM, states that the types of treatment provided for MAM include enriched flour and RUSF:
- "Les aliments de supplémentation utilisés par les URENAM sont à base de:
- Farines industrielles améliorées en complexes minéralo-vitaminiques répondant aux normes internationales (Supercerealplus, Supercereal2),
- Farines locales enrichies (Exemple: Misola)53.
- Aliments Supplémentaires prêts à l’emploi(ASPE): Pâte à base de lipides (Exemple, «Supplementary Plumpy»ou PlumpySup)."
- English translation from original French: "The supplementation foods used by URENAM are based on:
- Industrial flour improved in mineral-vitamin complexes meeting international standards (Supercerealplus, Supercereal2),
- Enriched local flours (Example: Misola) 53.
- Ready-to-use supplementary food (RUSF): Lipid-based paste (Example, "Supplementary Plumpy" or PlumpySup)."
- Republic of Mali, Ministry of Health, Protocol for integrated management of acute malnutrition, 2011
- "Les aliments de supplémentation utilisés par les URENAM sont à base de:
- Table 1, Pg. 37 of Chad's national protocol for management of acute malnutrition displays the differences between SAM and MAM treatment:
- 12
- “SAM and MAM are managed in separate programs, using different food products and protocols. There is currently no globally accepted guidance for the treatment of MAM, and MAM is not always routinely treated. International mandate adds an additional layer of complexity: UNICEF supports the treatment of SAM and provides ready-to-use therapeutic food (RUTF) for use in outpatient therapeutic programs (OTPs); the World Food Programme supports the treatment of MAM and provides ready-to-use supplementary food (RUSF) or fortified blended flours for use in supplementary feeding programs (SFPs). In humanitarian settings, providing treatment for both SAM and MAM adds to the logistical and financial burden of health systems. When resources are scarce, and in the many settings where prevalence is not high enough to reach emergency thresholds, treatment of SAM is often prioritized, and children with MAM may not be eligible to receive care unless they deteriorate.” Bailey et al. 2020, pg. 4.
- Victoire Hubert, Research Manager, ALIMA, comments on a draft of ALIMA’s 2021 grant page, May 8, 2021 (unpublished). See the grant page here.
- "In addition to the tangle of agencies and case definitions, SAM and MAM programmes are chronically underfunded with only 25% of SAM cases treated globally in 2016 and 16% of (9,10) MAM cases reached by the World Food Program in 2017." Daures et al. 2020, Pg. 757.
- 13
Reliable data about children who do not receive treatment appears scarce. However, one study in Ethiopia tracked children identified as having MAM whose home districts were ineligible for food supplementation programs and found that during the 28-week tracking period, “only 54.2% of the children recovered with no episode of SAM by the end of the study.” James et al. 2016, pg. 2.
- 14
“SAM and MAM are managed in separate programs, using different food products and protocols. There is currently no globally accepted guidance for the treatment of MAM, and MAM is not always routinely treated. International mandate adds an additional layer of complexity: UNICEF supports the treatment of SAM and provides ready-to-use therapeutic food (RUTF) for use in outpatient therapeutic programs (OTPs); the World Food Programme supports the treatment of MAM and provides ready-to-use supplementary food (RUSF) or fortified blended flours for use in supplementary feeding programs (SFPs). In humanitarian settings, providing treatment for both SAM and MAM adds to the logistical and financial burden of health systems. When resources are scarce, and in the many settings where prevalence is not high enough to reach emergency thresholds, treatment of SAM is often prioritized, and children with MAM may not be eligible to receive care unless they deteriorate.” Bailey et al. 2020, pg. 4.
- 15
We are aware of two variants of the combined protocol: one known as ComPAS and one known as OptiMA):- "The Combined Protocol for Acute Malnutrition Study (ComPAS) assessed the effectiveness of a simplified, unified SAM/MAM protocol for children aged 6–59 months...Combined protocol clinics treated children using 2 sachets of ready-to-use therapeutic food (RUTF) per day for those with mid-upper arm circumference (MUAC) 11.5 cm and/or edema, and 1 sachet of RUTF per day for those with MUAC 11.5 to 12.5 cm." Bailey et al. 2020, Abstract.
- "Although acute malnutrition is a continuum condition, it is arbitrarily divided into moderate (MAM) and severe (SAM) categories defined by mid upper arm circumference (MUAC) or weight-for-height Z-score (WHZ)...We piloted a new MUAC-based and oedema approach for treating acute malnutrition in Burkina Faso with a single-arm proof-of-concept trial called Optimising treatment for acute MAlnutrition (OptiMA)...only one product was used for treatment (RUTF) at a gradually reduced dose based on a child’s weight and MUAC status." Daures et al. 2020, Pgs. 756-757.
- 16
- "As part of the solution, practitioners and experts have recognised the need to simplify approaches to wasting treatment and have identified key research priorities, such as “reviewing appropriate entry and discharge criteria for treatment of acute malnutrition” and “investigating the safety, effectiveness and cost-effectiveness of reduced dosage ready to-use therapeutic food dosages” (No Wasted Lives, 2018). The aim is to achieve greater coverage and improved efficiency of services (including cost-effectiveness) for children at high risk of illness and death, while maintaining quality of care." Emergency Nutrition Network, "Simplified approaches to the treatment of wasting," July 2020, Pg. 1.
- "ALIMA’s Optimizing treatment for acute MAlnutrition (OptiMA) is one such strategy, proposing three main changes to current protocols:
- Earlier detection by training mothers and caregivers how to use mid-upper arm circumference (MUAC) bands to screen children regularly for malnutrition in the home (i.e., family MUAC.)
- Simplification and easier management by using only one anthropometric measure (MUAC 125 mm (and/or oedema)) for admissions and one product (RUTF) for treatment.
- More intelligent use of the costliest input (RUTF) by gradually reducing the dosage based on a child’s MUAC status and weight to increase the number of children with access to treatment at no extra or similar cost." Phelan 2019, Pg. 40.
- 17
- "ALIMA’s Optimizing treatment for acute MAlnutrition (OptiMA) is one such strategy, proposing three main changes to current protocols:
- Earlier detection by training mothers and caregivers how to use mid-upper arm circumference (MUAC) bands to screen children regularly for malnutrition in the home (i.e., family MUAC.)
- Simplification and easier management by using only one anthropometric measure (MUAC 125 mm (and/or oedema)) for admissions and one product (RUTF) for treatment.
- More intelligent use of the costliest input (RUTF) by gradually reducing the dosage based on a child’s MUAC status and weight to increase the number of children with access to treatment at no extra or similar cost." Phelan 2019, Pg. 40.
- WHO defines 115 mm MUAC as the cutoff point between SAM and MAM.
