mothers2mothers
GiveWell aims to find the best giving opportunities we can and recommend them to donors (why we recommend so few charities). We tend to put a lot of investigation into the organizations we find most promising, and de-prioritize others based on limited information. When we decide not to prioritize an organization, we try to create a brief writeup of our thoughts on that charity because we want to be as transparent as possible about our reasoning.
The following write-up should be viewed in this context: it explains why we determined that (for the time being), we won't be prioritizing the organization in question as a potential top charity. This write-up should not be taken as a "negative rating" of the charity. Rather, it is our attempt to be as clear as possible about the process by which we came to our top recommendations.
Published: March 2012
For an older version of this page, see our 2009 review of mothers2mothers.
Table of Contents
What do they do?
mothers2mothers works with women during pregnancy and after birth to improve adherence to interventions aimed at preventing mother-to-child transmission (PMTCT) of HIV. It trains and employs mentors who work with HIV-positive pregnant women to improve adherence to recommended interventions. The mentors are HIV-positive women who have previously received PMTCT care.1
Does it work?
Country-level analysis
We compared country-level data on pregnant women receiving antiretrovirals for PMTCT to mothers2mothers data on when it started working in a country and how many new clients it reached with its program. About this data:
- Country-level data is reported by countries to the World Health Organization.2 We present data for the 25 higher HIV burden countries (as of 2009).3 We have not investigated the quality of this data.
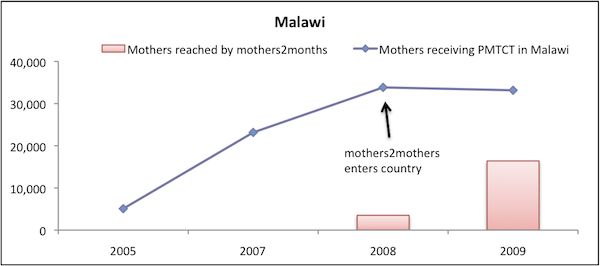
- We have only found mothers2mothers' data on new client numbers for 2009, with the exception of 2005 data from South Africa, and 2008 data from Malawi.4
- mothers2mothers reports, on its website, the year it started working in each of country.5
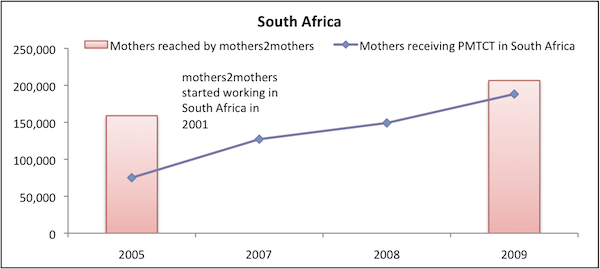
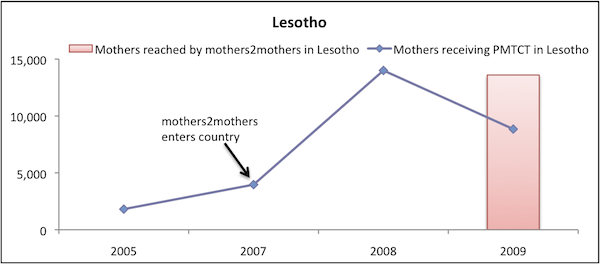
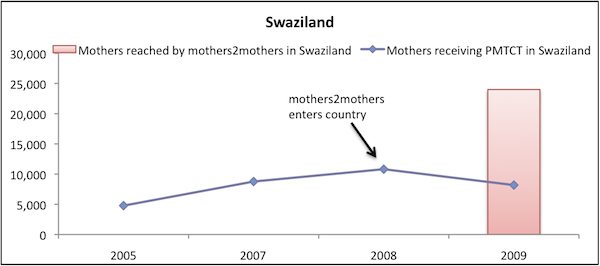
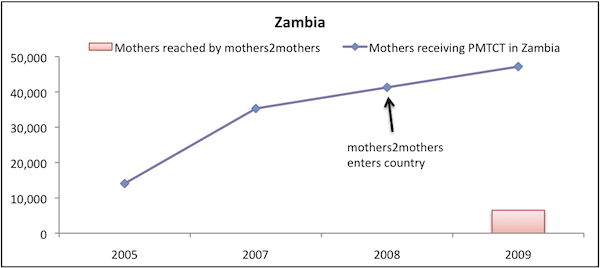
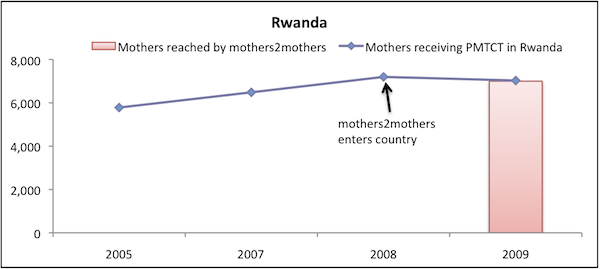
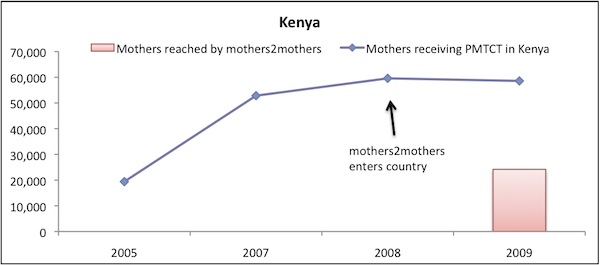
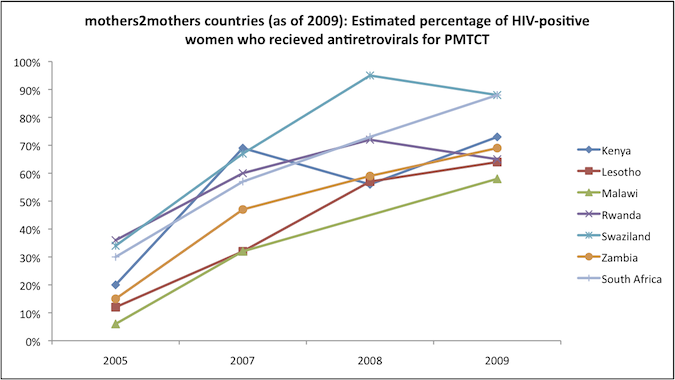
In most countries it works in, mothers2mothers' reported reach (i.e. number of new clients) rivals (or exceeds) the total number of women receiving antiretrovirals for PMTCT in the country. Given this extensive reach, if mothers2mothers' program is succeeding at increasing uptake of PMTCT, we could expect to detect this in country-level data. In the data shown below, we do not detect a country-level effect of mothers2mothers' program. In particular:
- Looking at the data from each of the countries mothers2mothers works in, it appears that (a) mothers2mothers's reported figures sometimes exceed the total country-wide figures reported by the WHO; (b) despite this, in most cases there do not appear to be significant improvements in trends of the WHO data following mothers2mothers's entry into a country.