- "In children aged 6–59 months, moderate acute malnutrition is defined as moderate wasting (i.e. weight-for-height between –3 and –2 Z-scores of the WHO Child Growth Standards median) and/or mid-upper-arm circumference (MUAC) greater or equal to 115 mm and less than 125 mm." WHO, "Supplementary foods for the management of moderate acute malnutrition in children aged 6–59 months," 2019.
- “Severe acute malnutrition is when children suffer severe wasting that may or may not be accompanied by swelling of the body from fluid retention. It occurs when infants and children do not have adequate energy, protein and micronutrients in their diet, combined with other health problems such as recurrent infections. It is diagnosed when the circumference of the upper arm is less than 115 mm or when the weight for height of a child is severely reduced.” WHO, "WHO issues new guidance for treating children with severe acute malnutrition," 2013
- "ALIMA’s Optimizing treatment for acute MAlnutrition (OptiMA) is one such strategy, proposing three main changes to current protocols:
- 18
- Victoire Hubert, Research Manager, ALIMA, comments to GiveWell on a draft of ALIMA’s January 2021 grant page, May 8, 2021 (unpublished)
- See the January 2021 grant page here.
- 19
"The community-based approach involves timely detection of severe acute malnutrition in the community and provision of treatment for those without medical complications with ready-to-use therapeutic foods or other nutrient-dense foods at home [...] Community health workers or volunteers can easily identify the children affected by severe acute malnutrition using simple coloured plastic strips that are designed to measure mid-upper arm circumference (MUAC) [...] Once children are identified as suffering from severe acute malnutrition, they need to be seen by a health worker who has the skills to fully assess them following the Integrated Management of Childhood Illness (IMCI) approach. The health worker should then determine whether they can be treated in the community with regular visits to the health centre, or whether referral to in-patient care is required." WHO, "Community-based management of severe acute malnutrition," 2007, Pgs. 2-3.
- 20
“The updated WHO guidelines recommend that children with severe acute malnutrition who do not have health complications that require hospitalization, receive special, high-energy food and antibiotics to treat infection. This allows them to recover at home with their families.” WHO, "WHO issues new guidance for treating children with severe acute malnutrition," 2013.
- 21
"Severe acute malnutrition remains a major killer of children under five years of age. Until recently, treatment has been restricted to facility-based approaches, greatly limiting its coverage and impact." WHO, "Community-based management of severe acute malnutrition," 2007, pg. 2.
- 22
Covert infection:
- “The lack of clinical signs and symptoms and atypical clinical presentation in some infected malnourished children were attributed to impairment of the acute inflammatory response.” Christie, Heikens, and McFarlane 1988, Abstract.
- “Many advanced cases of SAM are complicated by concurrent infective illness, particularly acute respiratory infection, diarrhoea, and gram-negative septicaemia.” Collins et al. 2006, pg. 1992.
“The currently available evidence supports the continued routine administration of amoxicillin 80mg/kg/day in two divided doses for 7 days for children with uncomplicated SAM treated within the community.” Williams and Berkley 2016, pg. 9.
- 23
The Combined Protocol for Acute Malnutrition Study (ComPAS) (Bailey et al. 2020) tested a protocol using MUAC (along with presence of edema) as the single criterion to diagnose acute malnutrition, determine dosage of RUTF, and diagnose recovery in South Sudan and Kenya. The Optimizing treatment for acute MAlnutrition (OptiMA) protocol has been trialled in Burkina Faso (Phelan 2019) and DRC (Phelan 2019), with another trial planned for Niger (U.S. National Library of Medicine, ClinicalTrials.gov, "Optimizing Acute Malnutrition Management in Children Aged 6 to 59 Months in Niger (OptIMA Niger)," 2021). The OptiMA protocol uses MUAC (and presence of edema) to diagnose and discharge patients and uses both weight and MUAC to determine dosage of RUTF.
- 24
"Community health workers or volunteers can easily identify the children affected by severe acute malnutrition using simple coloured plastic strips that are designed to measure mid-upper arm circumference (MUAC). In children aged 6-59 months, a MUAC less than 110 mm indicates severe acute malnutrition, which requires urgent treatment. Community health workers can also be trained to recognize nutritional oedema of the feet, another sign of this condition." WHO, "Community-based management of severe acute malnutrition," 2007, pg. 2-3. Alé et al. 2016 provides evidence that mothers and other caregivers can be trained to accurately measure MUAC and identify malnourished children.
- 25
- “Children who are identified as having severe acute malnutrition should first be assessed with a full clinical examination to confirm whether they have medical complications and whether they have an appetite. Children who have appetite (pass the appetite test) and are clinically well and alert should be treated as outpatients. Children who have medical complications, severe oedema (+++), or poor appetite (fail the appetite test), or present with one or more Integrated Management of Childhood Illness (IMCI) danger signs should be treated as inpatients (strong recommendation, low quality evidence).” WHO, "WHO child growth standards and the identification of severe acute malnutrition in infants and children," 2009, pg. 3.
- Our understanding is that the assessment procedures described above for standard CMAM are followed in the combined protocols as well.
- 26
“[In CMAM], the outpatient clinic monitors the child’s response to the treatment and provides antimicrobial, antihelminthic, and antimalarial drugs; vitamin A supplementation; and measles vaccination (if required) before sending them home with sufficient ready to use therapeutic food (RUTF) to last until the following visit, allowing recovery to take place in the community.” Rogers et al. 2015, pg. 2.
- 27
- It is hypothesized that reducing infection in children with SAM can speed nutritional recovery and prevent mortality via prevention of colonizing microorganisms, reduction of the inflammatory response, direct reduction of inflammation, reduction in intestinal disease, and alteration of the gut microbiome. This mechanistic understanding is partially based on findings from broad-spectrum antibiotic use in children with HIV.
- “The increased childhood mortality associated with undernutrition is almost entirely due to the elevated risk of death from common infectious diseases such as pneumonia, diarrhea, and bacterial sepsis. . . . A vicious cycle between malnutrition and infection has been long recognized. Episodes of infection potentiate undernutrition via anorexia, reduced nutrient absorption, nutrient losses (such as vitamin A and proteins in diarrhea), diversion of nutrients to inflammatory responses, and tissue repair. Diarrhea is associated with malabsorption and marked losses of protein, vitamin A, zinc, and other micronutrients. All infections are associated with net protein loss with diversion of amino acids to acute phase and immune response proteins. Activation of inflammatory cascades also causes reduced appetite and loss of lean tissue and fat. Thus, episodes of infection, especially diarrhea, result in both linear and ponderal growth-faltering.” Jones et al. 2014, pg. S65.
- “The mechanisms by which these trials not only reduced mortality, but improved growth, are not clear. They may include treatment of active (but covert) infection; prevention of colonizing microorganisms causing disease; reduction of inflammatory responses, resulting in less nutrient diversion and less cytokine-mediated impairment of growth through hormonal control; nonantibiotic effects, including direct anti-inflammatory effects; reduction in enteropathy; and alterations in gut microbiome.” Jones et al. 2014 (on trials of antibiotics in children with HIV), pg. S67. Also see Figure 3 on pg. S68.
- 28
- ComPAS: “The rationale for a reduced dosage is to facilitate increased coverage—and in turn increased public health impact—of treatment in a resource-constrained environment. The optimal dosage achieves the right balance between meeting individual energy needs and extending treatment to more children. This study contributes to the evidence on the impact of different dosage regimes. This study aimed to test the hypothesis that the combined protocol would be non-inferior to the standard protocol in terms of recovery, and improve cost-effectiveness. Bailey et al. 2020, pg. 4-5.
- OptiMA: “More intelligent use of the costliest input (RUTF) by gradually reducing the dosage based on a child’s MUAC status and weight to increase the number of children with access to treatment at no extra or similar cost.” Phelan 2019.
- 29
We believe this is because the availability of community-based treatment makes it unethical to track malnourished children without treating them. For example, a WHO report says, “The assessment of the risk of death associated with different degrees of wasting can be carried out only by community based longitudinal studies with a follow up of untreated malnourished children. This can be analysed only from a limited number of existing studies. For ethical reasons, these observational studies cannot be repeated, as an effective community-based treatment of severe acute malnutrition is now possible.” WHO, "WHO child growth standards and the identification of severe acute malnutrition in infants and children," 2009, pg. 4, footnote 1.
- 30
- “In response to infection, the immune system first executes innate and then subsequently acquired host defense functions of high diversity. Both processes involve activation and propagation of immune cells and synthesis of an array of molecules requiring DNA replication, RNA expression, and protein synthesis and secretion, and therefore consume additional anabolic energy. Mediators of inflammation further increase the catabolic response. . . . Consequently, the nutritive status of the host critically determines the outcome of infection. Apart from deficiencies in single nutrients, such as vitamins, fatty acids, amino acids, iron, and trace elements, undernourishment based on [protein energy malnutrition] PEM greatly increases susceptibility to major human infectious diseases in low-income countries, particularly in children.” Schaible and Kaufmann 2007, pg. 0806.
- “Undernourished children principally die of common infections, implying that mortality is related to underlying immunodeficiency, even in mild forms of undernutrition...The precise nature of immunodeficiency in undernutrition therefore remains uncertain; however, the consensus from the available evidence is that both innate and adaptive immunity are impaired by malnutrition. Defects in innate immune function include impaired epithelial barrier function of the skin and gut, reduced granulocyte microbicidal activity, fewer circulating dendritic cells, and reduced complement proteins, but preserved leukocyte numbers and acute phase response. Defects in adaptive immune function include reduced levels of soluble IgA in saliva and tears, lymphoid organ atrophy, reduced delayed-type hypersensitivity responses, fewer circulating B cells, a shift from Th1-associated to Th2-associated cytokines, and lymphocyte hyporesponsiveness to phytohemagglutinin, but preserved lymphocyte and immunoglobulin levels in peripheral blood. Despite this, most malnourished children seem to respond adequately to vaccination, although the timing, quality, and longevity of vaccine-specific responses may be impaired.” Bourke, Berkley, and Prendergast 2016, pg. 386-87.
- 31
- “Ready-to-use therapeutic foods (RUTF) are high energy, fortified, ready-to-eat foods suitable for the treatment of children with severe acute malnutrition. These foods should be soft or crushable and should be easy for young children to eat without any preparation. At least half of the proteins contained in the foods should come from milk products." WHO, "Community-based management of severe acute malnutrition," 2007, pg. 6.
- WHO outlines the specific nutritional composition of RUTF in the Nutritional Composition table of WHO, "Community-based management of severe acute malnutrition," 2007, pg. 6. “Few studies have directly targeted immune pathways in malnourished children; however, standard protocols for SAM treatment include antibiotics, which can reduce mortality and improve nutritional recovery. The mechanisms through which antibiotics improve outcomes in malnutrition are unclear, but may include treating clinical and subclinical infections, reducing chronic inflammation or ameliorating enteropathy through changes in the microbiota; antibiotic effects on immune function have not been evaluated.” Bourke, Berkley, and Prendergast 2016, pg. 396.
- 32
- See Olofin et al. 2013, Table 1, pg. 4.
- Our impression is that Olofin et al. 2013 and an earlier analysis (Black et al. 2008) are the most important papers estimating malnutrition’s effects on mortality. Black et al. 2008 has more than 6,000 citations, and WHO, "Updates on the management of severe acute malnutrition in infants and children," 2013 cites Black et al. 2013, which updates and expands on Black et al. 2008. Black et al. 2013, in turn, cites Olofin et al. 2013 (then in press) on mortality effects.
- From WHO, "Updates on the management of severe acute malnutrition in infants and children," 2013, pg. 10: “Childhood undernutrition is a major global health problem, contributing to childhood morbidity, mortality, impaired intellectual development, suboptimal adult work capacity, and increased risk of diseases in adulthood (7).” (Reference 7 is to Black et al. 2013.)
- From Black et al. 2013, pg. 438: “Suboptimum growth, according to anthropometric measures indicative of stunting, wasting, and underweight, has been shown to increase the risk of death from infectious diseases in childhood. This association has been recently re-examined with the pooled analysis of individual-level data from ten longitudinal studies involving more than 55 000 child-years of follow-up and 1315 deaths in children younger than 5 years. As with previous analyses, all degrees of stunting, wasting, and underweight had higher mortality and the risk increased as Z scores decreased (appendix p 11).” (Appendix, pg. 11 cites Olofin et al. 2013.)
- While Black et al. 2008 and Olofin et al. 2013 come to similar conclusions, we use Olofin et al. 2013 because it includes more studies than Black et al. 2008 (10 studies total, including seven of the eight in Black et al. 2008; information about the constituent studies is summarized here) and includes a more detailed methodological description).
- 33
See the "Access to health care" column here.
- 34
Hazard ratio for SAM (weight for length/height z score < -3) is 11.63 (CI: 9.84, 13.76). Hazard ratio for MAM (weight for length/height z score between -3 and -2 is 3.38 (CI: 2.86, 3.98). Olofin et al. 2013, Table 3, pg. 5.
- 35
- “We further adjusted for child’s sex and the assigned treatment in the randomized trials in our minimally adjusted models. Some additional covariates were available in 6 cohorts (e.g., household assets, mother’s education, household water source, and sanitation. See Table S1) but the available covariates differed across cohorts. Therefore, the maximally-adjusted HRs were estimated separately for each of the 6 cohorts and the HRs were pooled using a random effects meta-analysis using the method of DerSimonian and Laird.” Olofin et al. 2013, pg. 3.