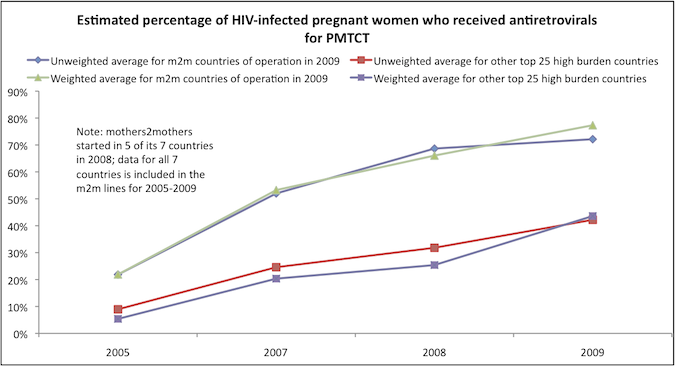
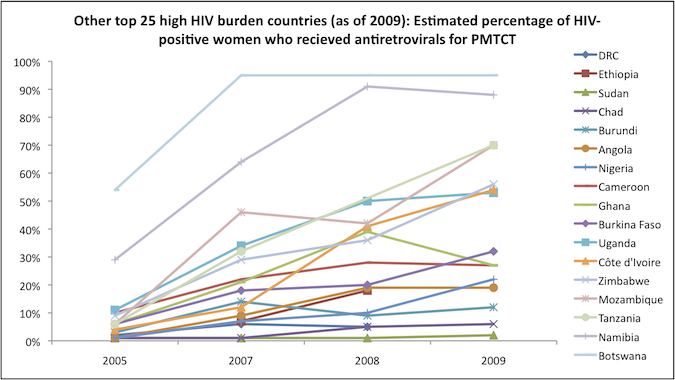
- There has been a positive trend in the estimated percentage of HIV-positive women who received PMTCT in the countries in which mothers2mothers was working in as of 2009 (note that it entered many of these countries in 2008). However, the trend in other high burden countries has also been positive, particularly in the southern African countries in which mothers2mothers does not work (Botswana, Mozambique, Namibia, and Zimbabwe, though less so in Angola).
We note that the group "mothers reached by mothers2mothers" is not necessarily a subset of "mothers receiving antiretrovirals for PMTCT in a country" because some mothers reached by mothers2mothers may not receive antiretrovirals for PMTCT. However, if the program is effective (and maybe even if it's not), we would expect a large proportion of mothers reached by mothers2mothers to receive antiretrovirals for PMTCT (as noted below, 83% of mothers not in the program and 93% of them in the program received PMTCT in mothers2mother's program evaluation).
mothers2mothers countries
Cross-country comparison
Independent evaluation
We reviewed an independent evaluation of the mothers2mothers program.6 The evaluation measured a number of factors,7 but we focus on evidence measuring the direct change in behavior: receipt and ingestion of the antiretroviral drug Nevirapine consistent with our take on what constitutes measurement of impact.
The evaluation focused on three health facilities in which mothers2mothers programs were located.8 Clinic providers identified women who might meet the eligibility criteria for the evaluation9 and selected both women who had engaged with mothers2mothers and those that did not.10 The study found a significant difference in the percentage of participants (93%) who had received and taken the drug vs. the percentage of non-participants (83%) who had received and taken the drug.11
However, like many studies evaluating charities' activities, this study appears to suffer from selection bias. There is no reason to believe that the women who participated in mothers2mothers programming are similar (in the ways that matter to drug uptake) to those who did not, and strong reason to believe that they may differ systematically. In particular, it seems highly likely to us that women who chose to participate in mothers2mothers are the same women who would be more likely to receive and take the appropriate drugs.
We therefore do not find this evaluation to be strong evidence regarding mothers2mothers' impact among pregnant women with HIV.
Sources
- Baek, Carolyn, et al. 2007. Key findings from an evaluation of the mothers2mothers program in KwaZulu-Natal, South Africa (PDF). Washington, DC: Population Council.
- GiveWell. Anti-retroviral therapy (ART) to prevent mother-to-child transmission (PMTCT) of HIV.
- GiveWell. Data on PMTCT and mothers2mothers' reach (XLS).
- mothers2mothers. Annual report (2005-2006) (PDF).
- mothers2mothers. Annual report (2008) (PDF).
- mothers2mothers. Annual report (2009) (PDF).
- mothers2mothers. History / Timeline. http://www.m2m.org/about-us/history-timeline.html (accessed July 4, 2011).
- mothers2mothers. The m2m model. http://www.m2m.org/what-we-do/the-m2m-model.html (accessed July 4, 2011). Archived by WebCite® at http://www.webcitation.org/5zvovIFON.
- World Health Organization. Towards universal access: Scaling up priority HIV/AIDS interventions in the health sector (2007) (PDF).
- World Health Organization. Towards universal access: Scaling up priority HIV/AIDS interventions in the health sector (2008) (PDF).
- World Health Organization,. Towards universal access: Scaling up priority HIV/AIDS interventions in the health sector (2009) (PDF).
- World Health Organization. Towards universal access: Scaling up priority HIV/AIDS interventions in the health sector (2010) (PDF).
- 1
"mothers2mothers offers an sustainable, scalable, and cost-effective solution to the challenge of providing PMTCT services in resource-limited settings. We do this by recruiting, training, and employing mothers living with HIV who have personally received PMTCT care. These women, Mentor Mothers, work side-by-side with doctors and nurses in health care facilities, and assume responsibility for ensuring that patients understand, accept, and adhere to interventions that are prescribed." mothers2mothers, "The m2m Model."
- 2
- World Health Organization, "Towards Universal Access: Scaling Up Priority HIV/AIDS Interventions in the Health Sector (2007)," Pgs 84-86, Annex 3.
- World Health Organization, "Towards Universal Access: Scaling Up Priority HIV/AIDS Interventions in the Health Sector (2008)," Pgs 130-132, Annex 3.
- World Health Organization, "Towards Universal Access: Scaling Up Priority HIV/AIDS Interventions in the Health Sector (2009)," Pgs 145-147, Annex 3.
- World Health Organization, "Towards Universal Access: Scaling Up Priority HIV/AIDS Interventions in the Health Sector (2010)," Pgs 128-131, Annex 5.
Data on estimated % of women receiving antiretrovirals for PMTCT is missing for 2007-2009 for India, so we have not included in the chart. Data is compiled, with citations, in GiveWell, "Data on PMTCT and mothers2mothers' Reach."
- 3
World Health Organization, "Towards Universal Access: Scaling Up Priority HIV/AIDS Interventions in the Health Sector (2010)," Pg 90. Data is compiled, with citations, in GiveWell, "Data on PMTCT and mothers2mothers' Reach."
- 4
All data on the number of mothers2mothers clients is from mothers2mothers, "Annual Report (2009)," Pg 8, with two exceptions. 2008 data from Malawi is from mothers2mothers, "Annual Report (2008)," Pg 14 and 2005 data from South Africa is from mothers2mothers, "Annual Report (2005-2006)," Pg 5. Data is compiled, with citations, in GiveWell, "Data on PMTCT and mothers2mothers' Reach."
- 5
mothers2mothers, "History / Timeline."
- 6
Baek 2007.
- 7
The factors were:
- "PMTCT knowledge
- Disclosure of HIV status
- Receipt and ingestion of Nevirapine [a drug used to prevent mother-to-child transmission of HIV]
- Infant feeding intentions and practices
- Family planing intentions and practices
- Referral and follow-up for care, and
- Psychosocial well-being of participants."
Baek 2007, Pg 8.
- 8
"There were three evaluation sites in the Pietermaritzburg area of KwaZulu-Natal. These sites drew women from urban and peri-urban settings." Baek 2007, Pg 1.
- 9
"Women were eligible for the study if they were between the ages of 18 and 49 years (inclusive) and they knew their HIV status. To participate in the study, pregnant women had to be between 6 and 9 months gestation. For new mothers, the eligibility criteria were slightly different at baseline (1–12 weeks postpartum) than at follow up (4–12 weeks postpartum). Clinic providers identified women who might qualify for the evaluation, briefly introduced the study to them, and referred them to the interviewers, who provided more information about the study." Baek 2007, Pg 8.
- 10
"The study examined how PMTCT knowledge and behaviors, and uptake of services changed over time (baseline to follow-up) and differed based on whether or not women participated in m2m activities. The m2m program considered a minimum of two contacts between a mentor mother and an antenatal or postpartum client to be programmatically meaningful; therefore, study respondents were considered program participants if they spoke with a mentor mother two or more times. The definition of a contact was broad; a contact could occur either before or after delivery, and could involve participation in a one-on-one interaction or a group session." Baek 2007, Pg 10.
- 11
Baek 2007, Pg 18.