- Minimally vs maximally adjusted HRs were 14.32 vs. 14.20 for SAM and 3.70 vs. 3.47 for MAM. See Olofin et al. 2013, Table 4, pg. 7.
- 36
- “The estimated odds ratios were then adjusted for confounding due to socioeconomic factors that affect mortality through other pathways, such as non-nutritional determinants of infection or access to better clinical care. The adjustment used data sets with robust measurement of socioeconomic status from Nepal and Honduras and showed that odds ratios were attenuated by 10% and 20%, respectively. On the basis of these results, 15% attenuation was applied to the odds ratios calculated with the generalised linear mixed models for underweight, stunting, and wasting.” Black et al. 2008, pg. 247.
- Black et al. 2008 do not report the covariates that are included to generate these estimates. However, the Nepal study is also used in the analysis by Olofin et al. 2013, and in Olofin et al. 2013, Table S1, they report available covariates as "Household assets (household ownership of: bari, khet; number of household owned: bicycles, cattle, goats, radios; materials used for house walls and roof), mother’s education, mother’s age, household latrine ownership, household caste."
- 37
Black et al. 2008 do not report the covariates that were measured in the two studies they use to estimate confounding. However, one of those studies (conducted in Nepal) is also used in the analysis by Olofin et al. 2013, and in Olofin et al. 2013, Table S1 they report available covariates as "Household assets (household ownership of: bari, khet; number of household owned: bicycles, cattle, goats, radios; materials used for house walls and roof), mother’s education, mother’s age, household latrine ownership, household caste." We do not know which covariates were reported in the other study, which was conducted in Honduras.
- 38
Children who are referred for inpatient treatment during CMAM treatment are generally not counted in CMAM program outcomes. “Individuals referred for complementary services, such as healthcare, have not ended the treat- ment and will either continue treatment or return to the treatment later. Do not include individuals transferred to other sites or who have not ended the treatment.” Sphere Association, The Sphere Handbook: Humanitarian Charter and Minimum Standards in Humanitarian Response, fourth edition, 2018, pg. 176.
- 39
In a very small analysis of 35 defaulters in Nigeria, the most common reasons given for defaulting were death, "didn’t eat Plumpy / vomited / couldn’t swallow," and "enrolled when visiting relatives / migrated." Lee et al. 2013, Slide 8.
- 40
“Experience over the past 5 years indicates that when sufficient attention is given to early case finding, most cases of SAM can be successfully treated solely as outpatients, enabling resource intensive inpatient care to be reserved for the minority suffering from SAM with complications.” Collins 2007.
- 41
- Specifically, we assume that 10% of all children with SAM at baseline in Olofin et al. 2013 had complicated cases, based on our understanding of rates of complicated SAM found in contemporary nutrition programs (GiveWell's non-verbatim summary of a conversation with ALIMA, November 13, 2020).
- We assume their mortality rate was similar to historical case fatality rates recorded for hospitalized children with complicated SAM (i.e., approximately 25%): "In most developing countries, case fatality rates (CFRs) in hospitals treating SAM remain at 20–30% and few of those requiring care actually access treatment." Collins 2007, Abstract.
- For simplicity, we attribute recorded deaths to the baseline status (i.e., we assume that children didn’t move between MAM, SAM, and non-malnourished states). Calculations are here.
- 42
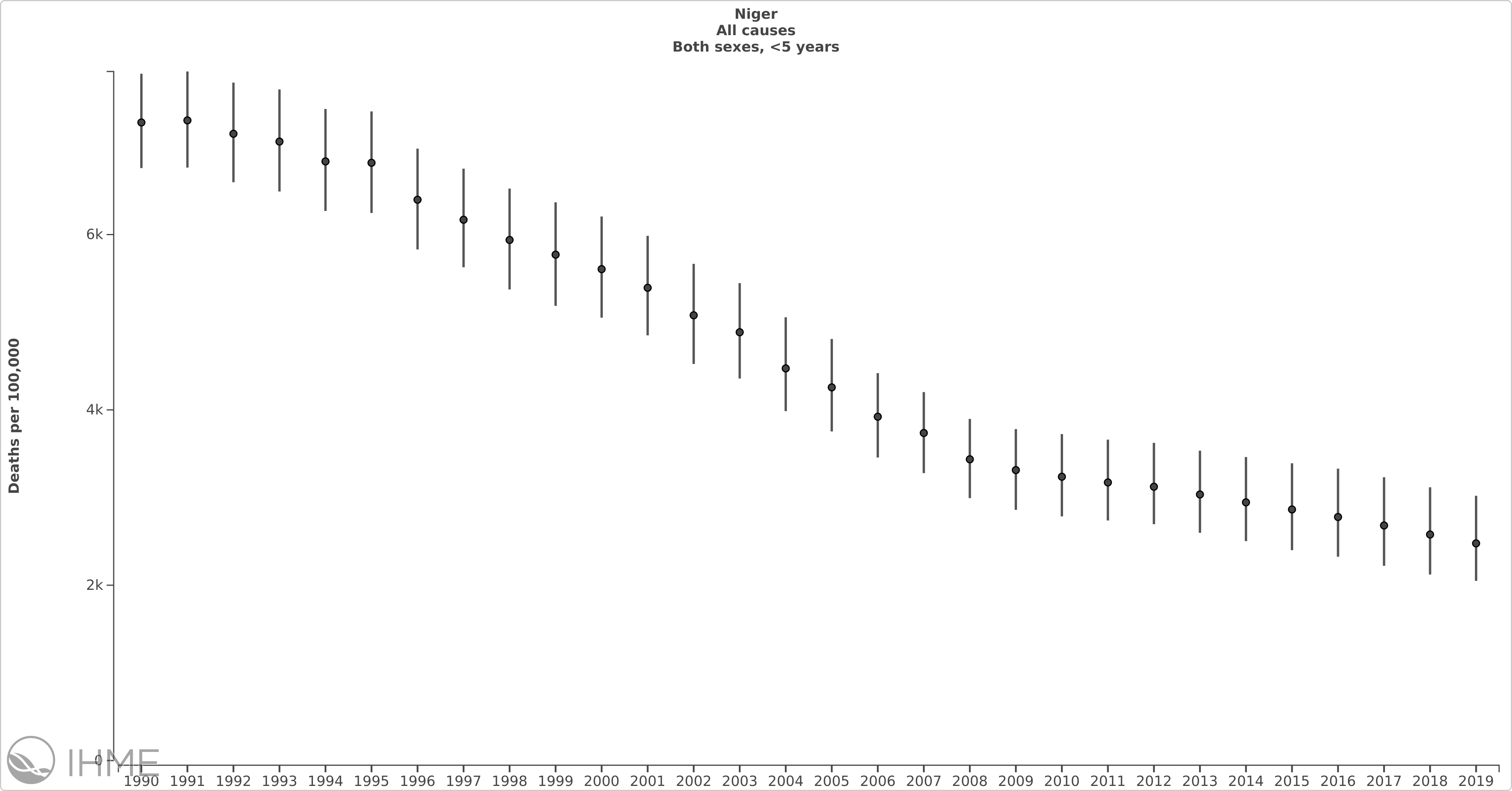
For example, in Niger under-5 child mortality rates are estimated to have fallen from approximately 7.3% in 1990 to approximately 2.4% in 2019. IHME, GBD Compare tool, under 5 deaths in Niger.
- 43
- All-cause HR for SAM (i.e., weight-for-length z-score < -3)=11.6 (95% CI: 9.84, 13.76). Olofin et al. 2013, Table 3, pg. 5. Cause-specific HR for respiratory tract infections=9.68 (6.07, 15.43); Diarrheal disease = 12.33 (9.18,16.57); Other infectious causes = 11.21 (5.91, 21.27); Malaria=1.24 (0.17, 9.29); and Measles = 9.63 (5.15, 18.01). Olofin et al. 2013, Table 5, pg. 8.
- Diarrheal incidence is estimated to have decreased about 12%, whereas all other categories have decreased at least 37%. See here.
- 44
HR for SAM (i.e., weight-for-length z-score < -3)=11.6 (95% CI: 9.84, 13.76). Olofin et al. 2013, Table 3, pg. 5. HR for respiratory tract infections=9.68 (6.07, 15.43); Diarrheal disease = 12.33 (9.18,16.57); Other infectious causes = 11.21 (5.91, 21.27); Malaria=1.24 (0.17, 9.29); and Measles = 9.63 (5.15, 18.01). Olofin et al. 2013, Table 5, pg. 8.
- 45
Diarrheal incidence is estimated to have decreased about 12% whereas all other categories have decreased at least 37%. See here.
- 46
This excerpt comes from discussions on vitamin A supplementation trials, but the same principles apply: “Cause-specific mortality results in the Ghana VAST trial, and other VAS trials, should be interpreted with caution because there is substantial uncertainty about how each individual died. Reasons for this include:
Diagnostic methods in these trials had substantial limitations. Most of the data come from “verbal autopsy”, an interview-based method that relies on the observations of family members and may be conducted months after a child’s death. These observations are then interpreted by physicians to form a diagnosis, and the assessments of individual physicians can differ substantially. Sometimes, no cause of death can be determined. This method is less accurate than a diagnosis based on direct examination by a physician and/or laboratory identification of pathogens.
It can be difficult to identify the primary cause of disease. Infectious disease deaths often involve multiple infectious organisms, and it can be difficult to determine which one is the primary cause of death. For example, in measles infection, secondary infections with other pathogens are often the proximate cause of death, and these secondary infections may be incorrectly identified as the primary cause of death.
Disease symptoms can overlap. For example, malaria can present with chest signs or diarrhea, and may therefore be coded as pneumonia or diarrhea. Conversely, deaths from pneumonia or diarrhea may be coded as being due to malaria.” GiveWell's non-verbatim summary of a conversation with Dr. David Ross, January 7, 2020. - 47
For example, the most recent Demographic and Health Survey Data from Niger showed that around 69% of 12-23-month-olds nationally had received the measles vaccine, only about 61% of children in the lowest economic quintile had, compared to 75% of children in the highest economic quintile. We expect that overall measles vaccination rates have increased in the intervening years but that the distributional patterns are likely to be similar. Institut National de la Statistique and ICF International, "Enquête démographique et de santé et à indicateurs multiples 2012," 2013, pg. 125-26.
- 48
“A vicious cycle between malnutrition and infection has been long recognized. Episodes of infection potentiate undernutrition via anorexia, reduced nutrient absorption, nutrient losses (such as vitamin A and proteins in diarrhea), diversion of nutrients to inflammatory responses, and tissue repair. Diarrhea is associated with malabsorption and marked losses of protein, vitamin A, zinc, and other micronutrients. All infections are associated with net protein loss with diversion of amino acids to acute phase and immune response proteins. Activation of inflammatory cascades also causes reduced appetite and loss of lean tissue and fat. Thus, episodes of infection, especially diarrhea, result in both linear and ponderal growth-faltering.” Jones et al. 2014, pg. S65.
- 49
For example, with regard to diarrhea cases: “The relative intractability of diarrhea incidence, as compared with diarrhea-related mortality, as shown in the present analysis and elsewhere, may suggest that growing access to timely and appropriate treatment, better nutritional status, and fewer coexisting conditions are contributing factors to reducing diarrhea-related mortality.” Reiner et al. 2018, pg. 1136.
- 50
Age distributions. We considered adjusting HR estimates upward to account for differing ages represented in the historical studies compared with CMAM programs, but did not ultimately make an adjustment.
- More than 34% of the children in studies used in Olofin et al. 2013 were 5 months of age or younger (Olofin et al. 2013, Table 2, pg. 5). Infants this young would not be treated in CMAM programs, which serve children 6-59 months.
- We understand that younger malnourished children generally have higher mortality rates than older children. However, HRs for malnutrition compared with a well-nourished state are lower for younger children than older children, because of higher mortality rates in general among infants and young toddlers. For example, using data on children 6-59 months in DRC, Senegal and Nepal (two of these three studies were also included in Olofin et al. 2013), Schwinger et al. 2019 find significantly greater HRs associated with severe acute malnutrition among children over 24 months than those under 24 months: “The hazard ratios (HR) were greater for children ≥ 24 months compared to younger children for all exposure categories (the WHZ-only category for SAM was not significant). As expected the mortality rate of normal older children was about half that of the younger children; there was a slightly lower fall in mortality rate between the age groups in the mildly malnourished groups. However, the reduction in mortality with age did not occur with moderately malnourished children, and the mortality rate was substantially higher in the severely malnourished older children than younger children assessed with either WHZ or MUAC, and particularly in those with both deficits.” Given this, the large proportion of children under 6 months of age in the studies included in Olofin et al. 2013 might lead to an underestimate of the average HR in a typical CMAM program.
- We choose not to adjust for this potential issue for two reasons. First, our understanding is that most children served by CMAM programs are at the younger end of the 6-59 month age spectrum. We expect the inclusion of younger children in the historical estimates would not significantly bias estimates if they are relatively close in age to the bulk of program participants. Second, we have not found a study that reports HRs for children under 6 months, which we feel is necessary to estimate an adjustment. We may revisit this issue later if the age distribution of a particular CMAM program we are considering funding implies that an age-adjustment could be consequential.
- 51
Country (Mortality rate): Congo, Democratic Republic of the (21%), Bangladesh (20%), Senegal (20%), Uganda (12%), Yemen (10%). See WHO, "Community-based management of severe acute malnutrition," 2007, pg. 2, "Mortality of children with severe acute malnutrition observed in longitudinal studies" table. Median = 20%, Average = 16.6%.
- 52
We have seen this approach used to estimate deaths averted by CMAM programs in Nigeria (Bulti et al. 2015) and Yemen (Al-Dheeb, Ziolkovska, and Chitekwe 2018). These write-ups were geared toward practitioners rather than academics and did not make any adjustments to hazard ratios derived from historical studies.
- 53
“Discharge criteria and monitoring: The number of discharged individuals includes those who have recovered, died, defaulted or not recovered. Individuals referred for complementary services, such as healthcare, have not ended the treatment and will either continue treatment or return to the treatment later. Do not include individuals transferred to other sites or who have not ended the treatment. If individuals join a nutrition programme after discharge from therapeutic care, report them as a separate category to avoid biased results. If an individual develops acute malnutrition symptoms as a result of other factors such as disability, cleft or surgical problems, include them in programme reporting. Investigate how the gender of the individual may influence access to treatment, treatment default, and recovery. Calculate discharge statistics as follows: Percentage of discharges recovered = number of individuals recovered/total number of discharged x 100.” Sphere Association, The Sphere Handbook: Humanitarian Charter and Minimum Standards in Humanitarian Response, fourth edition, 2018, pg. 176.
- 54
For example, Akparibo, Lee, and Booth 2017, appendix 3, summarizes published results of 5 CMAM studies. While the death rate was no higher than 4% in any of these studies, default ranged from 3.6% to 44%.
- 55
- Recent and planned trials of the combined protocols are designed to show non-inferiority of recovery between the combined protocols and standard protocol. Bailey et al. 2020 compared recovery rates under a simplified combined protocol using MUAC as the primary diagnostic tool (ComPAS) with the standard protocols in South Sudan and Kenya. It found “[r]ecovery in the combined protocol arm was non-inferior to that in the standard protocol arm, with 76.3% recovering in the combined protocol arm and 73.5% recovering in the standard protocol arm (risk difference of 0.03, 95% CI −0.05 to 0.10, p = 0.52).” Pg. 3. Mortality rates and non-response rates also did not differ significantly across trial arms. (Adjusted risk difference in death between standard and combined protocols with 95% CI: 0.00 [-0.01, 0.01]. Adjusted risk difference in non-response between standard and combined protocols with 95% CI: -0.03 [-0.10, 0.05]. Bailey et al. 2020, Table 2, pg. 13.)
- We understand that a trial of the optiMA combined protocol with non-inferior recovery as a primary outcome concluded in Democratic Republic of the Congo in 2020: “The investigators propose to conduct a community-based non-inferiority clinical trial with individual randomization comparing the OptiMA strategy to the Democratic Republic of Congo standard nutritional protocol for SAM. Study children will be randomly assigned to the intervention arm or control arm - with children at MUAC < 125 mm or oedema eligible for RUTF in the intervention arm and those meeting current WHO SAM definition eligible in the control group. All participants will be followed for 9 months post-randomization to assess non-inferiority as defined by a composite of three endpoints : alive, acceptable nutritional status (MUAC ≥ 125 mm and WHZ > -3, no oedema) and no relapse to acute malnutrition for those who were treated with RUTF. The main secondary outcome will assess the non-inferiority of OptiMA RUTF dosing (170 kcal/kg/d) in children meeting current WHO SAM criteria compared to children with the same criteria in the control arm who will receive 130-200 kcal/kg/d. . . . Actual study completion data: July 20, 2020.” U.S. National Library of Medicine, ClinicalTrials.gov, "Optimizing Acute Malnutrition Management in Children Aged 6 to 59 Months in Democratic Republic of Congo (OptiMA-DRC)," 2018.
- Another planned trial in Niger will compare recovery rates for under optiMA and ComPAS to the standard CMAM protocols: “This community-based non-inferiority trial will compare two strategies for the treatment of AM to the Niger protocol for SAM and MAM. The Optimizing treatment for acute MAlnutrition (OptiMA) strategy uses MUAC < 125 mm or nutritional oedema as admission criteria and optimizes RUTF by adapting doses to the degree of malnutrition. RUTF dose for MUAC < 115 mm or oedema is 170 kcal/kg/d and progressively reduces to 75 kcal/kg/d as MUAC increases. The Combined Protocol for Acute Malnutrition Study (ComPAS) uses the same eligibility criteria like OptiMA, but simplifies more the RUTF ration by providing 1000 kcal/d for children with oedema or MUAC < 115 mm and 500 kg/d for children with MUAC 115-124 mm. Children are considered recovered if they have 2 consecutive weekly MUAC measures ≥ 125 mm. Children will be individually randomized to treatment in one of the 3 study arms and will attend clinic visits weekly until nutritional recovery. After discharged, they will be monitored monthly via a nurse-conducted home visits until 6 months post-inclusion. The trial arms will be compared using a composite outcome indicator that includes vital status, anthropometric measures and relapse following the index AM episode. The hypothesis is that simplified strategies could substantially increase the number of children in care compared to current SAM programs without requiring additional RUTF or staffing while maintaining recovery rates in line with current programs.” U.S. National Library of Medicine, ClinicalTrials.gov, "Optimizing Acute Malnutrition Management in Children Aged 6 to 59 Months in Niger (OptIMA Niger)," 2021.
- 56
- "Twenty-one (21) community-based therapeutic care programs were implemented in Malawi, Ethiopia, and North and South Sudan between 2000 and 2005. These programs, which treated 23,511 cases of severe acute malnutrition, achieved recovery rates of 79.4% and mortality rates of 4.1%. Coverage rates were approximately 73%. Of the severely malnourished children who presented, 76% were treated solely as outpatients." Collins et al. 2006, pg. S49.
- A recent update to a Cochrane review now including six studies reports a much lower average recovery rate. The pooled rate is ~52.6% in RUTF arm ((298+208+31+57+15+6) / (605+290+174+68+20+13) = ~52.6). See Analysis 1.1 of Schoonees et al. 2019. This low rate is largely driven by two studies from India (Bhandari et al. 2016 and Jadhav et al. 2016) that have low recovery rates across intervention arms. We are unsure why these rates of recovery are lower.
- We chose to use the recovery rate from Collins et al. 2006 because it seems closer to rates reported by programs similar to those we might consider recommending funding. For example, the recovery rate for children with uncomplicated SAM was around 93% in 2020 in a CMAM program in Mirriah, Niger (program data provided by ALIMA), and a recent proof-of-concept trial of optiMA in Burkina Faso reported recovery rates of 86% overall and approximately 70% among children with MUAC < 115 (Daures et al. 2020). We anticipate using data from programs we're considering recommending funding in the future to update these parameters.
- 57
- Suri, Moorthy, and Rosenberg 2016, Table 4. We specifically use recovery rates among children with MAM treated with ready-to-use-food with a dairy component, because we understand there is some evidence that dairy proteins aid recovery from malnutrition, and such proteins are used in RUTF.
- “Studies suggest that dairy protein—as opposed to plant-based protein—increases lean body mass, accelerates linear growth, and improves recovery outcomes in undernourished populations. The biological explanation for these improved outcomes may be the existence of bioactive peptides, growth stimulating factors, a high concentration of branched-chain amino acids, and/or lactose. At its most basic level, milk protein consists of 2 major components: whey and casein. Whereas casein stimulates production of insulin-like growth factor I, whey has been linked to muscle restoration, bone growth, immune function, and intestinal integrity.” Stobaugh et al. 2016, pg. 926.
- 58
This possibility was raised in an analysis of deaths averted by CMAM programs in Nigeria: “This figure is, however, likely to underestimate the true proportion of beneficiaries that benefited substantially from the programme. This is because it is likely that a significant proportion of defaulting cases will have “defaulted” because the child had recovered and was clinically well. Such cases might be considered as self-discharged as cured.” Bulti et al. 2015, pg. 33.
- 59
- Stobaugh et al. 2018 is a systematic review of relapse rates following discharge from SAM treatment. We look at the subset of CMAM studies that reported cumulative incidence of relapse and extrapolate to estimate an annual rate. The resulting median annual relapse rate is 15% (see here). We use the simplifying assumptions that (i) the average child is 24 months old at discharge and thus has 35 months left of early childhood, and (ii) SAM and MAM incidents are uniformly distributed throughout childhood. We calculate (35/12) * 15 = 44%.
- The reduced dosage of RUTF used in combined protocol CMAM programs raises the concern that they could have higher relapse rates than standard programs. A four-month follow-up to the comPAS study in Kenya and South Sudan found no difference in rates of relapse for SAM or MAM children treated under the simplified or combined protocols: “There was no significant difference in odds of relapse between protocols (SAM, 3% vs 3%, OR = 1.0 p = 0.75; MAM, 10% vs 12%, OR = 0.90 p = 0.34).” Lelijveld et al. 2021, pg. 2.
- We are aware of, but have not yet reviewed results from, two additional trials (in Democratic Republic of the Congo and Niger) that track relapse under combined vs. standard protocols.
- “The investigators propose to conduct a community-based non-inferiority clinical trial with individual randomization comparing the OptiMA strategy to the Democratic Republic of Congo standard nutritional protocol for SAM. Study children will be randomly assigned to the intervention arm or control arm - with children at MUAC < 125 mm or oedema eligible for RUTF in the intervention arm and those meeting current WHO SAM definition eligible in the control group. All participants will be followed for 9 months post-randomization to assess non-inferiority as defined by a composite of three endpoints : alive, acceptable nutritional status (MUAC ≥ 125 mm and WHZ > -3, no oedema) and no relapse to acute malnutrition for those who were treated with RUTF. The main secondary outcome will assess the non-inferiority of OptiMA RUTF dosing (170 kcal/kg/d) in children meeting current WHO SAM criteria compared to children with the same criteria in the control arm who will receive 130-200 kcal/kg/d.” U.S. National Library of Medicine, ClinicalTrials.gov, "Optimizing Acute Malnutrition Management in Children Aged 6 to 59 Months in Democratic Republic of Congo (OptiMA-DRC)," 2018.
- “This community-based non-inferiority trial will compare two strategies for the treatment of AM to the Niger protocol for SAM and MAM. . . . After discharged, they will be monitored monthly via a nurse-conducted home visits until 6 months post-inclusion. The trial arms will be compared using a composite outcome indicator that includes vital status, anthropometric measures and relapse following the index AM episode. The hypothesis is that simplified strategies could substantially increase the number of children in care compared to current SAM programs without requiring additional RUTF or staffing while maintaining recovery rates in line with current programs.” U.S. National Library of Medicine, ClinicalTrials.gov, "Optimizing Acute Malnutrition Management in Children Aged 6 to 59 Months in Niger (OptIMA Niger)," 2021.
- 60
The costs of this subsequent round of treatment are included in our cost effectiveness analysis.
- 61
We identified one systematic review of papers that reported mortality rates among children 6-24 months after being discharged from treatment programs. It found that “of those discharged as nutritionally cured, mortality ranged from 0.06% to 10.4% at an average of 12 months post-discharge.” O'Sullivan et al. 2018, pg. 1. We are unsure whether children in this review received additional rounds of treatment (as we assume in our cost-effectiveness analysis), but given low coverage rates, it seems unlikely. Therefore, we would expect deaths following relapse under our assumptions to be lower than observed in this review.
- 62
Mortality resulting from uncomplicated SAM is strongly associated with the age of a child, with children under two representing the highest-risk age group.” GiveWell's non-verbatim summary of a conversation with Professor Jay Berkley, December 5, 2019.
- 63
“In studies that provided nutritional supplements, we observed positive significant pooled effect sizes on all five outcomes of length-for-age z-score or height-for-age z-score (effect size 0.05, 95% CI 0.01–0.09; p=0.01; n=50), cognitive or mental (0.06, 0.03-0.10; p<0.01; n=38), language (0.08, 0.03–0.13; p=0.01; n=21), motor (0.08, 0.04–0.12; p<0.01; n=41), and social-emotional (0.07, 0.02–0.12; p=0.01; n=20) scores.” Prado et al. 2019, pg. e1398.
- 64
“The use of amoxicillin to treat uncomplicated SAM has therapeutic benefits visible by anthropometry and by content of the gut microbiota. The main concern with the use of prophylactic antibiotics for this purpose is the effect on antibiotic resistance gene enrichment in the children’s microbiota. This concern was not supported here. The benefit/cost ratio for the use of prophylactic antibiotics for individuals in this cohort is positive when weighing effects on anthropometry, microbiome, and antibiotic resistance.” Langdon et al. 2018, Abstract.
- 65
“Overall resistance to commonly used drugs, like amoxicillin (MR 72.9%, IQR9.1%–87.3%) and trimethoprim/sulfamethoxazole (MR 75.0%, IQR 49.5%–92.3%) was high. . . . The high levels of resistance to amoxicillin and penicillin in S. pneumoniae and H. influenzae are also concerning given that pneumonia is a leading cause of death in children.” Tadesse et al. 2017, pg. 3-4, 7.
- 66
“The use of amoxicillin to treat uncomplicated SAM has therapeutic benefits visible by anthropometry and by content of the gut microbiota. The main concern with the use of prophylactic antibiotics for this purpose is the effect on antibiotic resistance gene enrichment in the children’s microbiota. This concern was not supported here. The benefit/cost ratio for the use of prophylactic antibiotics for individuals in this cohort is positive when weighing effects on anthropometry, microbiome, and antibiotic resistance.” Langdon et al. 2018, Abstract.
- 67
Das et al. 2020, Supplementary Information, Figure 15, pg. 9.
- 68
“No cases of severe allergy or anaphylaxis were identified. A total of three adverse events that were presumed to be drug reactions were reported: a generalized papular rash in a child who received amoxicillin, thrush in a child who received cefdinir, and bloody diarrhea that resolved spontaneously while treatment continued in a child who received cefdinir.” Trehan et al. 2013, pg. 428 and 430.
- 69
“The most common adverse reactions (> 1%) observed in clinical trials of AMOXIL capsules, tablets or oral suspension were diarrhea, rash, vomiting, and nausea.” FDA, "AMOXIL (amoxicillin) capsules, tablets or powder for oral suspension," 2015, pg. 1.
- 70
“Antibiotic exposure in children within the first 2 years of life was associated with current asthma (adjusted odds ratio [aOR] 1.72, 95% confidence interval [CI] 1.10–2.70), current atopic dermatitis (aOR 1.40, 95% CI 1.01–1.94), and current allergic rhinitis (aOR 1.65, 95% CI 1. 05–2.58) at 5 years of age. Analysis of the associations by type of antibiotics showed that cephem was associated with current asthma (aOR 1.97, 95% CI 1.23–3.16) and current rhinitis (aOR 1.82, 95% CI 1.12–2.93), and macrolide was associated with current atopic dermatitis (aOR 1.58, 95% CI 1.07–2.33).” Yamamoto-Hanada et al. 2017, Abstract.
- 71
“Antibiotic exposure in early life significantly increased risk of childhood overweight [relative risk (RR) = 1.23, 95% confidence interval (CI) 1.13–1.35, P < 0.001] and childhood obesity (RR = 1.21, 95% CI 1.13–1.30, P < 0.001). Antibiotic exposure in early life also significantly increased the z-score of childhood body mass index (mean difference: 0.07, 95% CI 0.05–0.09, P < 0.00001). Importantly, there was an obvious dose–response relationship between antibiotic exposure in early life and childhood adiposity, with a 7% increment in the risk of overweight (RR = 1.07, 95% CI 1.01–1.15, P = 0.03) and a 6% increment in the risk of obesity (RR = 1.06, 95% CI 1.02–1.09, P < 0.001) for each additional course of antibiotic exposure.” Shao et al. 2017, Abstract.
- 72
“The same countries that are receiving the most RUTF are those experiencing rapid changes in the nutrition landscape and increasing levels of obesity and chronic disease. The programs chosen to combat malnutrition must account for potential negative long-term effects across the lifespan that are relevant in the context of the nutrition transition and the double burden of over and undernutrition. Growth restriction in utero, rapid weight gain and undernutrition in childhood have shown some association with increased risk of obesity, diabetes, metabolic syndrome and associated chronic diseases in adulthood. Is it responsible to be introducing high-fat, high-sugar ‘nutrition’ supplements to these populations?” Bazzano et al. 2017, pg. 7.
- 73
As of 2021, we expect the marginal dollar we recommend will be about 10 or more times as cost-effective as GiveDirectly's unconditional cash transfer program. For an example of the cost-effectiveness of our recommendations, see this page.
- 74
See our cost-effectiveness analysis, “CEA - Standard CMAM” sheet, “CMAM vs cash” row.
- 75
For example, a 2016 IRC report detailed CMAM costs per child ranging from approximately $100 to nearly $500. International Rescue Committee, "Cost Efficiency Analysis: Treating Severe Acute Malnutrition," 2016, pg. 4.
- 76
In January 2021, ALIMA received a GiveWell Incubation Grant to support its program providing treatment of malnutrition and pediatric emergencies in Mirriah, Niger. We expect that part of this grant will be used to fund combined protocol CMAM as part of an RCT.
- 77
- Niger Need: “In Niger, 350,000 to 400,000 children are treated for SAM every year; ALIMA estimates that ideal coverage would require doubling this figure.” GiveWell's non-verbatim summary of a conversation with ALIMA, November 13, 2020, pgs. 1-2.
- Global Need: A 2010 World Bank report estimated $2.6B in additional funding is needed to treat SAM , without considering costs of treating MAM (Horton et al. 2010, pg. 31). This report used the optimistic assumption that SAM would fall by half because of successful prevention measures and estimated that treating 80% of SAM children would cost $2.6B more than already allocated. “Community-based management of severe acute malnutrition: This is an expensive intervention, which costs US$200 per child treated. The prevalence of severe acute malnutrition is 4.8 percent across the 36 countries in the 6–59 months age group (implying an incidence of 9.6 percent, using the incidence: prevalence ratio of 2:1). We assume that if all the other interventions are funded, that prevalence of severe acute malnutrition will fall to 50 percent of present levels (Isanaka et al. 2009, reporting on the effect of an intensive complementary feeding program). Unlike other interventions (where we aim for 100 percent coverage) we aim for 80 percent coverage, since there are no existing programs at scale achieving higher coverage, and we cost the intervention accordingly. Current coverage is approximately one million children (Stephane Doyon, Médecins Sans Frontières, personal communication). Additional annual cost = US$2.6 billion.” Horton et al. 2010, pg. 31.
- 78
The Combined Protocol for Acute Malnutrition Study (ComPAS) (Bailey et al. 2020) tested a protocol using MUAC (along with presence of edema) as the single criterion to diagnose acute malnutrition, determine dosage of RUTF and diagnose recovery in South Sudan and Kenya. The Optimizing treatment for acute MAlnutrition (OptiMA) protocol has been trialled in DRC with another trial planned for Niger and uses weight as well as MUAC (and presence of edema) to diagnose, determine dosage and discharge patients (Phelan 2019).
- 79
Our typical approach to cost-effectiveness does not include an adjustment for quality of life saved, nor are we certain that it should. However, in this case, it may be causing us to overvalue an intervention that is a shorter-term fix for children who remain in very difficult circumstances after treatment. The research team will continue to contend with these difficult moral questions as we examine this program further.
- 80
Most of the studies we have reviewed come from contexts where children are chronically malnourished, but we have not investigated how this is likely to affect the cost-effectiveness of the program. Our prior is that, in crisis settings, children are more likely to be able to weather malnutrition or infection in the absence of the program, so the program's impact will be smaller relative to the counterfactual. However, we also believe children would require fewer rounds of treatment on average to avoid death from malnutrition (as the period of malnutrition is shorter in a temporary crisis), so the program would be lower cost too.